Article Text

Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is no agreed standardised optimal protocol for performing intracytoplasmic sperm injection (ICSI). However, benchmark levels for ICSI key performance indicators (KPIs) have been suggested from the Alpha-ESHRE consensus meeting 2017. Clinics must monitor their KPIs and act accordingly if any reduced performance is detected.
WHAT THIS STUDY ADDS
An example of the use of quality improvement methodologies within fertility to standards for quality improvement reporting excellence(SQUIRE) guidelines.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Larger clinics may benefit more from the methodologies used in this study. This study is one of few reports where embryology KPIs are tracked following defined and controlled laboratory and clinical changes.
Problem
An established fertility clinic with over 16 years of delivering successful intracytoplasmic sperm injection (ICSI) treatment to infertile couples observed a drop in its fresh ICSI implantation rate key performance indicator (KPI) below benchmark level. This small-sized fertility clinic in southern England performs approximately 300 fresh egg collections a year, approximately half of which are ICSI treatments. The clinics expects to achieve a benchmark with combined maternal ages (<40 years) and day of embryo transfer of at least >25% implantation rate for fresh ICSI cycles. During 2019, the clinic identified a dip in its fresh ICSI success rates; however, the low number of fresh treatment cycles at this clinic and the natural variation (common cause variation) expected within fertility treatment can lead to unstable indicators which should be investigated with caution. Results will be influenced by patient factors (eg, maternal age, previous repeated unsuccessful attempts, significant clinical adverse factors) and the policies for deciding the day of embryo transfer and number of embryos to replace. The clinic had recently implemented a number of changes to procedures, increasing the number of blastocyst transfers and vitrification of embryos. Other ICSI KPIs at the clinic continued to reach benchmark levels, for example, fertilisation rate and damage rate. There is an inherent delay for clinical performance indicators related to pregnancy success, because of the wait for pregnancy blood result and 7–9 weeks before ultrasound data are available.1 Therefore, although implantation rate is a sensitive indicator of laboratory performance, it has a limited ability to rapidly detect suboptimal laboratory performance shifts. This has more impact on smaller clinics performing fewer cycles as larger multicentred clinics with much higher caseloads would have more stable indicators to enable identification of any issues more quickly. Once a trend had been identified the clinic further monitored the fresh ICSI implantation rate and undertook a root cause analysis of any recent changes around the affected period that could be having an impact. Implantation rate is judged an important indicator that reflects the overall performance of the laboratory, and an overall low implantation rate is a serious sign of a systemic problem.2 The clinic continued to see this indicator not reaching expected values and a plan for improvement was made and implemented to achieve benchmark fresh ICSI implantation rates as soon as possible.
Setting
The clinic collected eggs 2 days a week. Changing one of its egg collection days from Tuesday to Friday in order to offer extended culture to all patients from September 2018. There can be up to six egg collections per Wednesday list and up to three per Friday list. All patients have the same time for trigger injection, regardless of whether they are first or last on the list. This is based on the premise that 36–37 hours post-trigger is acceptable, and that eggs are collected from patients near to 40 hours post-trigger without compromising egg viability. Egg collections take place in Trust theatres. There are two ICSI practitioners, who use different micromanipulation needle types and two different ICSI rigs.
Background
ICSI is a technique used to overcome male factor infertility and fertilisation failure.3 A single sperm is selected, immobilised and injected into each denuded mature egg that has been stripped of its cumulus cells using micromanipulation tools. The first measurable and important parameter of successful ICSI is normal fertilisation and egg damage rates. While success of ICSI is often measured in terms of clinical pregnancy or live birth, high rates for laboratory parameters such as fertilisation or embryo development significantly contribute to the overall efficacy of a treatment cycle. The Alpha-ESHRE consensus meeting suggested KPIs with competence and benchmark levels for different parameters, but each clinic should establish their own benchmarks based on their experience and clinical practice.2 Implantation rate, defined at the number of fetal hearts observed per number of embryos transferred, provides an indication of the overall performance of the laboratory.
