Article Text

Abstract
Objective In response to the unacceptable racial disparities in US obstetric outcomes, our health system established a formal goal to reduce maternal morbidity for black women. Here, we describe our process for meeting this equity-focused goal in the context of diverse implementation climates at 5 inpatient sites.
Study design To meet the system goal, we established a collaborative of multidisciplinary, site-based teams. The validated 18-question Implementation Climate Scale (ICS) was distributed to site clinicians at baseline. Sites focused on haemorrhage, performing case reviews of black women meeting morbidity criteria. Comparing cases by site, site-specific areas for improvement in haemorrhage risk assessment, prevention and management emerged. Evidence-based practices (EBPs) were then selected, tailored and implemented by site. Monthly system-wide team meetings included (1) metric tracking and (2) site presentations with discussions around barriers/facilitators to EBP implementation. Maternal morbidity rates among black women were compared the year before goal development (1 July 2019–30 June 2020) to the year after (1 July 2020–30 June 2021).
Results Mean ICS scores for inpatient obstetric units differed by site (p=0.005), with climates more supportive of implementation at urban/academic hospitals. In response to case reviews, sites reported implementing 2 to 8 EBPs to meet the goal. Despite different ICS scores, this process was associated with significant reductions in maternal morbidity for black women from pregoal to postgoal development overall and at sites 1, 2 and 3, with non-statistically significant reductions at sites 4 and 5 (overall: −29.4% reduction, p<0.001).
Conclusions A health system goal of reducing maternal morbidity for black women led to a data-driven, collaborative model for implementing site-tailored interventions. If health systems prioritise equity-focused goals, sites can be supported in implementing EBPs that improve care.
- collaborative, breakthrough groups
- implementation science
- obstetrics and gynecology
Data availability statement
Data are available on reasonable request. Data will be made available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There are unacceptable racial disparities in US obstetric outcomes.
WHAT THIS STUDY ADDS
This study describes a collaborative approach to a multifaceted, equity-focused goal across a US health system, which resulted in significant reductions in maternal morbidity for black women.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Prioritisation of equity-focused goals at the health system level has the potential to support diverse sites in reducing disparities in obstetric outcomes.
Problem
Significant racial and ethnic disparities in maternal morbidity and mortality are only widening in the USA. Pregnant or postpartum women of colour are 3–4 times more likely to die than their white counterparts, regardless of socioeconomic status.1 Black women are also at significantly higher risk of severe maternal morbidity.2 It is clear that urgent change is needed to curb the crisis in racial and ethnic disparities in obstetric outcomes.
While obstetric racial and ethnic disparities are complex and multifactorial, one critical area of focus is care quality.3 Studies have documented that black patients tend to receive care in different and lower quality hospitals than white patients.4–6 In addition, hospitals that had higher proportions of black deliveries also had higher severe maternal morbidity rates for women of all races.4
Yet, much of the work around disparities in maternity care has focused on describing their complexities, rather than studying levers for combatting care inequities.7 One powerful method to improve care quality of individual sites is through quality collaboratives and health system-wide partnerships, which can pool resources and stimulate structured change.8–10 This teamwork approach to quality improvement has the potential for success at sites that might otherwise not have a robust quality infrastructure or a healthy climate around implementing new practices. Work in obstetrics has only just begun to address whether such collaborative models have the potential to reduce disparities in outcomes.11 Care collaboratives have the potential to improve care quality in sites that need improvement most, those often serving the largest populations of colour.
Background
In response to the unacceptable racial disparities in US obstetric outcomes, our health system took initiative, establishing a bold, formal goal to significantly reduce maternal morbidity for black women over a 1-year period.12 Here, we describe our process for meeting this equity-focused goal at five diverse, inpatient obstetric sites, which included (1) development of multidisciplinary teams, (2) collection of quality data to determine site-specific areas for improvement and (3) monthly system-wide meetings that supported implementation. This work compares maternal outcomes in our health system 1 year before to 1 year after establishment of this goal. We hypothesised that a collaborative approach would allow individual sites to select and implement the evidence-based practices (EBPs) they needed most in order to reduce maternal morbidity for black women.
Methods
This is a prospective, quality improvement study comparing outcomes 1 year before (1 July 2019–30 June 2020) and 1 year after (1 July 2020–30 June 2021) development of a health system-wide ‘team goal’ to reduce maternal morbidity for black women. SQUIRE V.2.0 guidelines were used when drafting this manuscript.13
Our health system is composed of five sites that provide inpatient obstetric services. Sites 1 and 2 are urban, academic hospitals, site 3 is a rural, community hospital and sites 4 and 5 are suburban, community hospitals. Breakdown of sites by delivery volume and proportion of black patients are detailed in table 1.
