Article Text

Abstract
Complications can occur anytime during pregnancy and childbirth. Pregnancies associated with high-risk factors have a higher-than-normal risk for fetomaternal complications. Bhagwan Mahavir hospital is a public sector hospital catering to low-risk and high-risk pregnant women (PW) in the labour room (LR)). The obstetrics and gynaecology team observed that at times the LR team failed to identify high-risk pregnancy (HRP) during admission in LR and to manage complications timely and efficiently. Therefore, the team started a quality improvement (QI) project in January 2019 with the aim to admit preidentified HRP in LR from existing 0% to 80% in 3 months.
The QI team followed the point-of-care quality improvement methodology to conduct this improvement process. They identified HRP in the outpatient department (OPD) during their antenatal care (ANC) visits, mentioned an HRP number on their ANC cards, and did risk stratification with yellow and red stickers into moderate and severe HRP respectively. Preidentified HRP were attended, admitted and managed on priority in the LR. The team achieved its aim in the ninth week of the QI initiative and sustaining to date. The team also measured and analysed the type of HRP identified in OPD, complications occurring around the process of childbirth in LR, maternal near-miss, maternal death and PW referred out from LR. They observed a 6.5%-point reduction (68.93%) in the median complication rate of major life-threatening complications following this improvement process.
This new intervention facilitated the team in early initiation of management of HRP in OPD, their triaging in LR, preparedness towards managing complications, involvement of support staff, PW and their relatives in the patient care, and redistribution of human resources according to priority area. The lessons learnt are generalisable and can be used in other facilities with similar settings.
- Quality improvement
- PDSA
- Control charts/Run charts
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
All pregnancies especially high-risk pregnancies (HRP) are at potential risk of complications during pregnancy and childbirth.
Early identification, risk stratification and management of HRP improve pregnancy outcomes.
What this study adds?
The team followed the point-of-care quality improvement methodology with available human resources to identify HRP and used colour codes for risk stratification.
This intervention helped the team in early identification and management of HRP in antenatal clinic, their triaging in labour room, preparedness towards managing complications and redistribution of human resources according to priority area.
How this study might affect research, practice or policy?
The lessons learnt are generalisable and can be used in other facilities with similar settings to improve patient care at different levels without additional human resources or financial support.
Problem
Pregnancy and childbirth are considered physiological processes and most pregnancies and childbirth worldwide are uneventful. However, all pregnancies are at risk anytime during pregnancy, childbirth and thereafter. Complications can occur anytime during pregnancy and childbirth, which in turn can affect the health and the overall survival of the mother and the fetus. Almost 15% of all pregnant women (PW) can develop potentially life-threatening complications which might require skilled care with some requiring major intervention for survival.1
Bhagwan Mahavir (BM) hospital is a 250-bedded secondary care public sector hospital in the north-west district of Delhi, India. It caters to low and lower-middle socioeconomic populations from the surrounding area. This hospital provides round-the-clock essential and emergency obstetrics and newborn care services in the labour room (LR). The median delivery per month is 317. The LR receives PW from its antenatal care (ANC) OPD, nearby primary healthcare centres and PW referred from other secondary care and private sector hospitals. The PW delivering at LR consists of both low-risk and high-risk pregnancy (HRP). The LR team manages most of the HRP and refers them to a tertiary care centre only in cases of pregnancy associated with medical disorders like cardiac disease, chronic renal disease, acute renal failure, etc requiring super specialised treatment, with disseminated intravascular coagulopathy requiring massive blood and blood component transfusion, with an extremely premature baby, and baby requiring in-utero treatment. This hospital has an emergency and an elective operation theatre, 10-bedded neonatal intensive care unit (NICU) adjacent to LR, a 12-bedded common ICU and a blood bank. The blood bank does not prepare blood components hence arranges from nearby tertiary care centres.