ICSI is a multifaceted, highly technical, invasive procedure that involves manipulation of gametes and is time intensive for the laboratory. Success of ICSI can be influenced by many factors during several consecutive steps, when evaluating one you cannot exclude the end effect of the previous.4 Patient factors, gamete quality/competence, clinical stimulation protocols, upstream and downstream procedures, timings, practitioner variation, environment, culture conditions and the ICSI technique itself are just a few examples. Published studies have led to various options for performing ICSI and despite 30 years of use, there is no agreed standardised optimal protocol, resulting in many clinics around the world using slightly different approaches.4
Design
To ensure that a problem is correctly understood and framed prior to starting the PDSA cycle an imperative part of the wider methodological approach is to conduct investigations.5 Investigations can include process mapping, failure mode effects analysis, cause and effect analysis, data analysis and review of existing evidence.
A lead from each discipline of the multidisciplinary team formed a working party to look at all current processes, any recent changes and discordance between the clinics practice and the current published evidence base to identify causal factors for this drop in fresh ICSI success rates. The working party were motivated and driven to find any improvements to implement as soon as possible in their duty to provide the best care to patients. An action plan was put in place with regular meetings held to share findings from investigations and to regularly review the KPIs. The Trust was informed. If no improvement was seen the team agreed to seek advice from an external review, to scrutinise all procedures and processes, to help identify any areas where improvements could be made. This process mirrors the Lean management philosophy of ‘fresh eye approach’ and ‘Gemba’. Fresh eyes method is the introduction of people to an area or process in which they are not familiar. By doing this, the people are not biased towards one method or another and may quickly see some improvement opportunities that people working in the area have overlooked. As results did not improve, an external review was invited in December 2019.
All clinic fresh and frozen treatment cycle information is collected within an electronic database and a number of standard KPIs are analysed and reported at quarterly KPI meetings. Background measures such as environmental monitoring, consumable tracking, equipment monitoring, and non-conformances/adverse outcomes are monitored and records kept. All this information was used by the team (both clinical and laboratory) to perform a root cause analysis to identity a possible cause for the reduction in fresh ICSI success rates as shown in online supplemental information 1.
Supplemental material
The team’s extensive analysis of the clinics data and existing evidence revealed causal factors that might be impacting ICSI success rates. An increased frequency of egg collections being performed <36 hours post-HCG trigger was noticed, and ICSI cases were always first on the lists because of the additional processing that was required. The root cause of this was a Trust wide theatre operational improvement initiative to reduce operating theatre running cost by optimising start times of list (defined as first contact; needle to skin). Resulting in egg collections starting earlier in the morning than previously. These cases had a lower success rate than cases performed at 36 hours for in vitro fertilisation (IVF) and 37 hours for ICSI. The clinic would implement staggered personalised HCG trigger times for patients based on the theatre list order and type of treatment to ensure 36 hours for IVF egg collections and 37 hours for ICSI, based on clinic data. This identified a need for impact assessment when there is a change to any aspect of operation that could impact the fertility clinic. Adding more flexibility to the day of egg collection (eg, 3 lists) might further optimise the time of egg collection to improve viability and could also ease the pressure on the embryology team by allowing for a more even distributed workload. However, as the clinic relies on the Trust theatres for egg collection procedures, this would be controlled by hospital management.
The airflow and temperature in theatre has historically been cool and inconsistent, temperature control is critical for maintaining egg viability. The theatres are open plan with many types of operations taking place, including dentistry, so there could be volatile organic compounds in the background air that might adversely be impacting on egg quality. The team put in a capital bid in 2019 to purchase an enclosed portable biological safety cabinet (Unica) to gain more control of the environment during egg collection procedures and replace the aged embryology equipment. Bids were also put in for electronically controlled heated stages to replace aged equipment within the IVF laboratory for more consistent temperature control. While the team waiting for procurement of new equipment temperature optimisations were made to existing equipment for egg collection, such as use of a second grant heated block for egg tubes.