Characteristics of five labour and delivery sites within the health system, with approximate delivery volumes and proportion of black patients delivering at each site
Multidisciplinary teams
To meet the system goal, first, leadership of the project was established as the Chair of the Department of Obstetrics & Gynaecology and the Physician Lead for the system-wide Women’s Health Service Line. Next, we established a collaborative of multidisciplinary teams at each of the five sites. While teams could recruit as many members to participate as desired, and included patient representatives, we asked that teams be led by a triad including a physician, nursing and quality leader who would represent the local teams at system-wide meetings.
Baseline measurement
Implementation Climate Scale
At the start of this work, the Implementation Climate Scale (ICS) was distributed to clinicians caring for patients in maternity care settings at the five inpatient obstetric sites from all roles, including physicians, nurses and nurse-midwives. Implementation climate is the extent to which intended users perceive that use of EBPs are expected, supported and rewarded.14 Leading theories posit that the stronger the implementation climate, the more consistently EBPs will be used in care at a given site.15 The purpose of the ICS in this setting was to obtain a baseline sense of how easy or difficult the implementation of EBPs would be at each site, and then to place clinical and implementation outcomes in context of these results.
The survey was an adapted form of the 18-question ICS,16 which has been validated in several settings, including child welfare services, substance use disorders treatments and inpatient nursing units.17–19 The ICS measures six dimensions for EBP implementation (each subscale made up of three items): focus on EBP, educational support for EBP, recognition for EBP, rewards for EBP, selection for EBP and selection for openness. Response format is a 4-point Likert scale with higher scores indicating greater value.
Clinicians were invited to participate anonymously via email ListServe. There were no exclusion criteria. The survey was open from 13 November 2020 to 13 December 2020. ICS total and individual dimension scores were compared by site using one-way analysis of variance (ANOVA).
Case report forms
Using initial assessments around severe maternal morbidity in black women at our institution, it was determined that the majority of cases (approximately 50%) met criteria due to obstetric haemorrhage. Thus, the decision was made by the leadership team to focus the first year of the team goal on evaluation and improvement of care and disparities in obstetric haemorrhage. A standardised case report form (CRF) was developed in Research Electronic Data Capture (REDCap), adapted from the American College of Obstetricians and Gynecologists CRF for severe maternal morbidity.20 Additional questions focusing on the risk factors for, causes of and treatments for obstetric haemorrhage were added to the form. The CRFs were distributed to site-based teams, and feedback used to modify the CRF to best meet site needs.
Each week, data experts pulled cases of black women meeting criteria for obstetric haemorrhage (defined as estimated and/or quantitative blood loss >1000 cc for any mode of delivery21 or retained placenta) at each site and distributed the list to each site’s leadership. Leadership distributed cases to team members for data abstraction into REDCap CRFs. Clinical and demographic characteristics, labour and delivery outcomes including details of obstetric haemorrhage as well as management modalities were compared by site using χ2 or Fisher’s exact test for categorical variables and one-way ANOVA and Kruskal-Wallis for continuous variables as appropriate.
Monthly system-wide team meetings
Site-based leadership were asked to attend monthly system-wide meetings. At these meetings, REDCap data from CRFs were presented and compared by site. In addition, maternal morbidity rates by site were tracked monthly and presented for discussion. As such, site-specific areas for improvement in haemorrhage risk assessment, prevention and management emerged. As a part of these meetings, sites then discussed and selected EBPs to be implemented in response to the data. While many EBPs were selected from the Council for Patient Safety in Women’s Health Consensus Bundle on Obstetric Haemorrhage,22 sites were able to choose any EBPs they felt would be effective at meeting the ‘team goal’. Sites then tailored and implemented selected EBPs with the goal of improving haemorrhage-related morbidity for black women.
Additionally, as EBP implementation expanded across sites, monthly meetings also included presentations from sites on progress, with engaged group discussions around barriers and facilitators to EBP implementation. As part of these meetings, sites that had successfully implemented strategies shared their success and challenges in order to help facilitate implementation at other sites. This allowed for all sites to contribute as a presenter and to participate as a learner in the adoption of new strategies. Because each site was implementing several interventions simultaneously, and sites were implementing different EBPs, individual Plan-Do-Study-Act (PDSA) cycles for each EBP are not described here. However, sites often used PDSA cycle terminology when describing their individual implementation processes in monthly group meetings.
