Article Text

Abstract
Introduction Modern safety approaches in healthcare differentiate between daily practice (work-as-done) and the written rules and guidelines (work-as-imagined) as a means to further develop patient safety. Research in this area has shown case study examples, but to date lacks hooking points as to how results can be embedded within the studied context. This study uses Functional Analysis Resonance Method (FRAM) for aligning work-as-imagined with the work-as-done. The aim of this study is to show how FRAM can effectively be applied to identify the gap between work prescriptions and practice, while subsequently showing how such findings can be transferred back to, and embedded in, the daily ward care process of nurses.
Methods This study was part of an action research performed among ward nurses on a 38 bed neurological and neurosurgical ward within a tertiary referral centre. Data was collected through document analysis, in-field observations, interviews and group discussions. FRAM was used as an analysis tool to model the prescribed working methods, actual practice and the gap between those two in the use of physical restraints on the ward.
Results This study was conducted in four parts. In the exploration phase, work-as-imagined and work-as-done were mapped. Next, a gap between the concerns named in the protocol and the actual employed methods of dealing with physical restraint on the ward was identified. Subsequently, alignment efforts led to the co-construction of a new working method with the ward nurses, which was later embedded in quality efforts by a restraint working group on the ward.
Conclusion The use of FRAM proved to be very effective in comparing work-as-done with work-as-imagined, contributing to a better understanding, evaluation and support of everyday performance in a ward care setting.
- patient safety
- nurses
- continuous quality improvement
- qualitative research
- compliance
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Research efforts in modern patient safety approaches like Safety II and Resilient Healthcare use the Functional Resonance Analysis Method (FRAM) as a method to highlight sources of performance variability and resilience. While this is also the case for studies investigating the tension field between work-as-imagined and work-as-done, it remains unclear how FRAM can benefit the ongoing improvement of patient safety through embedding research findings into practice.
WHAT THIS STUDY ADDS
Our study shows that FRAM is an effective tool to address the tension field between work-as-imagined and work-as-done for nurses on a hospital ward. Results illustrate how quality and safety in nursing can be addressed bottom-up together with stakeholders.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study provides a roadmap for the use of FRAM as a tool to integrate research findings from a Safety II perspective into practice, offering new directions for quality improvement studies interested in further improving patient safety by expanding on practices and skills that are already present within nursing teams.
Introduction
In recent years, there has been an increasing interest in the theories and methods behind the concept of Resilient Healthcare (RHC) and Safety II (S-II).1–3 Although progress has been made, the exact and sustained contribution of RHC has yet to be determined.4 5 The S-II perspective illustrates a renewed interest in the understanding that work can be imagined in a certain way, but in practice is often different. Dealing with the tension field between the ideal (documented) care and the reality is important, but it is also necessary to take the strategic considerations and practical challenges6 into consideration.
Ward care is no exception because the often unpredictable and busy nature of the work makes it a place where everyday care is difficult to manage or improve.7 While adherence to clinical and nursing guidelines is a necessary starting point, most clinicians and nurses would agree that deviations from standards are equally important to meet the unpredictable course of events inherent in treating unstable ward patients.8–11 This means that the actual performance of work can differ (significantly) from how it was intended.
The traditional approach for most hospitals in accounting for quality and patient safety is predominantly found in compliance, rules following through guidelines and protocolisation. At the same time, ward nurses are expected to deal with unexpected changes12 on a day-to-day basis, at times favouring departure from the standardised and expected to meet the challenges at hand. In managing such challenges, new directions for improving patient safety could be already present in daily practice but remain undetected by conventional quality approaches.
In the literature on RHC, this dilemma is illustrated by highlighting the difference between work-as-imagined (WAI) and work-as-done (WAD).13 WAI reflects the way in which we think that work is or should be performed. It reflects the desired working standards, often embodied in guidelines and protocols, improvement plans or rules. WAD, on the other hand, is the way in which these working activities take form in actual practice: it encompasses how healthcare workers give substance to the work that needs to be performed (which may or may not include desired procedures and working methods). A structural gap between WAI and WAD might have negative consequences for patient safety,14 but can also be difficult to detect.15 Engaging nurses in finding this gap could have positive influences on patient safety16 and job satisfaction,17 through which it is a promising step in operationalising S-II.18
Most studies examining WAI and WAD differences use the Functional Resonance Analysis Method19 (FRAM) as a tool to map how imagined and actual performance differ. FRAM is a modelling method used to map a set of activities, instances and/or an entire process in sociotechnical systems19 20 and has been used in previous research to align WAI with WAD.21–23 Detecting unwanted performance variability within or between the two can highlight potential points of improvement. Consequences of this variability have to be examined in light of the current process. Targeted improvements can then be implemented and ideally sustained.