In LR, one postgraduate senior resident (SR), one undergraduate junior resident (JR) doctor and two staff nurses (SN) in a shift provide all the services. These include labour monitoring, conducting vaginal and caesarean section (CS) delivery and other emergency operative services, and follow-up of mothers after delivery. All deliveries, including vaginal deliveries, are conducted by doctors. SN does not conduct vaginal delivery in this hospital. When the SR goes to OT for any surgical procedure, LR is left with the JR and the SN. In such a situation, before implementation of this quality improvement (QI) process, many a time the JR on duty could not identify an HRP and failed to provide appropriate care around birth to a high-risk PW. There was no process of triaging of PW in the LR. The HRPs were not preidentified or screened during ANC visits. The LR team was failing to anticipate and manage complications timely and efficiently especially in the absence of SR on duty in the LR. The preparedness to manage complications timely and efficiently was poor as they were unanticipated. This was an important concern and a challenge to provide quality healthcare services and safe delivery to the PW attending LR of BM hospital and to give them a good childbirth experience.
In the meantime, the obstetrics and gynaecology (OBGYN) department of BM hospital got the opportunity to participate in a hub and spoke model of a QI project.2 As a participant, the OBGYN team decided to address this problem through QI methodology and started a QI project with an aim to admit preidentified HRP in LR from existing 0% to 80% in 3 months (from 1 January 2019 to 31 March 2019).
Background
All pregnancies are at potential risk of complications during pregnancy and childbirth. The WHO has reported that almost 830 women die daily because of complications during the antenatal period and childbirth.3 There are five main reasons for the death of PW such as severe haemorrhage, maternal infections, unsafe abortion, hypertension-related disorders of pregnancy such as pre-eclampsia and eclampsia, and medical complications such as cardiac conditions, HIV/AIDS or diabetes complicating or complicated by pregnancy.3
An HRP is associated with an actual or potential risk to the mother or the fetus. HRP is defined as pregnancy with pre-existing or current conditions that put the mother, the fetus, and the newborn baby at higher-than-normal risk for complications during or after the pregnancy and childbirth.4 These include very young and older women and those with previous or current medical and obstetric complications.3 The chances of pregnancy-related complications are more in HRPs.5 6 The presence of comorbidities among PW significantly increase the risk of progression to severe maternal morbidity (SMM).7 A systematic review of SMM found that the most common preventable factors in SMM cases were provider-related, specifically, a failure to identify ‘high-risk’ status and delays in diagnosis and treatment.8
Worldwide, 10%–30% of pregnancies are estimated to be ‘at-risk’. In India, about 20%–30% of pregnancies belong to the high-risk category.9 10 Identification and management of HRP initially and throughout pregnancy improve pregnancy outcomes for the mother and the newborn.9–13 Hence, all pregnancies need to be evaluated for associated high risks through routine ANC provided by healthcare professionals. Early identification of HRP flags PW who need clinical attention.14 The prognosis of the HRP also depends on its severity. HRP has been categorised into mild, moderate and severe HRP according to the associated high-risk factors. Several risk scoring systems and risk stratification using colour codes have been used to categorise HRP.15–17 The risk factors are based on past obstetric history, present pregnancy, medical and surgical illnesses, and each factor is assigned a score proportional to the degree of risk.18
Baseline measurement
A consultant and an SR from the OBGYN team collected the baseline data regarding HRP delivery and complications from the available records in LR. The birth register included records of all deliveries conducted in BM hospital including complications. In the birth register, the diagnosis included all the important key variables like parity, number of fetuses, gestational age, fetal presentation and any associated high risk. They collected the number of HRP delivered in LR in the last month (Decmber 2018). This was 32% of the total delivery. The median complication rate of major life-threatening complications like antepartum haemorrhage (APH), postpartum haemorrhage (PPH) and severe pre-eclampsia/eclampsia during pregnancy and childbirth in the last 6 months of the year 2018 was 9.43%.
The OBGYN team decided to record the percentage of preidentified HRP admitted in LR out of total HRP delivery as the process measure. Another process measure was to record all preidentified HRP in ANC OPD to know the type of HRP coming to BM hospital.
As an outcome measure, the team decided to keep a record of the percentage of major life-threatening complications (APH, PPH, severe pre-eclampsia/eclampsia), maternal near-miss, and maternal death to observe any improvement in these indicators following implementation of this QI initiative.
