Article Text

Abstract
National Health Service (NHS) clinical staff are required to demonstrate involvement in quality improvement (QI) and patient safety. Clinicians are often best placed to identify problems and design solutions for their own clinical environments, yet the rotational nature of training can impact on the design, implementation and sustainability of projects.
The In-hospital Quality Improvement for Respiratory team was created in August 2020 within a busy respiratory department to inspire a culture of continuous improvement and provide a sustainable infrastructure to support and progress QI projects (QIPs).
The trust uses the LifeQI platform which provides a change score from 0.5 (intention to participate) to 5.0 (outstanding sustainable results) as a representation of a QIP’s progress.
We aimed to increase the number of QIPs in the respiratory department registered on the LifeQI platform from 1 to at least 10 projects by September 2021.
A QI framework was used to identify and address four primary improvement drivers: (1) QI understanding/training, (2) QI faculty communication, (3) QI participation, and (4) QIP completion using multiple Plan-Do-Study-Act cycles. Data were collected on the number of active respiratory projects registered within the LifeQI platform, mean LifeQI change score and the number of projects with a change score ≤1.
Twenty-four new QIPs were initiated in the first 12 months, with a number of projects leading to sustainable change. The largest improvements were seen in autumn 2020 as the faculty’s multidisciplinary membership expanded.
We achieved our aim of increasing the number of registered QIPs, sustaining the QI faculty throughout the COVID-19 pandemic. Our multidisciplinary membership continues to increase and the faculty has improved access, organisation and project progression across a large department with an established process for rotating staff to join existing QIPs. Our model has the potential to be replicated in other clinical departments within NHS organisations.
- Quality improvement
- Clinical microsystem
- Continuous quality improvement
- Hospital medicine
- PDSA
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Engagement in quality improvement (QI) work is a requirement for all doctors in training and allied health professions. However, access to supported environments and supervision for QI is variable.
It is unclear at present how multidisciplinary staff members interact in their team-based environments to deliver improvement. There is often a disconnect between the intrinsic drivers of delivering safe patient care with the highest quality and the extrinsic needs to fulfil the curriculum of many healthcare professions which mandate active participation in improvement work.
Clinical microsystems can be defined as a small group of individuals, such as healthcare professionals, patients and sometimes their carers to deliver care for a defined population of patients. The use of clinical microsystems delivers good impact on clinical and educational outcomes. The use of these microsystems is often limited to chronic health conditions with a stable permanent staff group, the use of a microsystem in a staff group that often rotate every 4–6 months is less well known.
Our QI faculty was created as a novel approach to organising, supporting, promoting and sustaining QI within a busy medical department with rotational staff.
WHAT THIS STUDY ADDS
Our study demonstrates the importance of developing multidisciplinary QI faculties that can support and coordinate departmental staff to help deliver meaningful QI programmes across a department, enabling an environment where continuous improvement can embed and grow. This is opposed to the often short-term improvement projects that are sometimes limited to individuals rotating frequently through a department.
The study suggests that with the support of a mentoring and coaching QI faculty, we were able to increase the number of registered QI programmes within the department and demonstrate advancement of these projects through the LifeQI progression score. The study has also shown a steady growth in numbers of the core members of the QI faculty with a widening multidisciplinary membership. The respiratory QI faculty is now approaching 2 years now, and in itself has shown sustainability.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our work has shown that departmental QI faculties can support the delivery and sustainability of QI work in busy rapidly changing medical environments.
The study suggests the departmental QI faculties could be a potential mechanism of developing mentoring within a department, allowing continuity of QI programmes and an avenue towards a culture of continuous improvement.
This has the potential to ensure future improvement programmes enable staff closest to the problems have the permission and support to improve them.
Problem
In 2019, only one registered quality improvement project (QIP) was undertaken within our department despite a number of audit action points and patient safety incidents from previous respiratory clinical governance meetings.