Interestingly, little attention has been paid to how narrowing the gap between WAI and WAD can be achieved for longer periods of time. This is important, since existing practices can change, with the risk of reasoning from an outdated picture. Many studies however approach WAI and WAD at an explorative angle or aid in the initial planning and design phase of quality improvement interventions.21 23 Few examples exist as to how FRAM can contribute to narrowing the WAI and WAD gap in the long run.21 23 The often complex processes targeted in these studies remain at an interplay between different stakeholders inside and outside the primary process itself, offering little certainty if indeed the appropriate route is taken and maintained.
Few empirical examples exist as to how FRAM as a method can directly contribute to applying and embedding WAI and WAD differences in everyday clinical work. This study aims to find an explorative but systematic approach for pinpointing new directions in improving patient safety. By using a concrete example of a nursing intervention on a hospital ward, the objective of the study is to investigate how FRAM can effectively be applied to decrease the gap between WAI and WAD. The study also investigates how subsequent findings from an FRAM analysis can be transferred back to, and embedded in, the daily ward care process of nurses.
Methods
Design
This study was part of a larger ethnographic action research project, focused on (1) increasing the discretional space of the ward nurses and (2) understanding the dynamics of how WAI and WAD differ from the perspective of the ward nurses. The theoretical background is rooted in resilience engineering and used the WAI–WAD gap as a framework for understanding the tension field between prescribed and actual working activities. As the WAI–WAD gap is essentially influenced by the perspectives of the actors involved, the present study follows an interpretivist approach as rooted in traditional ethnographic research.
Contributing to the action research, JT performed an ethnographic inquiry between February 2020 and October 2020 aiming to get acquainted with the wards context, healthcare professionals and culture. This allowed understanding of contemporary working methods and interdisciplinary collaborations on the ward. The usage of physical restraint was observed as of notable interest by the wards’ nurses and management, since neurological patients on the ward are prone to confusion and at-risk behaviour, making them a potential risk to themselves or others around them. With the larger action research in full progress during October 2020 and June 2021, the researcher JT also joined the wards’ nurse-led workgroup concerned with appropriate physical restraint application on the ward. During this period, the role of the researcher changed from being an accepted spectator on the boundaries of the group to being a more engaged action researcher collaborating with the ward nurses on a daily basis.
Setting
This study took place on a combined neurological and neurosurgical ward with 38 beds in a tertiary referral centre. Primarily ward nurses were included in the study, as well as eight members of a nurse-led physical restraint working group, one physician assistant and clinical and nursing management of the ward.
FRAM
FRAM was used as an explorative and iterative method to map, analyse and discuss differences between WAI and WAD with stakeholders on the ward. In short, an FRAM starts with determining the tasks or activities relevant to the modelled case or process, called functions. The amount and level of detail of the functions depends on the underlying aim of developing the FRAM. Findings during the FRAM construction can guide the level of detail necessary to arrive at greater understanding. Once a set of functions is determined, the relationships or couplings between the functions are made. Coupling between functions can be made by indicating the relevant features or dimensions of that function—called aspects. Aspects include Input (I), Output (O), Precondition (P), Resource (R), Time (T) or Control (C). These aspects help map and understand the nature of the coupling between the functions of the FRAM. Functions can thus be coupled in multiple ways, but always in such a manner that the Output (O) of a function forms a connection to at least one of the five other aspects of another function (I, P, R, T, C). See Clay-Williams et al21 for a detailed explanation of FRAM in a clinical setting.
