Article Text

Abstract
Background ST-elevation myocardial infarction (STEMI) is a highly time-sensitive and life-threatening condition. Early recognition and timely management are challenging in a busy emergency department (ED), especially in low/middle-income countries where emergency systems are often fragmented. The aim of our quality improvement (QI) project was to increase the percentage of patients with STEMI undergoing primary percutaneous coronary intervention (PCI) with door to balloon (D2B) time of <90 min by 30% over 12 months.
Methods As part of the first step in QI, baseline data were collected at different points in the process of care. Using process maps and fishbone analysis, delays in patient registration, ECG and communication with cardiology were identified as some bottlenecks, and change ideas were tested using plan–do–study–act cycles using point-of-care QI methodology. The majority of the change ideas focused on interventions in the ED like strengthening triage, training frontline staff, early diagnosis and quick transportation of patients.
Results During the baseline phase, 22.22% of patients were found to have a D2B time of <90 min. We achieved an increase of 47.78% in patients receiving PCI within 90 min and hence increased to 70% at the end of the intervention phase. Data collected for 4 months after the intervention phase were found to have sustained the effort.
Conclusion Significant improvement in the door to reperfusion time resulted from a meticulous assessment of emergency care processes by drawing process flow chart and implementation of change ideas like introduction of fast-track policy for patients with chest pain, reducing staff turnover in the triage area, formal training of staff, continuous engagement with cardiology team and by interchanging of processes which led to a reduction in time to ECG.
- quality improvement
- emergency department
- time-to-treatment
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author, AK, upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
ST-elevation myocardial infarction (STEMI) is a life-threatening condition requiring timely management. The emergency care in low/middle-income countries (LMICs) is often fragmented. To achieve quality care of door to balloon (D2B) time of <90 min is a challenging task in LMICs.
WHAT THIS STUDY ADDS
In this quality improvement (QI) project, simple change ideas implemented using plan–do–study–act cycles were successful. This included both process and people changes. These change ideas improved the percentage of patients with STEMI having D2B of <90 min from a baseline of 22.22% to 70%. Data collected for 4 months after the intervention phase were found to have sustained the effort. This study demonstrates that simple change ideas using available resources can significantly improve emergency care in LMICs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Several problems in the emergency department (ED) can be addressed using simple QI methodology. We hope to introduce more EDs in LMICs and the South East Asian region in applying a similar process to improve the quality of their services for the benefit of patients particularly for time-sensitive conditions like STEMI, acute stroke, sepsis and trauma.
Introduction
The World Bank Disease Control Priorities Project estimates that about 40% of the disease burden and 50% of deaths in low/middle-income countries (LMICs) are directly related to lack of emergency services.1 Ischaemic heart disease is the leading cause of mortality in LMICs.2 ST-elevation myocardial infarction (STEMI) is one of the most time-sensitive and life-threatening diseases, commonly presented to the emergency department (ED).
Chest pain is one of the most common presenting reports in the ED.3 4 Only 8%–10% of patients with chest pain have cardiac ischaemic events.3 Non-life-threatening causes of chest pain are much more common than STEMI. Hence, early recognition and intervention in STEMI can be challenging in a busy ED. The American College of Cardiology/American Heart Association 2013 guidelines recommend that patients with STEMI presenting within 12 hours of symptom onset should have a door to balloon (D2B) time of fewer than 90 min.5
Several studies from LMICs mention the causes of delays in STEMI care.6–8 A state-wide government-led prehospital initiative in India improved STEMI care by strengthening transfer of patients to percutaneous coronary intervention (PCI)-capable hospitals using the hub and spoke model.9 Another study from India evaluated a fast-track protocol and reduced the door to thrombolysis time in patients with STEMI by 33 min.10 A quality improvement (QI) methodology has shown to improve processes in different clinical settings in the country.11–14A few successful QI projects published are reduction in waiting time outside the triage from 50 min to <30 min in an ED,11 improvements of hand hygiene in neonatal intensive care unit and prevention of hypothermia in preterm neonates.13 There is no published literature on reducing the D2B from India. Hence, we sought to replicate similar efforts in our in-hospital context to improve STEMI care. The project aimed to increase the percentage of patients with STEMI undergoing primary PCI with D2B time of <90 min by 30% in 12 months after the baseline phase.