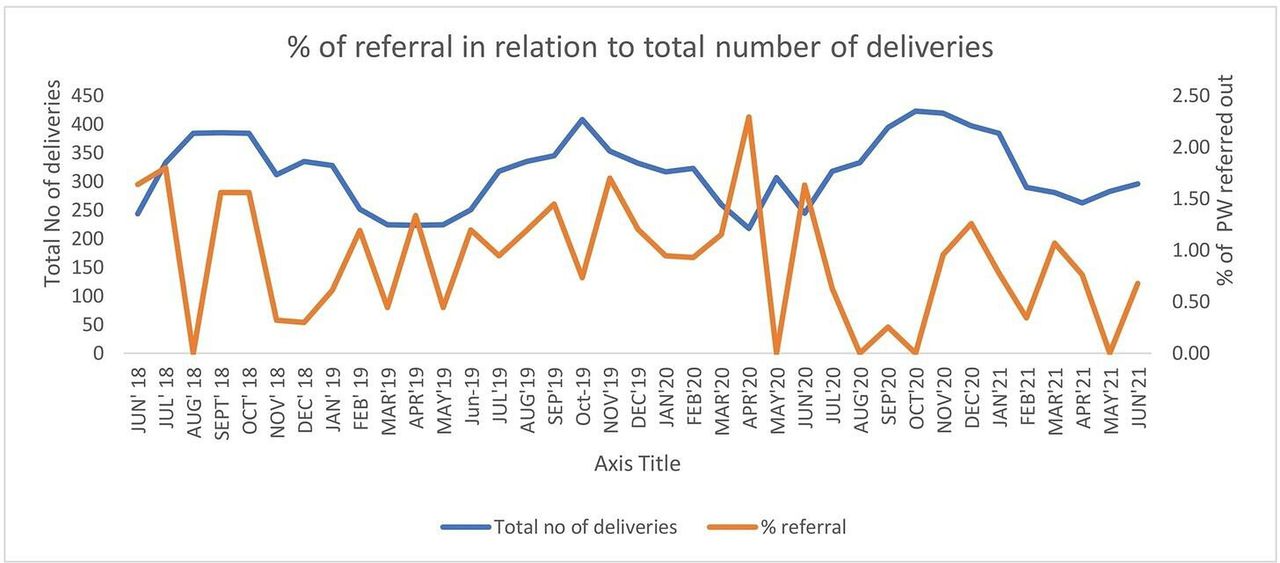
The number of PW referred out to tertiary care centre from LR was taken as the balancing indicator to assess the impact on the referral of PW.
Design
The OBGYN team followed the Point of Care Quality improvement (POCQI) methodology19 to conduct this improvement process. An external QI coach from Nationwide Quality of Care Network, India, and a QI trained consultant oriented the doctors and SN posted in the department about the QI methodology. A QI team was formed involving consultants, resident doctors, and SN from LR and OPD. The QI team conducted brainstorming sessions and used process flow chart and fishbone analysis to analyse the problem of HRP being admitted in LR without being preidentified and to find out possible change ideas to bring an improvement.
Process flow chart showed that at the time of admission duty doctors were not screening the PW according to HRP. They were not highlighting the PW as HRP which they identified during history taking and examination. There was no communication between duty doctors and SN regarding HRP admitted in LR. JR and SN were not giving handover of HRP specifically during their shift change. After delivery HRP were shifted to the ward and discharged without being highlighted. Thus, the HRP were identified, managed and discharged mostly at the level of SR and consultants. There was no involvement of JR, SN and support staff in the management of HRP leading to unanticipated fetomaternal complications.
Fishbone analysis of the problem (figure 1) showed that there was no awareness among doctors and SN about the importance of highlighting HRPs during admission in the hospital and the involvement of JR, SN and other support staff in the management as a team. There was no process or policy to triage PW at the time of admission in LR, to identify HRP in OPD during their ANC visits and to highlight HRP during hospital stay.

Fishbone analysis of the problem. HRP, high-risk pregnancy; JR, junior resident; LR, labour room; OPD, outpatient department; SN, staff nurse.
The QI team decided to orient the staff of OPD and LR, especially the JR and SN about HRP, the importance of their preidentification and their role in the management of an HRP. Also, to identify HRP in OPD during ANC visits, to give them an HRP number on ANC card and to record all HRPs in the HRP register. SR and JR in LR to look for the HRP number on each ANC card at the time of admission for triaging and to mark it as HRP in the case sheet. The SN to write the HRP number from the case sheet in the admission and birth register along with the diagnosis. To record the complications occurring in any PW admitted in LR, including the low risk, in the complication register as before. The team designed this process to initiate the specific treatment of an HRP early in OPD and to refer timely to a higher centre if needed. Also to facilitate the LR team in triaging the HRPs during admission by looking at the HRP number in the ANC card, recording the number of preidentified HRP delivered in LR, and giving hand over of HRPs during shift change.