The In-hospital Quality Improvement for Respiratory (InQuIRe) team formed in August 2020 as a QI faculty at a large teaching hospital trust with two acute hospital sites that serve a population of 1 million. There are four 30-bedded respiratory wards across the trust. The respiratory services also have a number of general and specialist clinic services including facilities for bronchoscopy, endobronchial ultrasound and thoracoscopy. Foundation year (FY) and internal medicine trainee (IMT) doctors rotate every 4 months, specialist registrars (SR) and senior clinical fellows (SCFs) annually.
All projects are encouraged to be registered through the LifeQI platform.1 This is a web-based system for centralised registration, recording and collaboration of improvement work. This allows the trust, departments and individuals to have oversight of all active QI work in their area. The software enables creation of a project aim, driver diagrams, clear documentation of Plan-Do-Study-Act (PDSA) cycles and collection of data with automatic creation of run charts.
The LifeQI change score is a useful tool as a rapid, visual representation of a QIP’s progression. QIP members are encouraged to regularly review and amend the change score for their project. The scores range from 0.5 (intent to participate), increasing by 0.5 points each step along the change journey up to 5.0 (outstanding sustainable results). Detailed descriptions of the LifeQI change scores are available in online supplemental appendix 1.
Supplemental material
We aimed to increase the number of QIPs in the respiratory department registered on the LifeQI platform from 1 in August 2020 to at least 10 projects by September 2021.
Through the creation of team InQuIRe our secondary aims included increasing the understanding of QI methodology, participation and engagement in QIPs across our department.
Background
All clinical staff are required to demonstrate involvement in QI and patient safety,2–5 and current training scheme requirements state that doctors in training should contribute to6 7 and lead8 QI initiatives. Indeed, clinicians are often best placed to identify problems and design solutions for their own clinical environments.9
Furthermore, the rotation of medical staff through hospitals in a region should be viewed as an opportunity to share good practice across different trusts and to bring new ideas to solve long-established problems. However, the frequency of job rotations can make the design and implementation of QIPs difficult, resulting in narrow or simplistic projects. Embedding change to sustain results beyond the next rotation is even more challenging.10 11
Increasingly there has been a move towards QI training sessions within teaching programmes; however, there can be a disconnect between an awareness of theoretical QI methodology and the real-life challenges of participating in QI while juggling a wide range of clinical activities required by trainees. The Faculty of Medical Leadership and Management found that 80.3% of trainees reported lack of time during the working week as a barrier to QI work.10 Additionally, absence of timely data to facilitate continuous improvement can be a further obstacle to successful QIPs.12
The concept of clinical microsystems as part of an integrated QI curriculum has been previously researched.13 A clinical microsystem is a small group of individuals, such as healthcare professionals, patients and their carers, who work together in a particular setting to deliver care for a defined population of patients.14 Microsystems were found to deliver a good impact on clinical and educational outcomes. A follow-on nursing focus group also suggested that improvement work facilitated good channels for communication with opportunities for collaboration. The authors proposed a move away from the individual ‘protected time’ concept for doing improvement work and channelling improvement in a more integrated, experiential, team-based approach.
Additionally, optimising improvement requires detailed methodology and significant engagement, and maximising this can be one of the hardest challenges for improvement champions.15 Conventional top-down healthcare has been shown to inhibit engagement; however, environments that encourage positive relationships within the multidisciplinary team (MDT) to align their goals can lead to increased engagement.16 17
Previous work has shown that the introduction of a multidisciplinary QI steering group and provision of QI training reinvigorated enthusiasm for QI in a busy emergency department and led to successes in a number of projects delivered by their multidisciplinary QI teams.18
Therefore, team InQuIRe was formed to provide a framework for sustainable QI within the respiratory department.
Measurement
Outcome measures
Total number of active respiratory QIPs.
Self-reported mean LifeQI change score of QIPs.
These were chosen to capture the overall outputs of the QI work in the department. All projects should be registered on LifeQI before data collection can begin, therefore this measure is a marker of the registered QI activity within the department. Change scores help show the self-reported progression of a project and define the stage of the project in a measurable numeric figure.