Methods
Setting
Ours is a tertiary teaching hospital with an academic emergency medicine department. Our ED caters to more than 450 patients every day with a bed capacity of less than a hundred. We handle both medical and surgical cases of adult and paediatric in the ED. Trauma is handled in a separate building. During busy hours, it is common to see more than 50 patients waiting outside triage. We use a locally developed triage system—All India Institute of Medical Sciences (AIIMS) Triage Protocol in our ED.15 The average ED disposition time of our patients is more than 36 hours. All healthcare workers in the ED work in three shifts with approximately 20 doctors (3 post-MD, 5 postgraduate trainees in emergency medicine and 12 non-trainee junior doctors), 20 nursing staff members, 1 ECG technician, 15 security guards and up to 12 hospital attendants (HAs) in each shift. We have round-the-clock cardiology and PCI service at our centre.
The project was started after obtaining the institute’s ethical clearance. A QI team, including doctors, nurses, health assistants and security guards, was formed and the team was led by coauthor (BG). The project was supervised by a faculty in emergency medicine. All team members were trained in the point-of-care QI methodology developed by the South East Asian Regional WHO and the Department of Paediatrics of AIIMS, New Delhi.16
Patient and public involvement
There was no patient or public involvement in the design, conduct or reporting of this study.
Measurement
To standardise documentation before data collection, we replaced analogue clocks with digital clocks and made it compulsory for all residents to note the time on patients’ medical notes. A baseline phase was conducted for 2 months in which the team members collected data without intervention. The following data points were recorded.
Door time: the time the patient entered the triage room; obtained from the ED computerised registration paper, and triage slip after its implementation.
ECG time: printed on the ECG strip.
Cardiology communication time: noted from the telephone register in the ED maintained by the telephone operator.
Cardiology team time of evaluation: obtained from the emergency patient’s record sheet.
Balloon time: the time at which a stent was inserted into the coronary artery. These data were recorded from Picture Archiving and Communication System (PACS).
Understanding and analysing processes of care
The team used process mapping and fishbone analysis to identify causes for delays in emergency STEMI care. The change ideas were discussed by the team and tested. The change ideas were tested in four phases of 3 months each. Two to three change ideas were tested using plan–do–study–act (PDSA) cycles in each phase. Successful ideas were implemented. No patient was involved in the design, conduct or reporting of this study.
Process mapping was done by ‘shadowing the journey’ of five patients from the entry of the patient to the triage room until stenting in the cardiac catheterisation laboratory (cath lab) by the QI team members. The process of patient flow was drawn during a team meeting and divided into smaller processes according to the time intervals calculated. The meeting was attended by QI team members. Stakeholders involved are depicted in a map (figure 1). The major bottlenecks identified were delay in patient registration, delay in ECG and delay in communication with cardiology (figure 2).