Data collection and analysis
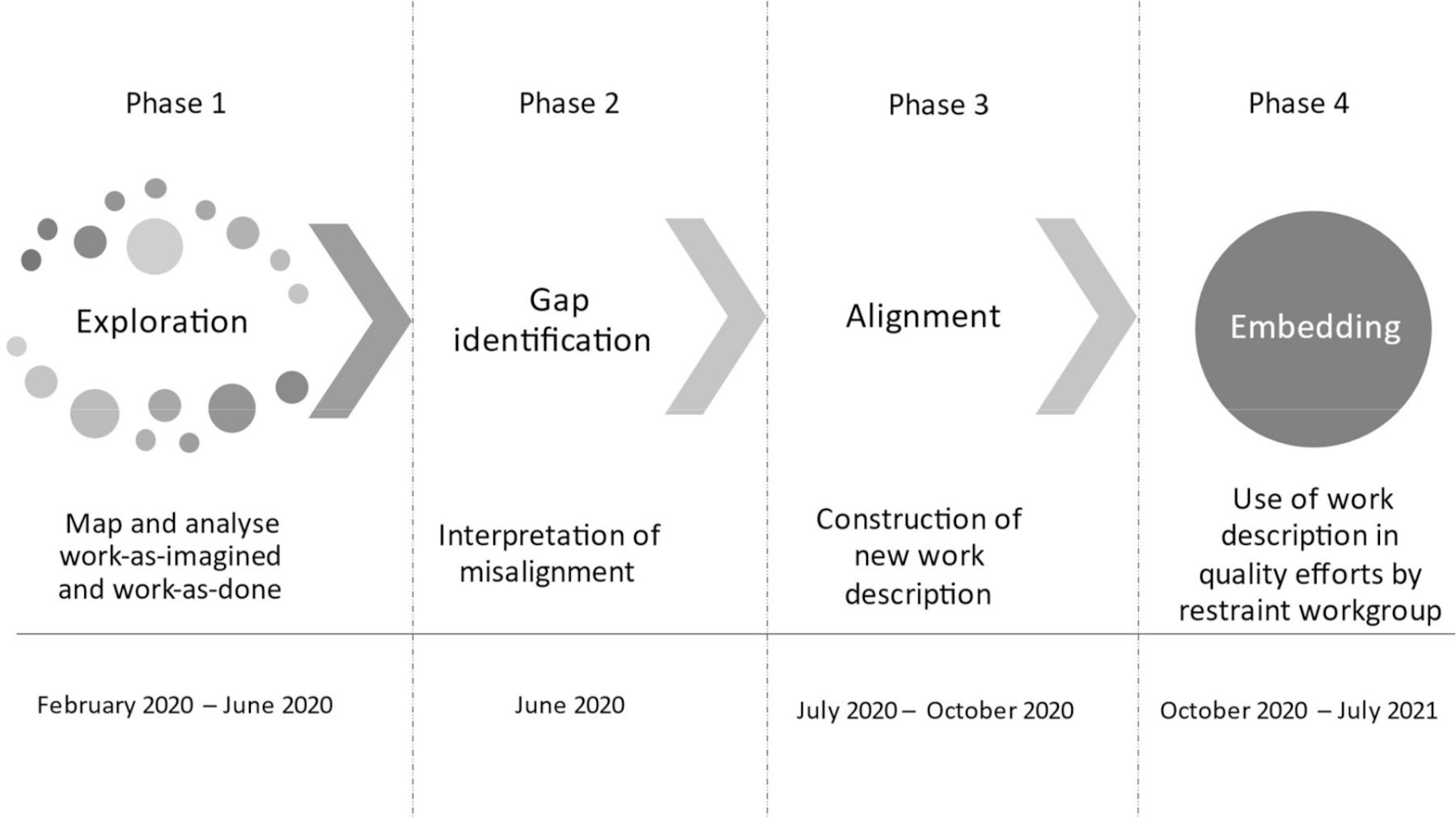
Data was collected through participant observations, both semi-structured and unstructured interviews, individual and group discussions with stakeholders on the added value of a hospital-wide protocol of physical restraints versus the actual use of restraints by nurses on the ward. During the observations, data was collected through in-field jottings later elaborated on in-field notes. Data from the interviews was collected through note-taking and writing comments in the FRAMs. All data was organised in a separate research diary, reflecting recurrently on the role of the action researcher. Modelling of the FRAM was done using the FRAM model visualiser, and the FRAMs (WAD and WAI) were printed for the interviews. The FRAMs were constructed iteratively until a clear comprehension of WAD and WAI was achieved. Data for FRAM development and discussion was collected during the period from February 2020 to June 2020. Based on the interpretation of the gap between WAD and WAI, a three-page working method was written, printed, discussed and revised in person with ward nurses, eight members of the wards’ nurse-led physical restraint working group, one physician assistant and clinical and nursing management of the ward between July 2020 and October 2020. Management gave their feedback and agreement digitally and during regular quality meetings on the ward. From October 2020 to June 2021, the researcher JT made in-field observations kept in an action research diary when engaged with the topic of physical restraints on the ward. The whole iterative process of data collection, processing and analysis is discussed in detail in the findings section. The research steps of the study are shown in figure 1.