Outcome measures
Implementation outcomes
At the completion of the first year of the team goal, June 2021, a year end survey was distributed to sites to compile implementation results. Sites were asked to list (1) areas for improvement identified through data analysis and (2) EBPs implemented. For each EBP implemented, sites were asked to describe local barriers to implementation, and how (if at all) the team goal structure aided in implementation. Surveys were completed together by at least two members of the site-based leadership team, including one physician and one nursing representative. Cross-validation of site responses were performed with a second survey compiling initial survey responses.
Clinical outcomes
Our primary outcome was maternal morbidity among black women. For the purposes of this work, maternal morbidity was defined as present if a case met any of the following criteria: Vizient 4, Vizient 5, Vizient 6 (including postpartum haemorrhage (EBL/quantitative blood loss ≥1000 cc) and/or retained placenta, postpartum infection and obstetrical embolism), or the Centers for Disease Control and Prevention severe maternal morbidity metric.23
Maternal morbidity was compared from before to after initiation of the team goal by site using χ2 test. Maternal morbidity is shown as graphed rate by month (with blinded absolute rates) and the change in proportion from before to after implementation (Δ) rather than specific individual site rates to protect site anonymity. Statistical analyses were performed with Stata V.15 (StataCorp, College Station, Texas, USA). All tests were two-tailed, and p values <0.05 were considered statistically significant.
Results
Implementation Climate Scale
The ICS was completed by 156 clinicians across the 5 sites, of which 136 (87.2%) completed it regarding an inpatient obstetric site and were included in this analysis. More than 80% of participants were from the two urban, academic sites, and 18% from community sites. There were no responses from site 5. Of participants, 31% were nurses, 6% nurse-midwives and 63% physicians. Participants were median age 37 years IQR (32–45) and nearly 50% had >10 years of experience in their role.
Of those who responded, total ICS scores differed by site, and were higher among the two urban, academic sites as compared with community sites (p=0.005; table 2). Similar significant patterns emerged in the subscales of focus on EBPs (p=0.01), education support for EBPs (<0.001) and recognition for EBPs (p<0.001). There were no significant differences among sites in the subscales of rewards for EBPs, selection for EBPs and selection for openness.
Implementation Climate Scale (ICS) results by site, both overall and for each subscale
Case review forms
One hundred seventy-two cases of black women meeting criteria for obstetric haemorrhage were reviewed across sites from July 2020 to June 2021 (table 3). Patients meeting haemorrhage-related morbidity were overall similar between sites at baseline, such as in age and body mass index (BMI). Importantly, across sites, high rates of anaemia during pregnancy were noted among cases. Yet, intravenous iron, an EBP for anaemia management, was used at sites 1 and 2, and not at all at sites 3, 4 and 5. Sites 1, 3 and 5 saw the majority of their haemorrhage cases occurring during labour inductions, and all sites noted most cases occurred after vaginal delivery.
Cases of black women meeting obstetric haemorrhage criteria by site from July 2020 to June 2021
Sites differed most in terms of management modalities selected for treatment of obstetric haemorrhage. For example, tranexamic acid, a highly effective agent for reducing bleeding during postpartum haemorrhage, was used almost exclusively at site 2. All sites reported low utilisation of B-lynch sutures and uterine artery embolisation, effective second-line treatments for haemorrhage when uterotonics are unsuccessful.
Implementation outcomes
All five sites submitted end-of-year reports. In response to case reviews, sites reported implementing two to eight EBPs to meet the team goal (table 4). Some of the most commonly implemented EBPs included improvement in documentation and coding practice, incorporation of a haemorrhage risk assessment tool into the electronic medical record (EMR) and implicit bias training.
Evidence-based practice (EBP) implementation by site
When considering barriers to implementation, common themes included generating provider buy-in, and getting accurate data streams to support implementation. When asked how the collaborative helped sites in support of implementation, the most frequently mentioned facilitator of the collaborative was the opportunity to share best practices and receive feedback. Sites also mentioned an encouragement to expand focus and an appreciation for progress deadlines.