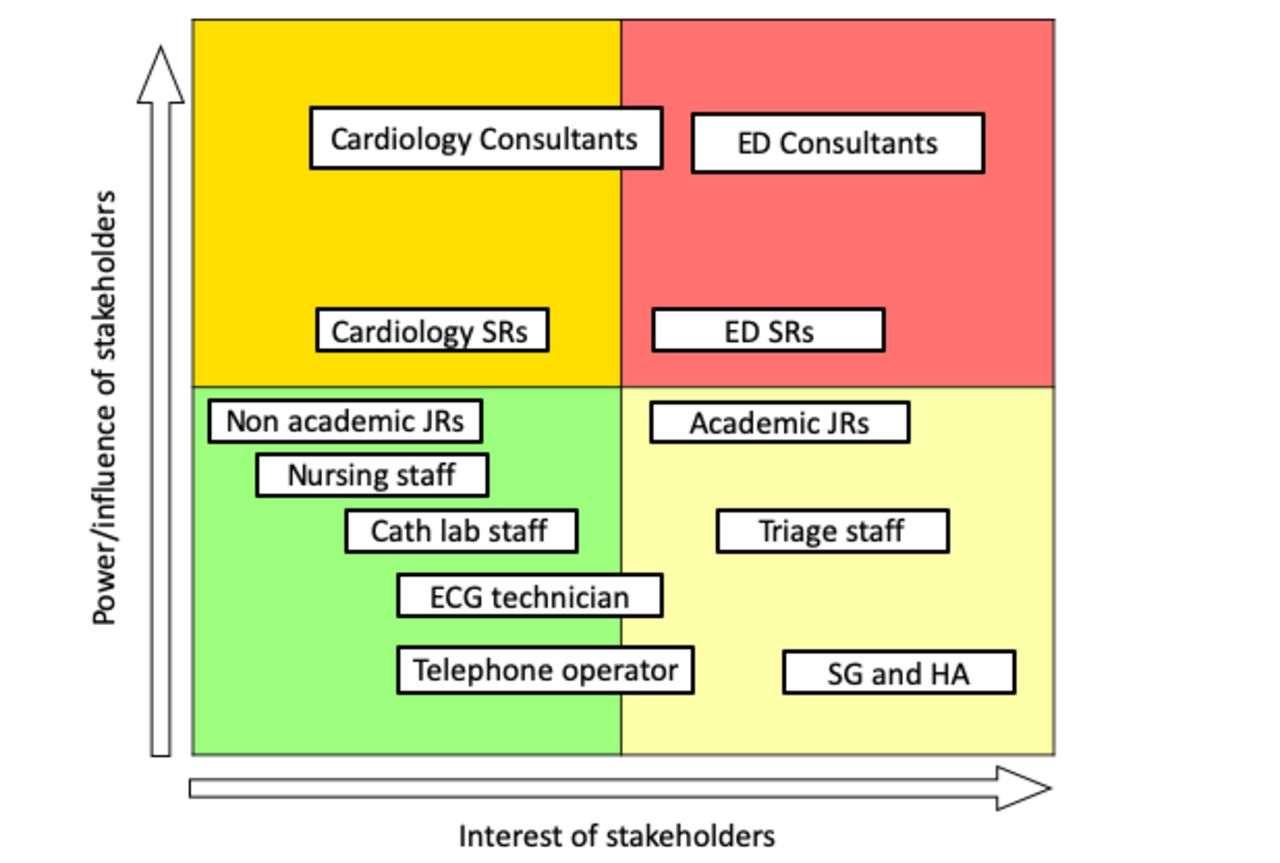
Stakeholder map. cath lab, catheterisation laboratory; ED, emergency department; HA, hospital attendant; JR, junior resident; SG, security guard; SR, senior resident.
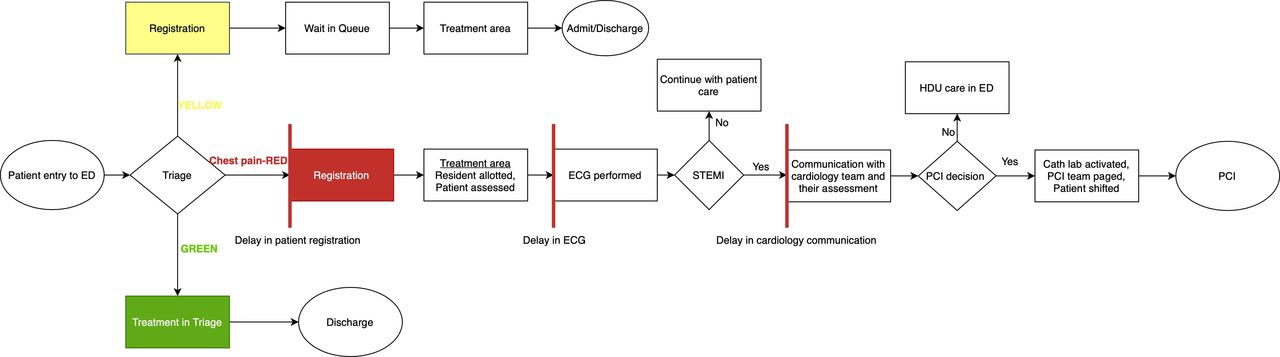
Process mapping with bottlenecks highlighted in vertical red lines. cath lab, catheterisation laboratory; ED, emergency department; HDU, high dependency unit; PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction.