The clinical team engaged with the improvement work and proposed the high estradiol levels associated with the superovulation protocols may be causing suboptimal progesterone levels in fresh cycles. This may help explain why the fresh ICSI implantation rate was lower than frozen cycles. The clinic’s frozen ICSI implantation rates were above benchmark which suggested that ICSI embryo viability may not be compromised, based on the assumption that the optimal embryo is transferred in the fresh embryo transfer and suboptimal embryos are transferred in the frozen embryo transfer. Corrective action was proposed to double the dose of progesterone support from January 2020 for all patients having stimulated IVF/ICSI.
The clinic had always placed cumulase enzyme and polyvinylpyrrolidone (PVP) (buffered for ambient air) within a CO2 incubator prior to use because the culture media needed to be gassed. The team knew that this may alter the pH of the enzyme or PVP; however, the culture period is short (~2 hours), and this process had been used for >16 years with good success. With an appropriate heated workstation, the use of zwitterion-buffered media for pH maintenance during very brief visual assessments (<2 min) is not considered justified, although when denuding eggs and assessing their maturity prior to ICSI such media can be used to provide a more stable environment.6 With reassurance from the external reviewer the clinic would now switch culture media for an ambient air buffered handling media for the egg collections and denudation wash droplets to prevent any risk of pH change. The denuding dishes are warmed in an ambient air incubator. A bench top incubator would be switched to temperature only (no CO2) for this purpose on an egg collection day. Due to historic toxicity concerns of some zwitterion buffers during ICSI injection the clinic took a cautious approach to changing to a new injection media.7 A process of validation began in the first quarter of 2020 of split sibling eggs between current culture media and the new handling media. This was cut short by the clinic closure in March 2020. After reviewing the data in 2021 from this small cohort of eggs and outcomes the clinic could establish that the new media was not inferior to the current culture media used (clinical pregnancy/ET; 20% (1/5) current IrvineScientific continuous single culture medium complete (CSCM-C), 29% (2/7) new IrvineScientific multipurpose handling medium complete (MHM-C).
The optimal timings for ICSI remain unclear and existing results are not fully conclusive. Most articles are concordant that a preincubation time before ICSI is beneficial on ICSI results, and cumulus–corona cells may have a positive effect during this preincubation.8 Improvements in egg maturation, fertilisation rate and embryo quality have been reported following incubation periods of 2–4 hours between egg collection and ICSI.9–11 A longer culture period prior to cumulus cell removal has been associated with an increase in clinical pregnancy and live birth results;12 however, other studies have shown that there is no influence on ICSI outcome.13 14 The current clinic process there is usually a 3-hour delay between denuding eggs and performing ICSI, for example, denudation takes place after 11:00 hours and ICSI begins at 14:00 hours. This delay might adversely affect egg quality and competence as eggs may be more vulnerable to temperature and environmental changes without protective cumulus.12 The overall suggestion from the majority of studies is for the injection to be performed straight after the denudation procedure.4 The lab team proposed to change the process to incubate eggs for ~3 hours after collection, denudation would then take place at 40 hours post-HCG trigger and ICSI injection to commence straight after this. Clinic data also supported this with optimal success rates in groups that had ICSI injection at 40–41 hours post-HCG trigger. PVP would be added to the ICSI dishes 10 min before use.
The ICSI procedure itself was assessed during the external review, and both ICSI practitioners were observed to perform mock ICSI injections and were highly skilled at this task, so it was not a cause for concern. The only suggested improvements were to save time during the procedure, which might reduce the amount of time culture dishes are outside the incubator which would reduce the risk of changes in temperature or pH. Rotation of the egg on the holding pipette with the injection pipette for perfect alignment of the first polar body at 12:00 or 18:00 hours takes additional time. The optimal positioning of the first polar body, thought to be associated with the presumed location of the meiotic spindle, has not been determined.4 Immunostaining and polscopy techniques have demonstrated that the two do not always coincide;15 therefore, the location of the polar body is only a crude measure for spindle position.16 If the 15:00 and 21:00 hours are avoided, egg position should be quickly enforced using the holding pipette only and the ICSI swiftly performed.
One of the problems with troubleshooting at the clinic was that there are two different types of ICSI workstation: Narashige with oil syringes and Research Instruments (RI) with air syringes. Both ICSI practitioners also have different ways of pre-equilibrating the injection pipettes and use different micromanipulation products. For consistency and during trouble shooting and improvement work, all practitioners would use the same tools and pre-equilibration technique.