Clinical outcomes
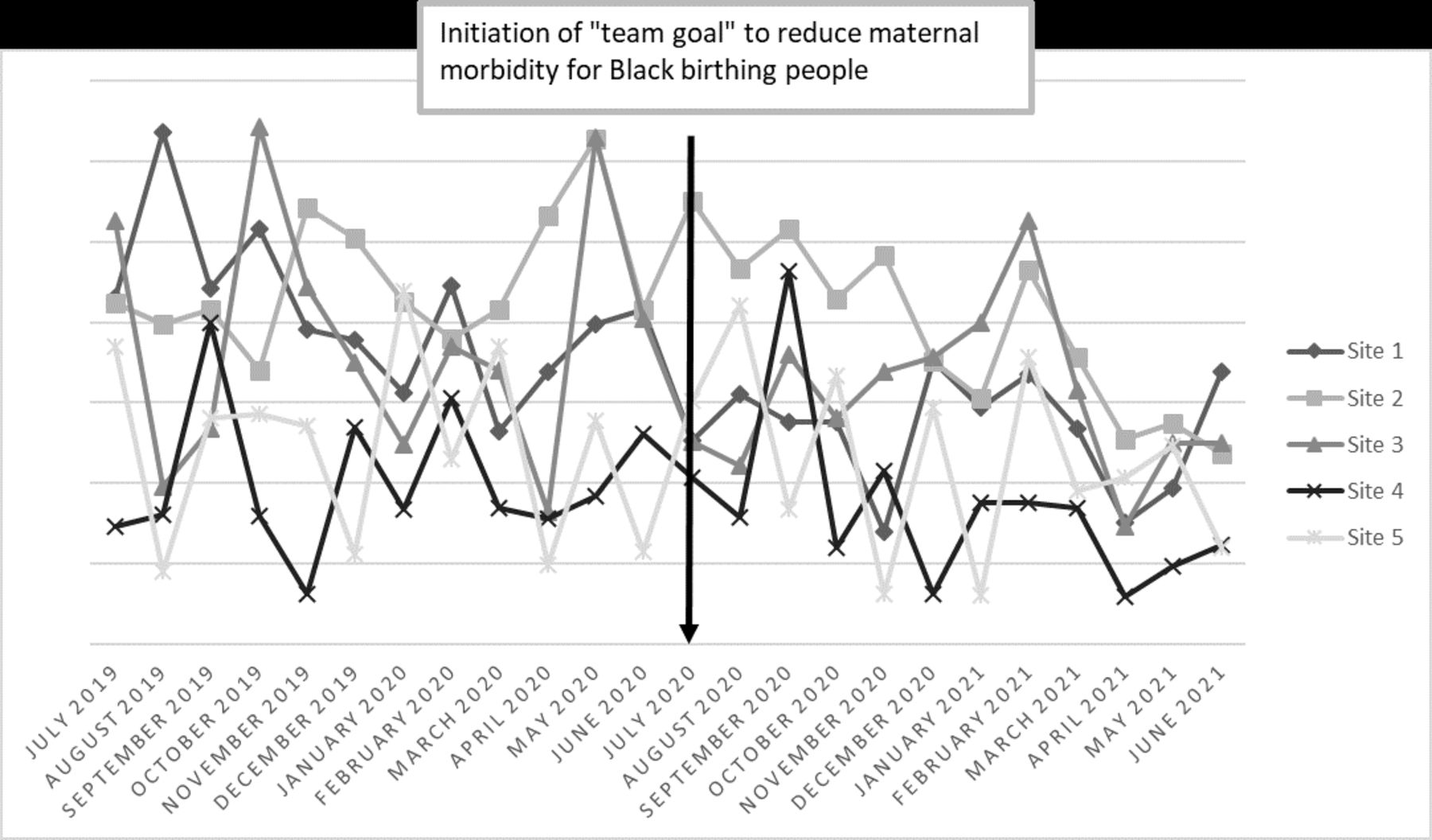
This process was associated with significant reductions in maternal morbidity for black women from pregoal to postgoal development overall. Scores at sites 1, 2 and 3 all had significant improvements in maternal morbidity with non-statistically but likely clinically significant reductions at sites 4 and 5 (overall: −29.4% reduction, p<0.001; table 5). Maternal morbidity rates over the pre-implementation and post-implementation periods are demonstrated by site over time in figure 1.

{kind=link}
Maternal morbidity rate by site over the pre-implementation and post-implementation periods. The ‘team goal’ began in July 2020, and meetings occurred monthly throughout the year. Absolute rates are blinded per site request.
Change in maternal morbidity from pre-implementation to post-implementation of the health system-wide team goal, by site
Connecting the dots
While this work describes an overarching view of this system-wide quality improvement level, it may be prudent to connect the dots, that is, to detail how the described process led to tangible site-specific change. During the monthly meeting, sites 1, 2 and 5 all noted that a large percentage of their haemorrhages were occurring after labour induction. In response, they developed a standardised protocol for active management of labour induction, which was workshopped at the system level, in order to prevent prolonged inductions that increase haemorrhage risk. Site 3 was struck by the lack of utilisation of intravenous iron in response to antepartum anaemia, and developed a protocol modelled after protocols already in place at sites 1 and 2 to expand their use of this effective medication. For a final example, sites 4 and 5 noted their differences in medication selection for management of obstetric haemorrhage as compared with sites 1 and 2, thereby developing standardised protocols with system-wide input for haemorrhage management.