The SR in the team from OPD and LR will collect the data for analysis from OPD and LR, respectively. The team decided to analyse data for the percentage of preidentified HRP admitted in LR weekly. The denominator would be the total number of HRP delivery conducted in the facility. The team further decided to analyse the data for the type of HRP identified in OPD, complications occurring around the process of childbirth in LR, maternal near-miss, maternal death and PW referred out from LR on monthly basis. The team met weekly to evaluate the progress and to identify ways to improve the preidentification of HRP and their management.
Strategy
The QI team arranged orientation sessions and invited the doctors and SN posted in OPD and LR to orient them about HRP, the importance of early identification of HRP in ANC OPD, triaging of PW in LR at the time of admission, their role in the management of an HRP and the basics of QI methodology. These sessions were conducted repeatedly to orient all staff posted in the department.
The team started the QI intervention in the ANC OPD. In BM hospital, ANC OPDs are conducted on every alternate day (Monday/Wednesday/Friday). There are four OPD rooms. In each room one consultant and one SR attends the PW coming to the OPD. They kept a list of HRP in all OPD rooms to identify HRP based on their clinical history and examination. The consultant supervised that SR is correctly picking up all HRP. A similar list was kept in LR also. The LR team followed these preidentified HRPs to facilitate triaging in LR and to calculate the percentage of preidentified HRP admitted. All PW attending the ANC OPD and admitted in LR for delivery were included in the study. The PW admitted in LR were from own ANC OPD (booked PW) and directly coming to LR for the first time (unbooked PW). Consultants, resident doctors and SN working in LR and OPD were involved in the documentation and monitoring of data, conducting plan–do–study–act (PDSA) cycles, and execution of change ideas after testing them. Later, the team also involved support staff, a nursing orderly (NO) from OPD and, a security guard (SG) from LR in the team. The support staffs were explained about the ongoing improvement process and their role in the management of HRP. The team conducted a series of PDSA cycles in the OPD and LR to test the change ideas as described in table 1.
Plan-Do-Study-Act (PDSA) cycles
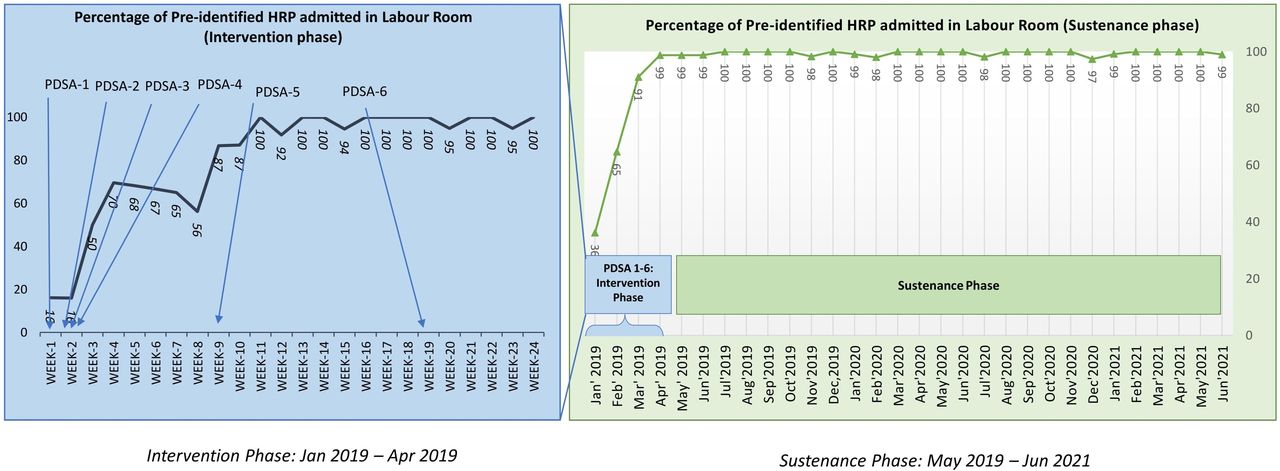
Through PDSA cycles 1–3 in OPD, the QI team streamlined the process of identification of HRP in OPD and giving an HRP number. PDSA cycles 4–6 helped the team in triaging the HRPs in LR. In PDSA 7, the team redistributed the available human resources and posted one additional SR in LR to support the LR team.