Research steps. In the ‘exploration’ and ‘gap identification’ steps, work-as-imagined and work-as-done were mapped, analysed and discussed with the wards’ nurses. In the ‘alignment’ and ‘embedding’ steps, action researcher JT collaborated with the nurses to make explicit their working methods in a new work description, which was later used by the restraint workgroup to address quality and safety issues concerning restraint use on the ward.
Reflexivity
With no background in medicine or nursing, but a masters degree in cognitive psychology and a theoretical background in (patient) safety literature, the researcher JT had little assumptions or prior experiences with ward care. JT was supported by DV, a supporting quality advisor new to the field of medicine but with extensive experience in the application of FRAM in several safety critical domains.
For the informed consent procedure, ward management regularly communicated the researchers’ presence on the ward. Participation in the study and consent was obtained verbally before and during observations, interviews and discussions. Data was anonymously processed during analysis and could not be related back to individuals. Data was stored securely within a data safe folder of the participating hospital.
Patient and public involvement
Aside from patient treatment being inseparable from participant observations on the ward, patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Findings
Exploration phase
During the first phase (table 1), identification of WAD started with participant observations on the ward and subsequent construction of an FRAM (FRAMwad). In turn, input for WAI was based on the current applicable hospital-wide protocol for physical and environmental restraints and the respective work documents forming the input for a separate FRAM (FRAMwai). After the initial FRAMs were developed, researchers JT and DV conducted single and group open-interviews during phase two, discussing both FRAMwad and FRAMwai until a clear comprehension of both FRAMs and the gap was reached. The output of each interview was used to further refine both FRAMs.
Research process of building FRAM models of work-as-imagined and work-as-done
The FRAM analyses not only served as input for discussions with nurses on the ward but were equally important for data capturing and analysis during the interviews, propelling deeper understanding of WAI–WAD differences. Furthermore, discussing the printed FRAMs allowed for open dialogue between the participants, reflecting on the contemporary working methods and the appropriateness of the related WAI. An important aspect of the interviews was to clarify to the participants that the researchers were not judging working methods on efficiency or adherence to the protocol per se, but were merely interested in how the participants go about their day (FRAMwad) and in what way the protocol was helpful in this respect. Presenting both process perspectives in two FRAMs on A3 paper helped to verbalise, capture, discuss and trim the FRAMs during and after the interviews. Appendix A and B show both FRAM’s as used during the last group interview.
Supplemental material
Identification of gap
The discussions with the nurses revealed both nuances and important mismatches between protocol and actual working practices. Since physical restraints are a complex intervention, an elaborate description of the FRAMs’ pointing out in more detail the fundamental differences between WAI and WAD for physical restraint use on the ward can be found in Tresfon et al (2022, currently submitted to Global Qualitative Nursing Research).
The differences could be related to practical issues (eg, protocols were hard to find) as well as substantive issues in which the protocol made no references to some activities that were important aspects of dealing with restraints on the ward. Detailed nuances could be found in, for example, informing the physician, family members and/or legal representatives after the physical restraint had been applied in acute cases. Other differences were more drastic, such as the continuous collaboration between nurses in identifying appropriate measures to take, as opposed to the upscaling step-by-step approach mentioned in the protocol. Such an example of WAD illustrated physical restraint use as both an individual and teamwork skill of nurses in an uncertain clinical process. WAI however relied heavily on the judgement of a physician whenever a physical restraint was considered.
In general, the comparison between WAI and WAD uniquely revealed that:
The protocol was limited useful for the nurses. This was due to the multitude of documents, as well as that the protocol followed strict categorisations of environmental and physical restraint types, which were not recognised as such by the nurses.
Consequentially, reporting and evaluation of physical restrains through separate forms within the electronic patient record was only done to a varying degree by the nurses. The ward nurses preferred to discuss the details of the patients’ current situation verbally during handovers.
The nurses engaged in several tactics to distract or comfort the patient in times of confusion, preventing subsequent at-risk behaviours from becoming unmanageable and physical restraint use from being necessary. In fact, the nurses initially try to prevent confusion from occurring by monitoring and mitigating signs of restlessness, an indicator for nurses that a patient can become confused. The protocol did not mention restlessness as such, stating none of the tactics for dealing with restlessness and just a few for dealing with confusion.