All patients presenting to the ED enter through the triage area. Triage is performed by a triage team including a resident doctor and two nursing officers. The baseline process was as follows: all patients with chest pain were triaged as ‘red’ and transferred inside to the treatment area after registration at the emergency desk. In the treatment area, a resident was allotted who assessed the patient and requested an ECG. The junior resident discussed the case with the ED senior resident (post-MD/registrar) to confirm the diagnosis and initiate management. If STEMI was diagnosed, the patient was shifted to a high dependency unit within ED, initial medical therapy was given and the resident informed the cardiology team. The decision for PCI was made by the cardiology team. The cath lab was activated and the patient shifted. The radiographer uploaded all images on PACS after PCI (figure 2—baseline process flow chart with bottlenecks).
A fishbone analysis looking at all components of causes of delays was done during a team meeting after the baseline phase (table 1).
Fishbone analysis
Strategies
Change ideas were tested using PDSA cycles. Successfully tested ideas were adopted, adapted or abandoned. Our interventions mainly focused on system improvement within the ED. The interventions were decided based on the detailed study of the process mapping and identification of the bottlenecks. Some of the coauthors had experience with other projects in the same setting which helped us decide on the interventions quickly.11 Intervention phases included reducing the door to ECG time, streamlining STEMI detection and cardiology team activation time reducing transfer time to cath lab and faster STEMI diagnosis (figure 3).

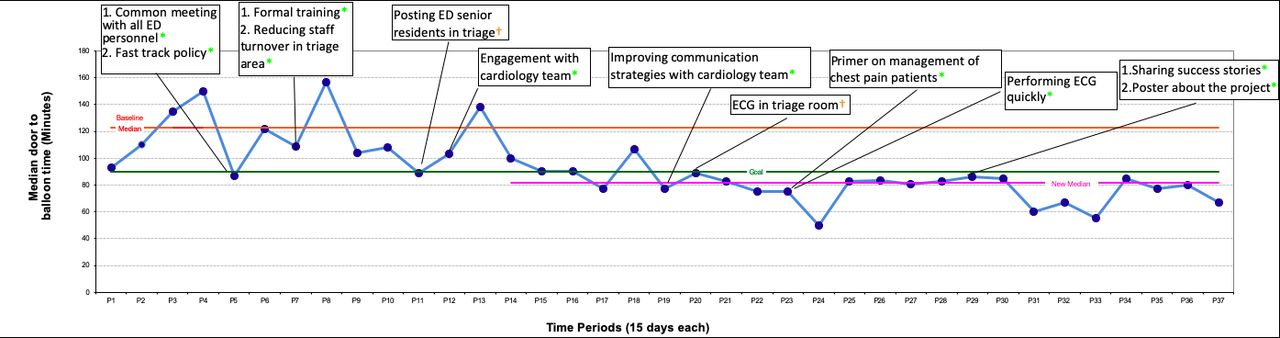
Run chart depicting the median door to balloon (D2B) time. Each data point on the X-axis represents consecutive periods of 15 days each (P). P1: 8 February–22 February 2018 and P37: 1 August–15 August 2019. Each data point on the Y-axis represents the median D2B time during 15 days. The baseline median (red line) D2B time was 122.5 min and the new median (pink line) was 81.7 min. The interventions have been captioned in the boxes. The ideas which worked and were implemented are marked in ‘green’. The ideas that did not work are marked in ‘orange’. ED, emergency department.