The SR in the team from OPD and LR collected weekly data for the total number of deliveries, the total number of HRP delivery and the total number of preidentified HRP admitted in LR. For the first 6 months, the team collected and analysed the data weekly and thereafter at the monthly intervals in the sustenance phase.
They also collected monthly data of HRP identified in OPD, major life-threatening complications, maternal near-miss, maternal death and PW referred out from LR. The data were entered in a Microsoft Excel spreadsheet for compilation, analysis and comparison. The team used run charts to display and interpret the serial measurement of process and outcome indicators and to study the impact of changes. They analysed the data whenever there was a shift in the median.20 21
To sustain this improvement process, the QI team had representatives of all the stakeholders and frontline staff including the support staff. The POCQI learner’s manual19 was kept handy and the team members revised the concepts of POCQI whenever required. The external QI coach and the QI trained consultant were there to support and guide the team. The members build up a good rapport with each other in the team. The doctors in the team understood the importance of communication with SN and support staff. The team met regularly to identify ways to improve and sustain the QI project. Successes were celebrated and failures were discussed in these QI meetings. The team members, especially the support staff, were appreciated for their efforts. This helped the team to continue the work with the same enthusiasm and motivation. They shared the successful change ideas with other staff of the department and invited their inputs for further improvement and sustenance. The successful change ideas tested in PDSA cycles were implemented in the routine processes as the new way of working. The new doctors and staff joining the department were oriented about this improvement process at the earliest. The stickers were not very costly and were procured online with imprest money. The leaders at all levels were kept in the loop and informed since starting and no leaderships issues were encountered. Eventually, this system change has become the routine of providing services in the facility. The SRs are collecting and analysing the data monthly along with other monthly censuses as per their roster under the supervision of consultants.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct or reporting, of this report. The objective of the study was to provide quality care to HRPs and their triaging to reduce complications during pregnancy, childbirth and thereafter.
Results
The total delivery in LR between January 2019 and June 2021 was 9347. During this period, the median HRP delivery was 33% out of which 34% were severe HRP delivery and 66% were moderate HRP delivery.
The QI team achieved its aim in the ninth week of the QI initiative and sustaining to date. The average preidentified HRP was 38% in the first 4 weeks, 64% in the next 4 weeks and 87% in the ninth week. Run chart showing percentrage of preidentified HRP admitted in LR (figure 2).

Run chart showing % of preidentified HRP admitted in LR. HRP, high-risk pregnancy; LR, labour room; PDSA, plan–do–study–act.
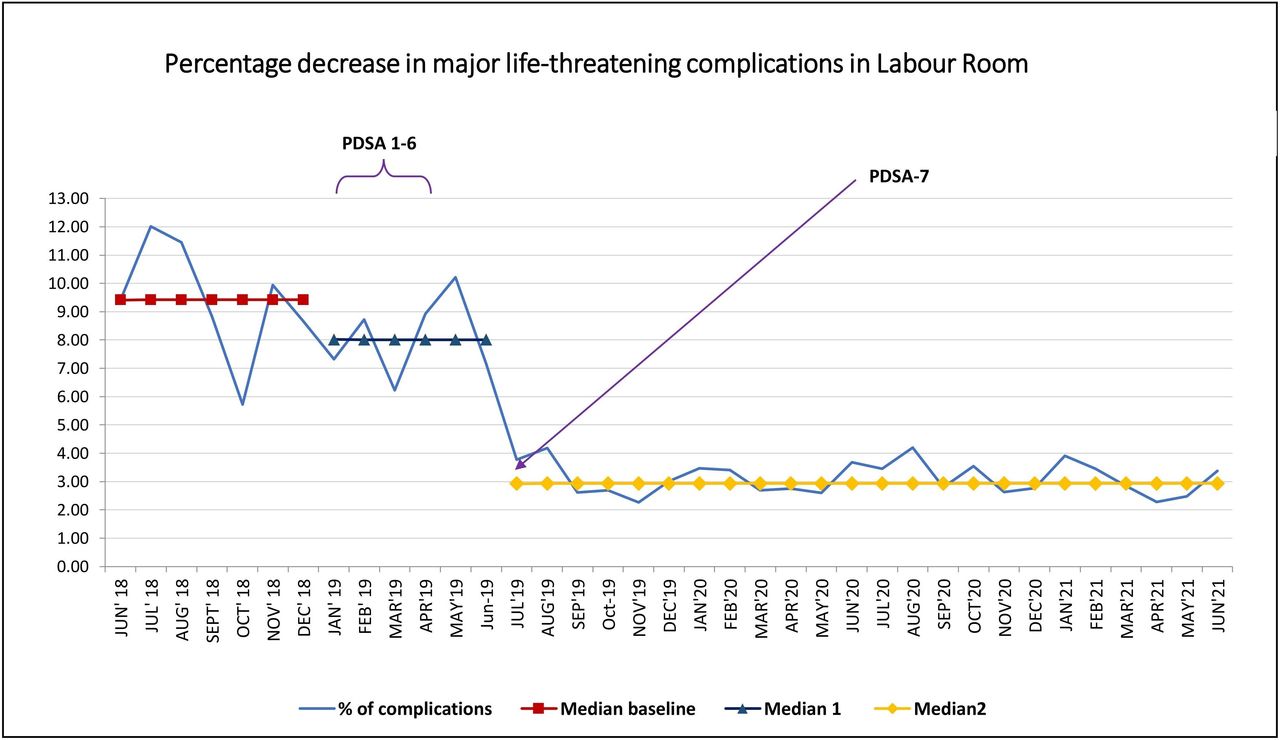