The application of restraints is a shared process in which the nurses collaborated continuously, making use of each other’s experience and skills when deciding which physical restraint to apply and during the application process in general. The importance of cooperation, nursing experience and skill was not reflected as such in the protocol, showing a greater tendency to consult the physician at given stages in the step-by-step approach.
Alignment
The findings from the gap between FRAMwad and FRAMwai were used to construct a new description of the working methods on the ward, reducing the number of pages considerably and changing the phrasing from a directive check-and-balances tone of voice to a more friendly and helpful kind of writing. Also, five actionable questions constructed as ‘steps’ formed the root of the new working method (table 2).
Questions guiding the new work description of physical restraints on the ward
Initially, the working method was member checked with several ward nurses. They were asked if the nurses would be confident that a new colleague whom had taken the mandatory theoretical and practical teachings, knew the appropriate actions to take based on the working method. After that, together with a nurse-led physical restraint working group on the ward, the working method was collectively refined. During this session, the concept of restlessness was untangled from confusion and highlighted by the nurses as not only something fundamentally different but also coined as a nursing indicator that a patient can become confused and develop at-risk behaviour.
Embedding
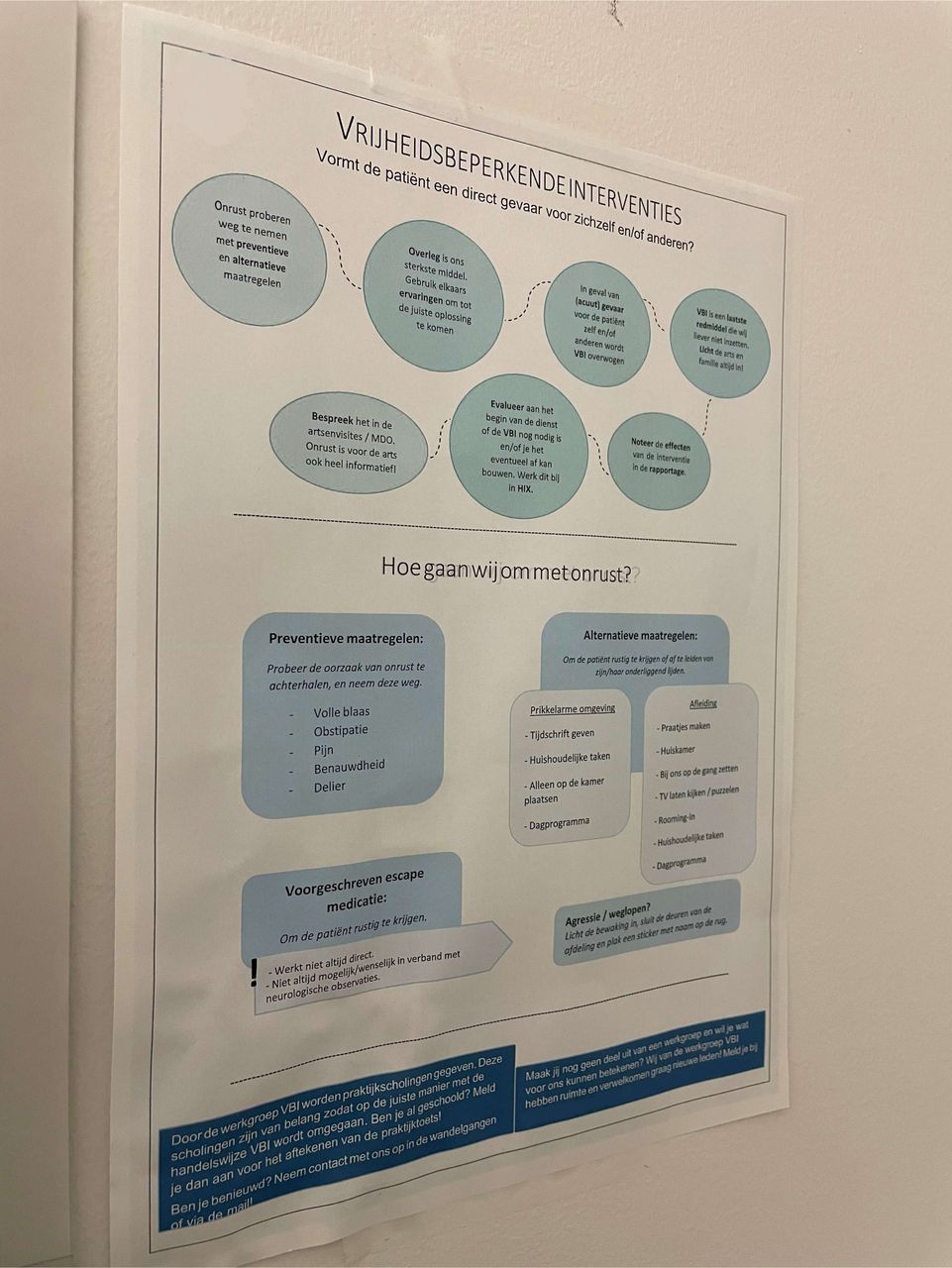
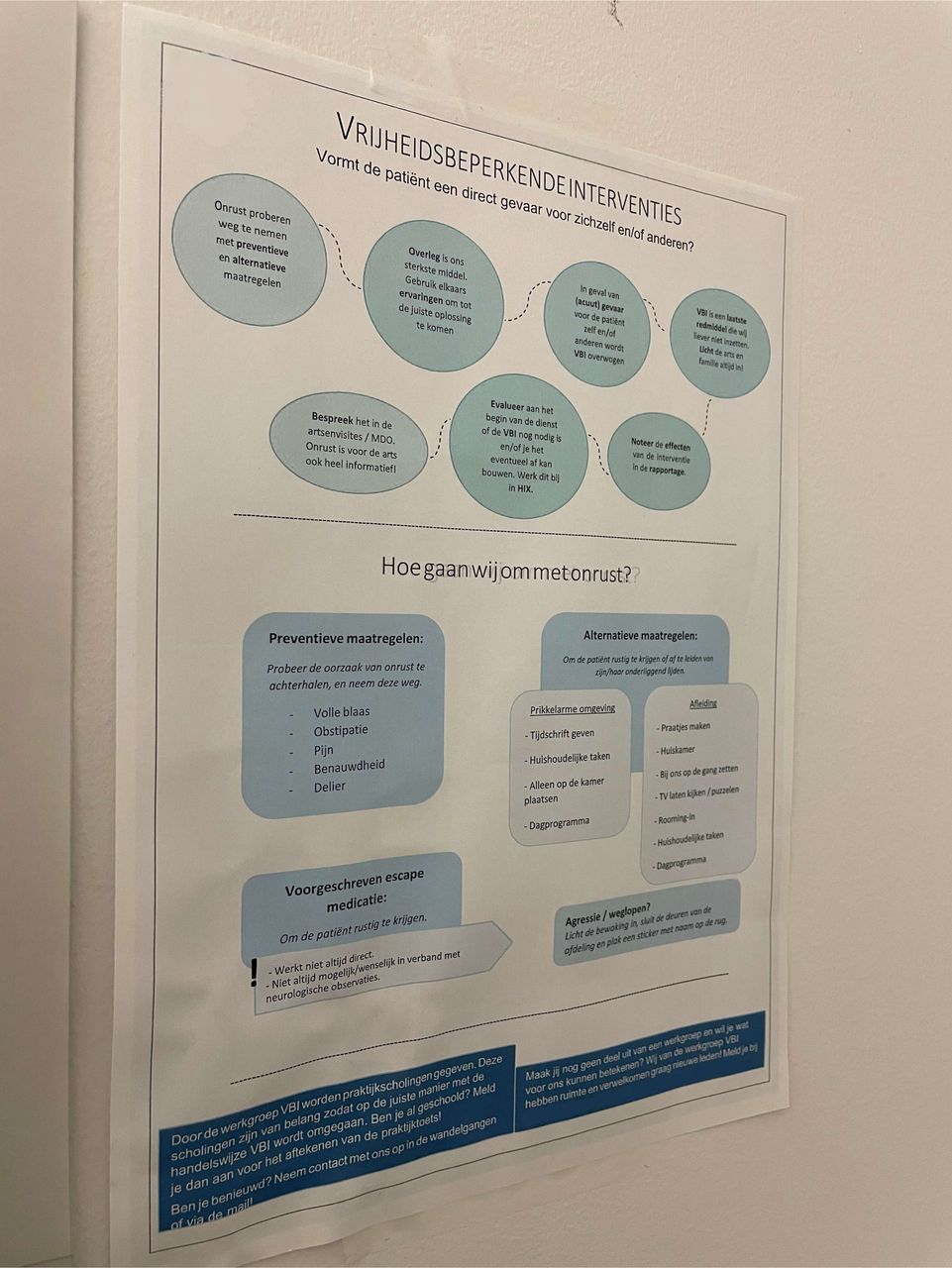
After clinical and nursing management, as well as a physician assistant on the ward, reviewed the description minor modifications were made. While making their current working methods explicit two quality and safety issues on the ward were found by the physical restraint work group. An organisational problem was identified in the arbitrary reporting and evaluation of restraints in the electronic patient records. This reduced data reliability of the physical restraints performance indicator (see table 3). For the ward, it was believed important to refresh the working methods among contemporary nurses and educate new employees in the same manner. The working description was adopted by the physical restraints workgroup as a supplement to the protocol and used as a supporting tool during practical teachings of physical restraint usage to new colleagues on the ward. In the following months, two nursing students whom joined the restraints workgroup used the work instruction as a basis for a poster campaign on the ward. The campaign was held during the ‘physical restraint week’, a period with daily reminders, practical and theoretical teachings in the use of physical restraints on the ward (figure 2).