Intervention phase 1 (9 April–30 June 2018): reduce door to ECG time
A common meeting with all cadres of ED personnel
Three orientation sessions were conducted. Healthcare personnel of all cadres working in the ED, particularly posted in the triage area, attended them. This included residents, nurses, HAs and security guards. The meeting focused on creating awareness about the delay in care for patients with STEMI and why it is important to address this gap with emphasis on teamwork. We had discussions with the cardiology team during the same period. Result: the median door to ECG time reduced from baseline 20 min to 11 min over the 2-week period.
Fast-track policy for patients with chest pain
We developed a fast-track system for patients with chest pain where any patient who presented to the triage area with chest pain would be transferred to the treatment area with a hand-filled triage slip immediately without having to wait for emergency patient registration. During the same time, a dedicated route—‘red patient corridor’ for transport of ill patients between triage and treatment area—was also created and implemented. Short on-site training sessions (lasting less than 15 min) were organised early morning between 07:00 and 08:00 to help operationalise the fast-track system. The training sessions were held for 4 consecutive days so that staff working in all batches were covered. The fast-track system was tested and implemented in the afternoon shift. Result: the median door to ECG time, after both orientation sessions and fast-track policy, reduced from the baseline median of 20 to 8.5 min.
Formal training for triage staff
The security guards and HAs were trained to identify patients with chest pain waiting outside the ED to skip the waiting line and enter the triage area immediately. HAs were also involved in transferring patients to triage and treatment areas. A formal training programme which included a hands-on workshop on ‘basic life support’ was organised for this frontline emergency personnel on 2 days. They were primed to identify patients with chest pain and prioritise their transfer into triage area and from triage to the treatment area without delay. Result: the median door to ECG time was reduced to 7 min right after this intervention. A biweekly training roster for security personnel and HAs was created and followed.
Reducing staff turnover in triage and treatment area
World Health Assembly of the WHO stated that an important challenge in patient safety in emergency care is the lack of fixed staff.17 In our department, nursing staff and HAs were rotated in and out of triage frequently. Untrained staff posted in triage reduced process efficiency. This issue was addressed at a meeting of consultants and the nursing supervisor. Result: a plan was designed to fix the staff for a minimum period of 3 months and form a triage team comprising of doctors, nursing staff, HAs and security guards. The new triage team was formed a month later on 15 May 2018. This helped us in better implementation of the change ideas.
Intervention phase 2 (1 July–30 Sept 2018): streamlining STEMI detection and cardiology team activation time
Posting ED senior residents in triage
We posted ED senior residents in triage area to help streamline chest pain service. This change was tried in the morning and afternoon shifts for a day. It was not feasible to post senior residents in triage as the treatment area suffered from no senior person on the floor. Hence, the change idea was abandoned.
Constant engagement with the cardiology team
Cardiology residents new to the system would unknowingly delay care for patients with STEMI as was evident during the period of 7–21 August 2018, it took a median of 100 min for PCI after the cardiology resident assessment. Several brief discussions with the cardiology team focusing on streamlining processes for improved care in patients with STEMI were organised. Every patient who missed the window period was discussed with the cardiology team and the cause for the delay was identified and fixed. Result: during the period of 22 August and 5 September 2018, median cardiology resident assessment to PCI time was reduced to 55 min.
Intervention phase 3 (1 October 2018–31 December 2018): reducing transfer time to the cath lab
Improving communication strategies with the cardiology team
It was not always easy to communicate with the cardiology resident on call over the mobile phone. A new standard operating procedure (SOP) was introduced to contact the cardiology ward or cath lab directly on landline numbers. The numbers were made available and incorporated in the ED telephone directory. Result: this led to faster delivery of information. There was a significant reduction in time to communicate with the cardiology team from a median time of 13 min in mid-November to 6 min between 20 November and 4 December 2018.
Performing ECG in the triage room
Having an ECG machine in the triage room was thought to reduce the door to ECG time even further. An ECG machine was kept in the triage room on 3 December 2018. But due to crowding in triage and difficulty in handling two separate areas by the same ECG technician, the idea was not feasible and the change idea was abandoned.