The team plotted the month-wise data of percentage of major life-threatening complications from June 2018 onwards on a run chart. The median complication rate before implementation of the QI project was 9.43%. After implementation, in the first 6 months, the median was 8.02%. June 2019 onwards the team observed a shift in the data and calculated the median again which was 2.93%. There was a 6.5%-point reduction (68.93%) in the median complication rate of major life-threatening complications following this improvement process. Run chart showing percentage decrease in major life-threatening complications in LR (figure 3).

Run chart showing % decrease in major life-threatening complications in LR. LR, labour room; PDSA, plan–do–study–act.
There were no significant changes in the percentage of maternal near-miss, maternal death and referral data. Run chart showing percentage of referral during the study period (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A run chart showing percentage referred out. PW, pregnant women.
Table 2 is showing percentage of these indicators along with the percentage of major complications.
Percentage of outcome indicators
From January 2019 to June 2021, 5822 HRP were identified in ANC OPD and LR. Out of a total of 5822 preidentified HRP, 3545 (60.89 %) were moderate and 2277 (39.11%) were severe HRP. A total of 3843 (66.01%) HRP were identified in OPD and 1979 (33.99%) in LR. Online supplemental table 3 includes a list of HRP identified in OPD and LR. Common HRP were previous CS without short birth interval (16.88%), hypothyroidism (9.72%), mild/moderate anaemia (8.69%), Rh-negative pregnancy without isoimmunisation (7.04%), severe anaemia (5.82%), breech/ malpresentation (5.65%), hypertensive disorder in pregnancy (4.59%), etc.
Supplemental material
Lessons and limitations
Pregnancy is a physiological process and one of the best experiences of a woman in her life. This is the expectation and right of a woman to have a positive childbirth experience. At the same time, all healthcare workers aim to provide quality healthcare services to a PW coming to the facility. For the same reason, the OBGYN team started this QI project in BM hospital.
Preidentification of HRP helped in the early initiation of investigations and specific treatment and prevented the worsening of certain modifiable HRP. HRP requiring super specialised treatment were referred to a tertiary care centre timely. Initially identifying all HRP in OPD took time as PW used to come for their ANC visits at different schedules and some of them were near expected date of delivery (EDD) and got admitted in LR without being preidentified in OPD. Gradually preidentified HRP started coming to LR for admission. The HRP number and red/yellow sticker on the ANC card helped the LR team especially JR and SN, to triage and highlight HRP during their treatment in LR. Colour coding of ANC cards also helped the support staff to identify HRP and to inform the duty doctors in case of a busy LR. Preidentified HRP were attended, admitted and managed on priority. This helped the facility to provide timely and better services to HRP and to prevent potential maternal complications. Complications were anticipated timely and managed well. Preparedness towards managing complications was better than before. The team observed a 6.5-point reduction in the rate of major life-threatening complications in LR following this QI initiative.