The team also decide to tighten up on timings for fertilisation checks, with ICSI the optimal time to observe the maximum number of normally fertilised eggs is 16 hours postinjection (HPI).17 Clinic data indicated that checks were not strictly performed at 16 hours but between 16 and 18. Strict fertilisation check times were to be followed going forward with ICSI cases being checked at 16 HPI and IVF within 16–18 HPI.
The entire team showed a strong commitment to these changes which involved a great deal of process alterations. The changes would be made and sustained with close monitoring of KPIs.
Baseline measurement
Analysis: An external review was invited by the clinic to scrutinise all procedures and processes to help identify and confirm areas where improvements could be made. Recommendations were made covering clinical/laboratory policy and procedures, equipment and facilities, much of which had already been identified by the clinic staff analysis but confirmed and supported by the external reviewer. A plan was made to implement as many recommendations as was feasibly possible within the NHS service and the team designed a plan for improvement.
The strategy for implementation was based closely on the driver diagram (see online supplemental information 2). The main outcome measure for the improvement work was the fresh ICSI implantation rate which is defined as the number of fetal hearts divided by the total number of embryos transferred per ~25 ICSI case. Process measures included ICSI damage rates and fertilisation rates as well as background measures including egg maturity, maternal age and egg number. Process and background measures and their definitions are shown in table 1. Running the data on statistical-process-control (SPC) charts over time might reveal patterns in the data that indicate improvement due to the changes made. BaseLine, a system behaviour chart software, was used to plot the time-sequenced data. SPC was used prognostically to establish whether changes made to the process of ICSI led to improvement in KPIs. IBM SPSS Statistics 27 was used to perform the statistical analysis. To examine any difference in ICSI implantation rate between time periods preimplementation and postimplementation of improvement interventions χ2 was used.
Supplemental material
List of QI project KPI measures, their definitions and benchmarks
KPI measures were plotted either as a weekly average and/or a consecutive 25 ICSI case average. Averages can hide information and patterns so plotting data weekly would reveal more information but might not be helpful for pregnancy outcome data due to vast variation.
Implementation of improvement strategies
Our aim was to improve the fresh ICSI implantation rates to benchmark as soon as possible. The changes determined by the team for improvement following a root cause analysis, troubleshooting, data analysis and recommendations from an external review are listed in table 2. Patients and the public were not involved. The troubleshooting and investigation occurred over a series of months after the problem was identified. After no improvement was seen following changes made by the clinic and with support from an external review, a bundle of improvement interventions was to be put in motion as soon as possible at the end of December 2019. Any change that could be implemented with immediate effect was, for example, double dose of progesterone, personalised HCG time. Other changes involved the purchase of new equipment or media that took time to procure and then validate safely prior to first use. This led to a three-phase approach to the intervention PDSA bundle as shown in the study flow table below, which displays the changes that occurred over time.
Study flow table
The improvement work was interrupted by the COVID-19 pandemic when the fertility sector was legally required to stop all treatment in March 2020. During the shutdown period, the clinic was required to apply for a license to recommence treatment with safeguards in place to protect staff and patients from the virus, and to not burden the NHS, for example, safe superovulation strategies reduced risk of ovarian hyperstimulation syndrome (OHSS). The clinic was required to have a strategy to prioritise patients on the waiting lists to be offered treatment in a fair manner. Those most impacted by the delay were given priority to start treatment when the clinic obtained one theatre list from the Trust in August 2020. Due to the pressure on the NHS services, the Hospital Trust could only provide the IVF clinic with one of its egg collection lists. Therefore, the number of egg collection performed on a Friday increased from a maximum of 3 to a maximum of 7 to prevent capacity dropping by a half. The clinic had to optimise the egg collection process even further to ensure timely starts and efficient handovers.