Intervention phase 4 (1 January–31 March 2019): faster STEMI diagnosis
A primer on the management of chest pain
A new batch of residents joined in the first week of January 2019. A training programme was organised to introduce them to the functioning of the department and particularly the management of time-sensitive conditions including patients with chest pain. The programme was held on 10 and 14 January 2019. Result: door to ECG time remained less than 10 min and median D2B time was 75 min between 4 and 18 January.
Performing ECG quickly
To perform a quick ECG in patients with chest pain, the HA was asked to get the ECG done before handing over the patient to the resident. This quickened the process of STEMI diagnosis and reduced ED to cardiology communication time. The change idea was tested in the first week of January 2019. The median door to ECG time and door to cardiology communication time were 9 min and 20 min, respectively, during the data point of 4 January–18 January 2019. Result: the door to ECG time and cardiology communication time reduced further to 6 min and 12.5 min, respectively, in the next 2 weeks.
Data analysis
The outcome measure was D2B time. Process measures were door to ECG time, door to cardiology communication time and door to cardiology team assessment time. Balancing measure was the occasional overcrowding in the treatment area during peak hours resulting from several patients with chest pain triaged in a short period. We plotted the data points on a run chart for analysis. We used the median values as it is less influenced by outliers compared with the mean. When a shift was identified, the median was recalculated. A shift is defined as ≥6 consecutive data points on the same side of the median.18 We calculated the baseline median from 8 February to 8 April 2018.
Sustainability
Efforts were made to sustain the improvement achieved during 1 year of intervention. We collected data for 4.5 months after the last intervention. Both process and people changes were addressed as described below.
Poster about the QI project in the emergency
A poster was displayed in the ED showcasing improvements achieved during the study period. This positive message with pictures of ED staff on the wall was good to motivate the staff.
Sharing success stories
Success and failures encountered during the run of the project were shared with the team and other staff at large during departmental meetings. Health workers working in the respective areas were allowed to express views about the project, the problems faced and lessons learnt. Active team members were appreciated for their hard work by senior consultants and honouring them with a special certificate from the department.
We do not have data after the post-intervention phase due to the COVID-19 pandemic. Our institute does not have electronic health records for the data points collected in this study.
Overall results
In the baseline data from 9 February to 8 April 2018, only 4 out of 18 patients with STEMI who underwent PCI had D2B time of <90 min, that is, 22.22%. The baseline median D2B time was 122.5 min (IQR, 33 min). At the end of intervention phase 4, 70% (21 out of 30) of patients with STEMI underwent PCI within 90 min. In the data collected during the sustainability phase, 70% (42 out of 60) of patients with STEMI had D2B time of fewer than 90 min as compared with the baseline of 22.22%. A shift was identified from 22 August to 5 September 2018 data point and the new median calculated after that was 81.7 min (IQR, 10 min). The run chart is depicted in figure 3. The revised process map after interventions is depicted in figure 4. The individual results are described in the strategies section along with the description of each change idea.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
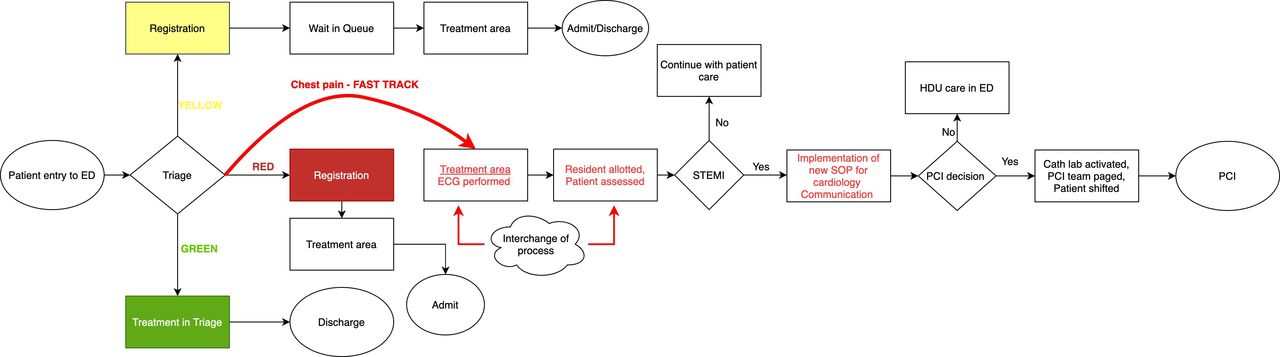
Revised process mapping after interventions. The successful process change ideas are highlighted in ‘red’. cath lab, catheterisation laboratory; ED, emergency department; HDU, high dependency unit; PCI, percutaneous coronary intervention; SOP, standard operating procedure; STEMI, ST-elevation myocardial infarction.