Further, this improvement process helped the team to assess the magnitude of HRP dealt with in the facility, to redistribute the available human resources according to priority area, and to involve staff at all levels. JR and SN were oriented and trained to triage HRP during admission and prioritise their management in LR. The NO and SGs were explained to identify HRP by looking at coloured stickers on ANC cards and to help them in getting HRP number and triaging. One additional SR posted in LR shared the responsibility of the LR team and allowed them to focus on providing care to PW admitted in LR. Additionally, the SN in LR were encouraged to conduct vaginal delivery for low-risk PW. The QI team also met the higher authorities of the hospital to make some policy changes to involve SNs in conducting vaginal deliveries.
The record of HRP identified helped the team to understand the type of HRP attending BM hospital and their risk stratification. The HRP list ensured the preidentification of all HRP and colour coding of ANC cards correctly. This list also helped the newly joined SR, JR and SN to identify the HRP and to carry on this QI initiative successfully. Any missing HRP and late-onset HRP were identified in subsequent antenatal visits in the OPD and LR.
Giving HRP numbers and colour coding of ANC cards helped in bringing awareness among support staff, patients and their relatives. They used to ask the reason for giving a number and putting a sticker on some of the PWs’ ANC cards. This allowed the team to involve them in patient care. PW and their relatives were aware of their HRP status and were well prepared. The team also encouraged them to share the information with other PW and family members to spread awareness about HRP and their role in managing such pregnancies.
Thus, a simple QI intervention allowed the team to improve patient care at different levels. The lessons learnt are generalisable and can be used in similar settings. Risk stratification using colour codes can also be implemented at the level of primary health centres for timely intervention and referral to higher centres.
However, despite being a simple methodology, there were challenges too in sustaining this QI project.
Because of the rapid turnover of SRs and JRs in the LR, reorientation of the new LR team and the newly posted SG and NO about this improvement process remained a challenge. The QI team involved their respective senior colleagues and directed them to orient all recruits about the working of this improvement process at the earliest. SR, JR and SN helped each other and the SG and NO to learn the process. The team leader and head of the department ensured that all recruits are aware of this new process and helped them to understand POCQI methodology and HRP whenever required.
Another challenge was to conduct periodic QI meetings. To overcome this challenge, in the first 6 months the team met weekly on a relatively free day in the afternoon and conducted the meetings even in the presence of one consultant, one SR and one SN. The weekly data and the discussions in the meeting were updated on the WhatsApp group for the benefit of the other members who could not attend the meeting. Later these meetings were arranged along with the routine monthly census reporting meeting of the department. The QI team met separately as and when required.
The success was also dependent on good communication and coordination between duty doctors and SNs posted in LR. Although the stickers are very cost-effective, regular procurement of yellow and red stickers is another limiting factor of this QI initiative.
The major limitation of this QI initiative is the team did not analyse the effect of the implementation of this intervention process on neonatal morbidity and mortality. The team plans to carry forward this process with the inclusion of neonatal health indicators as outcome measures.
Conclusions
In public sector hospitals, it is a major challenge to provide quality health services to PW with limited human resources. QI methodology has provided an opportunity to improve health services with available resources. In this QI initiative, with a simple intervention the team improved patient care at different levels. They adopted similar processes to improve other areas of patient care in the same as well as other departments of the facility. Other facilities with similar settings can also adopt this methodology to improve their healthcare services without any additional human resources or financial support.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge the contribution of the Nationwide Quality of Care Network (NQOCN), India for providing us training on POCQI methodology. We also acknowledge the mentoring support from NQOCN, India for conducting and sustaining this QI project, drafting the manuscript and for reviewing the manuscript before submission.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrPrabhaRanjan1, @DrMahtabSingh1
Contributors PK, MS and SS conceptualised the project and provided leadership to carry out this quality improvement work. PK, SS, PA, SR, AA, KA and SG were responsible for the conduction of the improvement process and data collection. PK, AA, KA and SG were responsible for data collection and compilation. PK, MS and RR contributed in drafting of the manuscript. PK and SS accept full responsibility for the work and/or the conduct of the study, access to the data, and the decision to publish. All authors revised it critically and approved the submission. MS and PK contributed in the data analysis and revision of the manuscript. All authors approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. Publication of this article is made Open Access with funding from the Nationwide Quality of Care Network.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.