New equipment was introduced later in 2020, an enclosed hood for egg collections and three electronic heated stages. The third quarter of 2020 after the shutdown saw reduced ICSI success rates for the first 17 ICSI cases; however, this was likely due to poor prognostic patients being prioritised for treatment first (low ovarian reserve, reduced egg numbers and increased maternal age) as identified in weekly KPI clinical data (not shown).
Phase 2 and 3 changes were implemented postlockdown when new equipment was available and validated. The clinic switched ICSI injection media to handling media from March 2021 onwards following satisfactory review of data from split cases performed prelockdown.
Postimplementation of improvement strategies
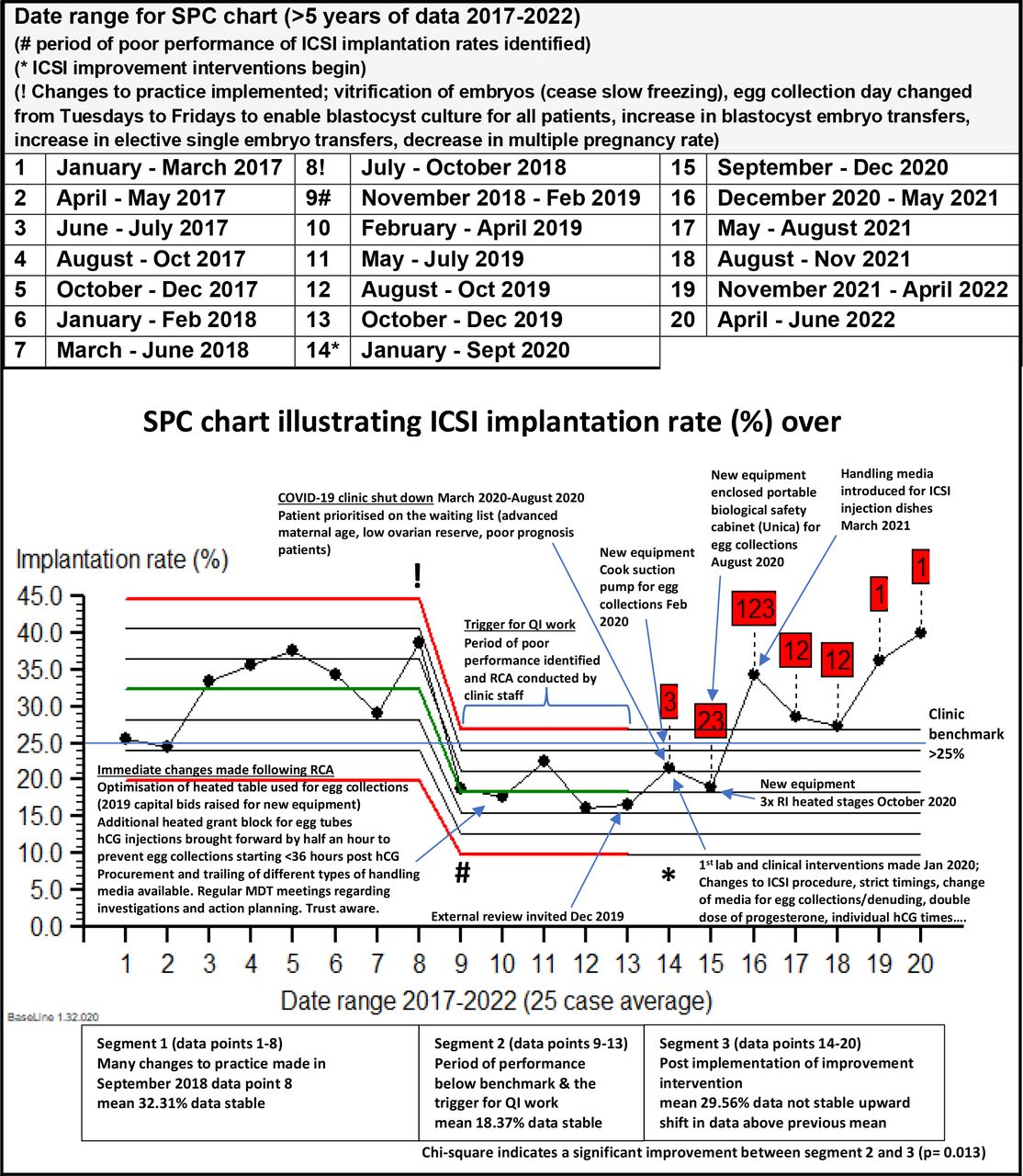
ICSI implantation rate was plotted over time on an SPC chart (BaseLine) as an average of 25 consecutive ICSI cases. At least 25 cases are recommended when monitoring pregnancy KPIs to provide a more accurate picture. These data included women <40 years old having fresh ICSI cycles. ICSI implantation rate over >5 years is plotted in the SPC chart (figure 1). Data points 3–8 June 2017–October 2018 show a shift towards a higher implantation rate. There is an opposite shift detected in the data for 6 points (9–15), from November 2018 to December 2020, of lower implantation rates over this period. This is a significant reduction in the implantation rate, as the clinic identified, and the reason for the root cause analysis and quality improvement work. The data are then split prognostically at the point that the intervention bundle was started to monitor any improvement in the baseline mean implantation rate that could be attributed to the changes made from the improvement work. The 7 data points postintervention implementation (from data point 14 January 2020) are all above the previous poor baseline mean of 18.37% implantation rate, and there are many signals present indicating a significant shift in the data. The first 2 data points postintervention are not as high as the other five. This is likely due to the impact of the COVID-19 pandemic as revealed when maternal age and egg collection number were plotted as a weekly average. Without the impact of this on the data, a bigger improvement might have been seen. Ideally, more points (at least 9) are needed to establish a new data baseline; however, the SPC chart highlights an upward shift towards a better implantation rate attributable to the changes made from January 2020, the 7 data points giving a mean implantation rate of 29.56% reaching clinic benchmark. More data points