Challenges and lessons learnt
Building systems of care and streamlining STEMI management are daunting tasks considering the heavy patient load and lack of adequate space within the ED. Although the American Academy of Emergency Medicine recommends patient to nursing staff ratio of 3:1,19 the patient to nursing staff ratio in red and observation areas of our department are 8:1 and 12:1, respectively. It is even worse during the night shifts (due to the posting of fewer nursing staff members at night). Patient to doctor ratio is also poor, with 6:1 in red areas and 15:1 in observation areas. Being a tertiary care referral centre, approximately one-fourth of all patients received are severely ill, triaged red and require early assessment and management. It was not possible for us to increase the triage staffing levels. However, by working on other low hanging opportunities such as minimising staff turnover, providing support with knowledge and skill development and eliminating wasteful steps, we were able to reduce waiting time for patients with chest pain.
Lack of knowledge about QI among emergency healthcare workers was one of the biggest challenges in conducting QI. Most of our staff never expected that the workplace could get better. They were not ready to accept new changes in the system. By repeatedly motivating the staff that change could happen through the combined effort and giving examples of successful QI projects of maternal and child care health in the institute, we were able to convince our staff to test the change ideas.
Although we are an academic department with 40 academic residents, due to their posting in different departments as part of their academic training, only three to four MD academic residents would be posted in ED in one shift at a time. Hence, non-academic residents make up 90% of the doctor strength in ED. This group of residents is appointed on an ad hoc basis for a period of 3–6 months. New residents would be naïve to the system and sometimes also lacked sufficient knowledge; nurses on the other hand were randomly posted in different areas of the ED. Hence, the whole process had to be repeatedly taught, making it an uphill task to initiate and sustain change ideas. This is by the WHO report, which states the lack of fixed staff compromises patient safety.17 Shift duties made it more cumbersome to communicate with all members of the staff effectively. It was a challenge to organise formal classroom training sessions. Conducting short on-site sessions on multiple occasions for smaller groups was an effective way to ensure the implementation of change ideas in all shifts. We introduced an ongoing induction programme for all newly joined residents every 3–6 months to orient and educate them about ED functioning and the QI project.
We have worked on both system-related and people-related changes in the project. The system-related change ideas which we tested were fast-track protocol (skipping the patient registration at the triage and red patient corridor): new communication SOPs with the cardiology team, posting ED senior resident in triage and performing ECG in triage. The first two change ideas were successfully implemented. People-related change ideas were orientation sessions, training the triage staff and discussions with cardiology team. To sustain the people-related change ideas, a few options we tried were: reducing the staff turnover in the triage and treatment room, biweekly training roster for security personnel and HAs, displaying posters in the ED and sharing success stories during departmental meetings. The activities performed to improve skills and knowledge were one-time activities. We are currently in the process of determining how to make training for STEMI a routine part of the system.
The shift obtained on the run chart at period 13 (figure 3) is a combined effort of engagement with the cardiology team, formal staff training and reducing staff turnover. Following this, other interventions did not result in special cause variation probably because of the constant changes in the population and difficulties in the system.