Overview of registered cases of physical restraint evaluation
{kind=link}
{kind=link}
Poster campaign. Similar posters were distributed and hung up throughout the ward at ingenious spots by the nursing students (eg, next to the printer, in the changing room, on the wall of work stations on the ward). Here, the poster hangs in the wards’ restroom.
Discussion
When comparing WAI with WAD, the use of FRAM yielded meaningful results in narrowing the gap between WAI and WAD. While WAI was insufficient in addressing the challenges met in practice, handling restlessness and confusion in daily practice (WAD) was found to be a collaborative nursing skill vital for mitigating and reducing restraint application. Besides, this skill was already taught to new colleagues and students on the ward, out of sight of hospital quality structures, causing the quality indicator to be misleading and the protocol of limited practical use for the nurses. Due to our iterative approach and active involvement of the ward nurses in the process of redesigning WAI itself, the quality improvement efforts in the study were directed by reflection on contemporary practices.
FRAM proved to be a helpful method, not only for understanding and comparing WAI with WAD, but also as an aid to stimulate the conversation about working practices during the interviews. FRAM provided the ward nurses with prompts to reflect on their working practices collectively. These reflections also offered a point of reference against which the prescribed (imagined) descriptions of work could be equally weighted. The active involvement and participation of the ward nurses during the FRAM discussions was paramount. Indeed, the continuous collaboration of the researchers with the ward nurses and other stakeholders helped to understand the interests of the people performing the actual work, while also allowing for a supportive base when co-constructing the new working method. Consequently, the constructed new working method showed how insights from an FRAM analysis can be translated toward a workable form of reflection on working processes in the nursing domain.
Taking guidelines, work instructions and protocols into account when reflecting on current practices also showed its value. WAI underappreciated meaningful aspects of WAD on the ward with important consequences. For instance, the monitoring done through recorded indicators was based on a skewed picture of reality as the nurses did not find the digital evaluation form helpful. This in turn limited the organisations’ ability to effectively monitor performance, while missing vital aspects of the nurses work in restraining. Furthermore, since physical restraints are a potentially dangerous intervention for patient safety,24–26 the skills of managing signs of restlessness and collaboration could be further stimulated and supported as a means to decrease the total number of restraint applications. As such, restraint-related falls could potentially be reduced. Such improvements cannot be achieved by only being strictly compliant to the protocol. By making the current work agreements explicit within the nursing team, alternative directions for improving patient safety became apparent.
Our explorative approach offers a new direction for institutions seeking to understand why WAD is not in line with WAI. It can also be used for quality and patient safety improvement studies by expanding on practices and skills that are already present within nursing teams. To improve care, appreciation is needed that deviations from WAI are not exceptions to the rule, but an inherent part of work in complex sociotechnical systems.27 While guidelines, protocols or work instructions can be a starting point for reflecting on WAD, this can also be a challenge in itself.2 28 In the patient safety literature, rule-following and the deviations have frequently been examined. This suggests that pragmatic and normative causes can be identified but both remain difficult to manage in general, since the context highly influences the appropriateness of deviation or the need for strict rule-following.15 29 30 Actively managing the gap between WAI and WAD could offer valuable directions for appreciating and acting on the tension between WAI and WAD.