should be collected to ascertain whether the improvement is sustained and attributable to the intervention bundle that was introduced. The time corresponding to the period of reduced performance (data points 9–13, n=170) was compared with the postimplementation of improvement intervention period (data points 14–20, n=238) by χ2. The ICSI implantation rate significantly improved (p=0.013) (for data, refer to online supplemental information 3).
Supplemental material

{kind=link}
SPC chart showing ICSI implantation rate (%) over time. The data are split at the period of poor performance and locked at point 14 when the intervention was started (January 2020). There are two previous implantation rate means of 32.32% (period of 1–8 January 2017–October 2018) and 18.37% (period of 9–13 November 2018–December 2019). The 7 postintervention data points are all above the poor performance segment mean and all have signals (red flags 3, 2/3, 1/2/3,1/2, 1/2, 1, 1) which indicate special cause variation and an upwards shift in the data. The ICSI implantation rate significantly improved in the post intervention period due the changes that were made (p= 0.013, ChiSq). The mean postintervention was 29.56%. ICSI, intracytoplasmic sperm injection; SPC, statistical process control.
ICSI damage rate and fertilisation rate per consecutive 25 cycles over time were stable, with no special cause variation and means within benchmark (6.43% damage rate; 68.52% fertilisation rate) (see online supplemental information 4 for additional measure data). The proportion of mature eggs at ICSI, number of eggs collected and maternal age per average 25 cycles were stable with no special cause variation (mean proportion of mature eggs 82.34%, mean number of eggs 10.95, mean maternal age 33.12). But when potted, weekly maternal age was significantly higher and egg numbers were significantly lower than usual around the time of recommencement of treatment. This could partly be due to patient factors of those patients prioritised on the waiting list (advanced maternal age, low ovarian reserve, low prognosis patients). This period coincides with a period of poor pregnancy rate.
Supplemental material
A change of practice to a more cautious approach to ovarian stimulation and elective freeze all (FAE) cycles may have impacted on the post intervention success rates. The number of FAE cycles had increased in 2020/2021 from 3.4% of cycles in 2019 to 10% in 2021. Patients most likely be better prognosis (good responders to stimulation) who are then removed from the fresh ICSI cycle data by not having an embryo transfer and therefore skewing the data.