A QI project has been published in the same setting, which coincided with the improvement phase of this study.11 The published QI project reduced the waiting of patients outside the triage area from 50 min to <30 min. This led to faster entry of patients into the triage area. However, this present QI started with the ‘door time’ as entry to the triage room. One change idea was common to both the projects: reducing staff turnover in the triage room. The concept of the change ideas like on-site training of staff and orientation sessions of the two studies were interdependent and the change ideas were decided quickly based on the improvement seen in one project.
Data collection was a big problem in our setting. We had to establish a data collection system in the ED for this project, as there was no existing system of regular data collection. It was only after a year into the study that data collection was commenced by dedicated data entry operators.
Fast tracking of all patients with chest pain led to occasional overcrowding in the treatment area. To counter this, we transferred these patients to the yellow queue after life-threatening causes of chest pain were ruled out based on history, clinical examination and point-of-care tests.
Administrative support and proactive leadership are important for conducting the study, especially in LMICs. Support from senior faculty and administrators to conduct a QI project positively impacts the working environment. Sharing of success stories and appreciation of frontline staff by senior consultants ensured the sustainability of the results achieved and involvement in more QI initiatives.
Limitations
Specific change ideas which worked for us may not work for other EDs as many factors are contextual. It was not always possible to test each change idea one by one and hence which change idea worked may not always be clear. The activities performed to improve skills and knowledge were one-time activities. We are currently in the process of determining how to make regular training and skills development for STEMI a routine part of the system. This will help sustain improvement over time even as new staff join the ED. There is also the issue of the processes reverting to previous ones as the project ends. By ensuring audits and regular supervision of vital quality indicators, the department can maintain quality in time-driven conditions.
Implications
Significant improvement in door to reperfusion time resulted from meticulous assessment of emergency care processes by drawing process flow chart and implementation of change ideas like introduction of fast-track policy for time-sensitive conditions, reducing staff turnover in the triage area, formal training of staff, continuous engagement with cardiology team and by minor interchanging of processes which led to a reduction in time to ECG.
ED services have received little attention in LMICs. ED functioning impacts the whole hospital and can have immediate impacts on health outcomes. Improvement of quality, efficiency, access and administration of timely emergency services can reduce mortality by 45% and disability by 36% in LMICs.20 Often young patients with no comorbidities seek emergency care in LMICs.21 This observation also tallies with the general population that we see in our adult ED. Therefore, interventions to decrease mortality and morbidity in emergency settings of LMICs could dramatically increase life-years saved.
Many hospitals, particularly large volume public sector healthcare facilities, face similar problems like ours. We encourage EDs to use available QI resources and expertise from other parts of the hospital or health system to streamline processes of care. Specific factors leading to delays and change ideas will vary in other contexts. However, the QI methodology of identifying a problem and writing a specific aim, forming a frontline team, determining measurement methods, analysing processes and testing change ideas to resolve the problem can be followed in other settings too.
Several problems in the ED can be addressed using simple QI methodology.11 We hope to introduce and guide more EDs in the region in applying a similar process to improve the quality of their services for the benefit of patients particularly for time-sensitive conditions like STEMI, acute stroke, sepsis and trauma. We recommend integrating QI initiatives into the residency programme in LMICs so that healthcare professionals are aware of this science right from their training days. We urge international organisations, national governments and policymakers to initiate and scale up QI efforts to improve emergency care services in LMICs.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author, AK, upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Institutional ethics committee approval was obtained (IECPG-530/20.12.2017, RT 35/31.10.2018).
Footnotes
Twitter @akshay21111
Contributors BG was the resident who led the project under AK. RS, SB, NJ, ME and PA mentored BG and provided inputs during the entire project. SB, NJ, ME, PA and AD were an integral part of the QI team and were actively involved in discussions and formulating new change idea. RS, AD, BB and VK helped in the implementation of change ideas. SB, ME and AD helped in data analysis. All authors have contributed and have edited the manuscript. BG is the guarantor and accepts full responsibility of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. Publication of this article is made Open Access with funding from the Nationwide Quality of Care Network.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.