In the S-II and RHC literature, FRAM is often used as a tool to understand the nature of adaptions in variable performance.4 31 32 While it has been demonstrated how this method can contribute to detecting important adaptations within clinical processes, few examples illustrate how such recommendations can be embedded within the actual work. Other applications have specifically aimed to determine the gap between WAI and WAD using FRAM.21–23 Examples indicate a need for a reassessment of practice variation and protocol compliance, or show how pre-adjustments in WAI can be made to better suit WAD. However they fail to recognise which actors within the clinical processes would benefit the most from such tasks, while our study illustrates how these stakeholders can be identified and included in realignment efforts throughout.
Highlighting where adaptive behaviour exists and where it deviates from WAI is the starting point for discussion and reflection between the involved professionals. In realigning WAI with WAD using FRAM, the tension field inherent between the two conceptual viewpoints on work as such should not be limited to picking a side (ie, ‘Forceful compliance vs anything-goes’), but should remain a continuous point of discussion and reflection throughout the organisation2: did the frontline professionals meet WAD as they intended? And is the WAI still helpful in this instance? Our study shows how FRAM can pinpoint such conversational topics or be used as a starting point for the conversation.
To our knowledge, this is the first study to illustrate how results from WAI–WAD comparison can be embedded in existing nursing practice. The new constructed working method reveals how FRAM can contribute to redesigning a working method in such a way that it better represents actual working practices while upholding presently existing requirements and system boundaries. Also, the description provided a useful tool for the education of nurses in appropriate working methods on site. Remarkably enough, FRAM has little value when limited to mere insights in working practices for researchers and left unattended on the drawing board. FRAM should be used as a structured conversational tool for allowing a discussion free from value judgements about the work with frontline health workers. The same goes for the continuous involvement of stakeholders in the FRAM process and for continuous reflection on the appropriateness of existing and newly derived working methods. Our explorative approach offers other institutions a roadmap for using S-II and RHC methods when struggling with a WAI–WAD gap.
Limitations and strengths
Our study reports on directions for improving patient safety, rather than a quality improvement report per se. A limitation of the approach used in the present inquiry is that the comparison between WAI and WAD is always highly specific to the organisation: which protocol(s) are in place, as well as common working methods used on the ward under study. However this does not pertain to limit the value of comparing the WAI–WAD gap with FRAM and subsequent discussion within the team, nor the development of a new working description. What can be problematic, is the time-investment made by the researchers and nurses to detect and realign WAI and WAD. Nevertheless, the WAI–WAD gap showed that the conventional quality instruments unsuccessfully address and misinterpret important aspects of the nurses’ work, which makes the time-person investment to use FRAM very worthwhile.
Although the study took place during the COVID-19 pandemic, distorting effects are believed to have been limited as the nursing team composition remained mostly intact during the study period. However, the anti-COVID-19 measures placing a maximum number of people allowed in meeting rooms was believed to influence the effectiveness of the quality control work, and as such, the physical restraint working group on the ward.
A strength of the study can be found in including different perspectives on work toward the same process and reflecting on it with stakeholders. The conceptualisation of WAI and WAD thus does not stop at a research area of RHC and S-II. This argues for a need toward a more reflexive, explorative and case sensitive research approach as opposed to working with rigid and stale designs.33 Indeed, the complexities of the clinical environments arguably call for in-depth qualitative work to understand the local norms and habits, and to ensure that meaningful differences are indeed appropriately addressed and retained.34 Also, expertise in human factors and safety within the quality department could be beneficial for managing the WAI–WAD gap. To achieve this in other contexts and hospital environments, our study indicated that FRAM can be used as a starting point by comparing and aligning WAD with WAI.
Conclusion
With FRAM the mismatches between WAI and WAD can brought out effectively, and the two can be aligned and embedded in everyday ward care. Discussing common practices on the ward revealed hooking points to improve and maintain dealing with specific patient safety issues. Combined with a curious and appreciative stance toward frontline health professionals during a continuous improvement approach, FRAM proves to be a very effective technique to align WAD with WAI, contributing to a better understanding, judgement and support of everyday performance in a ward care setting.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but Medical Ethics Review Committee Leiden Den Haag Delft exempted the study under reference number N20.019/ML/ml. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank all the nurses of the neurological and neurosurgical ward and other hospital staff whom participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to the conception and design of the study. Interviews were carried out by JT and DV. DV oversaw the FRAM development and analysis process together with JT. Member checking new work description was done by JT and DV. Embedding of work description was done by JT under supervision of KL, AHB-R and JH. KL, AHB-R and JH contributed to the interpretation and reporting of the qualitative data and reviewing the work critically. JH oversaw the research process. JT as guarantor developed the original manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.