Lessons and limitations
In this work, we evaluated the impact of a health system-wide ‘team goal’ to reduce maternal morbidity for black women across five inpatient obstetric sites using site-based multidisciplinary leadership. We demonstrated that these sites differed in practice model, and in climate around implementation. Standardised CRFs were used to evaluate cases of haemorrhage-related morbidity for black women at each site, and then compared at monthly system-wide meetings. Using the results of these case reviews, including significant differences in haemorrhage management noted by site, sites individually selected and implemented between two and eight EBPs each. And, despite differences in implementation climate across sites, this process was associated with significant reductions in maternal morbidity for black women from pregoal to postgoal development overall and sites 1, 2 and 3, with non-statistically but likely clinically significant reductions at sites 4 and 5 (overall: −29.4% reduction, p<0.001).
Our work describes in detail a successful system-wide quality improvement initiative with an equity focused goal. Our results align with other recent studies in this field. For example, Main et al performed a cross-sectional study of 99 hospitals participating in a haemorrhage quality improvement collaborative in California, which demonstrated significant reduction in disparities in severe maternal morbidity.11 Davidson et al demonstrated that implementation of a haemorrhage bundle while holding an equity lens to case reviews was associated with reduced rates of haemorrhage-related morbidity in Texas.24 While our work focuses on one health system rather than a state, we were able to demonstrate how targeting site-specific differences in case reviews allowed for implementation of needed EBPs, which was associated with clinical improvement. Future work should evaluate if such targeted quality efforts could be made at a state collaborative level. In addition, it is critical that future work go beyond hemorrhage-related morbidity. Since the publication of the Council for Patient Safety in Women’s Health Consensus Bundle on Obstetric Haemorrhage,22 our field has produced numerous other bundles of utmost importance to maternity care quality.25–27 Ongoing work through our health system will focus on and evaluate EBPs related specifically to the reduction in racial and ethnic disparities bundle for the second year of this ‘team goal’.27
Strengths and limitations
The strengths of this work lie in its large, prospective nature. In addition, this study is unique in its application of implementation science to an equity focused quality improvement initiative. Our work evaluated implementation climate, a key determinant of effective implementation of EBPs in healthcare, and took the success of our collaborative in context of these results.14 Thus, we were able to demonstrate clinical impact at all sites, including those with less positive climates around implementation.
Our evaluation of implementation climate was limited in its low response rate from non-academic sites. This study is also limited in its lack of patient-level data, and that the metrics tracked, including clinical outcomes or process measures, were overall limited. Maternal morbidity is shown only as a graphed rate by month and a change from pre-‘team goal’ to post-‘team goal’ development as preferred by our involved sites. Sites did not feel comfortable with providing absolute rates by month or for the pre-implementation and post-implementation periods. Given the design, we can only state associations between the ‘team goal’ and our improved outcomes. It is plausible that other system changes and/or secular trends, such as the COVID-19 pandemic, could have contributed to these improvements. Furthermore, our work did not include an evaluation for the impact of the our ‘team goal’ on non-black patients. As our system moves forward in this work, we plan to address goals in subsequent years to include all black, Indigenous and people of colour in order to address the profound disparities in these population groups. With collection of additional data in the coming years, we will also be able to assess sustainability.
Conclusion
A health system goal of reducing maternal morbidity for black women led to a data-driven, collaborative model for implementing site-tailored interventions. If health systems prioritise equity-focused goals, sites with an array of implementation climates can be supported in implementing EBPs that improve care.
Data availability statement
Data are available on reasonable request. Data will be made available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The institutional review board of the University of Pennsylvania exempted this study as quality improvement.
References
Footnotes
Twitter @rebeccahammmd
Contributors RFH designed the evaluation of the intervention, created the data collection tool, drafted the data analysis plan, analysed the data and drafted and revised the manuscript. SS and EH led the intervention overall, contributed to the data analysis plan and revised the manuscript. AJ, RF, TB and JC led the intervention at local sites, provided data and revised the manuscript. RFH acts as the author responsible for the overall content as the guarantor.
Funding This work was supported by a K23 Mentored Career Development Grant from the NICHD (K23 HD102523).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.