Lessons and limitations
Due to the urgency and commitment of the clinic to improve its fresh ICSI success rates many changes were made at the same time. Ideally, it would have helped us identify the more effective interventions by having many PDSA cycles and changing only one parameter at a time. This approach was not selected because of the inherent delay in outcome data and low cycle numbers meaning that immediate improvement might not be seen when testing interventions separately. Something that the team were not prepared to do. It was more responsive and ethical to implement a bundle of interventions aimed at addressing all possible causal factors, based on best practice and an external review, for patient care. This felt more ethical, responsive and low risk as none of the interventions were expected to reduce performance. However, this approach was more expensive as some interventions (eg, purchase of new equipment) had an associated cost to the clinic and this ‘bundle’ approach would complicate attribution of improvement to specific changes made.
The improvement project was affected by the COVID-19 pandemic, which cut short a promising improvement trend in fresh ICSI success rates in the first quarter of 2020. Additional changes to the service and procedures were required in response to the pandemic when the clinic reopened for fresh cycles in August 2020 to enable treatment to resume safely during the COVID-19 emergency while maintaining compliance with regulatory requirements. This period affected the initial fresh cycle results in many ways including theatre use, staff and patient well-being, the prioritisation of patients on the waiting list and a more cautious approach to OHSS. It was reasonable to prioritise patients in whom delay was most likely to significantly affect the outcome of treatment.18
Although improvement was observed during this study, it required a longer amount of time to show this on an SPC chart due to the shutdown period and reduced activity of a small fertility clinic which already had low fresh cycle volumes. An increase in FAE cycles reduced the fresh cycle data further. The improvement work was not as responsive as was desired. The statistical KPI monitoring system demonstrated by the current study may be more effective at identifying KPI shifts in larger clinics with higher cycle volumes.
An additional learning from the RCA was that any operational change that might impact the fertility clinic needs to prompt an impact assessment of downstream processes.
Conclusion
The clinic was able to detect a drop in its fresh ICSI implantation rates through monitoring KPI’s. Due to the low cycle volumes at the clinic, the trend was picked up over an extended time period. There is no agreed optimal protocol or pathway for ICSI, processes vary from clinic to clinic, a much-needed ICSI best practice paper is due for publication. The clinics clinical and laboratory team used a series of quality improvement tools, root cause analysis, literature review and input from an external review to identify potential problems with the fresh ICSI pathway and protocols, developing interventions that addressed these areas for improvement. Implementation of the interventions improved the fresh ICSI implantation rates significantly but the COVID-19 pandemic and treatment recommencement in 2020 had an impact on the improvement work. Extended time was required to ensure sufficient data was available to establish if the interventions resulted in an improvement, making the improvement work less responsive than desired.
Balancing measures provided important information to a complex system helping to inform how the system’s performance changed over time and provided possible explanations. Monitoring the KPI measures as weekly averages displaying variation over time helped to identify and interpret patterns that might otherwise have been missed for example, egg numbers and maternal age.
Both the changes made, and improvement has been sustained within the clinic with no drift in adherence to protocols. This was possible due to a small team with excellent engagement and commitment from all staff. The clinic will continue to closely monitor the KPI, and more data points on the SPC charts would help to demonstrate whether there was a significant and sustained improvement due to the changes made.
It is worthwhile disseminating this root cause analysis and improvement work to the assisted conception field as there are limited published reports where embryology KPIs are tracked following defined and controlled laboratory or clinical changes.1 This project could be more effective within a larger clinic with higher cycle volumes. Interventions made within this project may not be effective or suitable within other clinics due to each clinic’s unique patient population and ways of managing workloads. Each clinic would need to be informed by its own data analysis on the optimal ICSI procedure.
The next steps for the clinic to continuously improve its fresh cycle success rates and to increase capacity would be to provide more flexibility to egg collection days.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
All the clinic staff and the external observer, Bryan Woodward, for their involvement and contributions to this project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Clinic staff provided and cared for study patients. EW completed the data collection, reporting of the work, and is responsible for the overall content as guarantor. MC was the academic supervisor of EW and reviewed drafts of the report.
Funding Clinical Doctorate Training in Clinical Science funded by Health Education England, no award/grant number.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.