Process measures
Number of staff members in the respiratory QI faculty.
It is anticipated that by increasing the number of members within the faculty, especially from an MDT background, the output of QI work within our department will increase.
Balance measures
Number of QIPs with a change score ≤1.
A change score of ≤1 identifies a project to be within its initial planning stage, as shown in online supplemental appendix 1. If a project fails to progress, the score will not increase. Therefore, by measuring this we were able to determine if the QI faculty work was resulting in active and sustainable QI work, rather than simply leading to more QIP registrations.
Monthly data collection for all the above aspects was captured by members of the QI faculty and updated within our LifeQI project page.
Design
Four primary drivers were identified in order to meet our aims, and interventions were planned simultaneously across these domains. Figure 1 shows the driver diagram for the project.

Driver diagram. QIP, quality improvement project.
Description of primary drivers
QI understanding/training
Trust QI workshops were promoted for staff within the department. The local QI proposal form was shared for new starters in order to help frame new ideas. An introduction to QI and the current QI work within the department was incorporated into the departmental induction for new staff and delivered at each new rotation.
QI faculty communication
A QI display board was placed within the department to advertise the current QI work, QI team members and provide contact details for support. Physical folders were assembled to include QI proposal forms, fishbone diagrams and process maps for each project. Regular meetings were planned via Microsoft Teams until the faculty was fully established in order to maintain momentum, and minutes sent out to document progress and action points.
QI participation
In order to work towards our aims to create a long-term infrastructure for QI within the department, four SCF doctors and one respiratory SR were recruited to the team by two respiratory consultants with an interest in QI, one of which is the lead for quality and safety for respiratory. The SCFs are employed over a 12-month period and work across all respiratory wards on both acute sites. They provide continuity across junior doctor rotations and are embedded within clinical teams to promote QI. This was important in order to build sustainability into the faculty from the beginning.
The respiratory consultant body was approached for QIP ideas and asked to volunteer to sponsor and mentor projects. This list was then circulated within the department to encourage staff to approach the appropriate consultant to begin project work. All staff within the faculty registered for LifeQI access and were encouraged to attend trust QI training.
QIP completion
A respiratory QIP registry was created using Excel spreadsheet and was regularly reviewed at fortnightly meetings. Later, an action log was used to specifically allocate tasks to faculty members to ensure timely resolution of issues and encourage progression of projects. The LifeQI project change score was used, providing a useful snapshot numerical value to indicate the status of projects across our cross-site department, even when members were unable to attend meetings. LifeQI change scores could then be updated either during or after meetings to reflect the progress of a project towards completion.
Strategy
PDSA ramp 1: faculty meetings
1a. QI faculty meetings to discuss and progress current QIPs (15 September 2020)
Aims: (1) To mentor QI faculty members through current QI work to progress projects. (2) To review LifeQI data to ensure up to date.
Change hypothesis: Regular meetings will increase the number of QIPs and progression of QI work.
Strategy for change: Weekly meetings in person or via MS Teams with departmental QI leads. Reading lists of important QI methodology provided. Minutes to be kept to track progress and document required actions.
Outcome and learning: An increase in the number of QIPs registered and initially an increase in the mean scores of QIPs were observed; however, it was recognised that there was still scope to improve. The need to widen the QI faculty to include more members of the MDT quickly became clear in order to promote inclusivity of QI across disciplines and encourage collaborative working within the department. It was felt that this would help ensure projects were well rounded rather than doctor centric in their approach. Initially, an advanced clinical practitioner (ACP) was recruited, followed over time by two senior physiotherapists and three senior registered nurses. The addition of an ACP, physios and nurses as permanent members of staff within the respiratory department was anticipated to add to the continuity, support for MDT staff and increase the long-term sustainability of projects. Support from the clinical library service was incorporated with the aim of improving our evidence-based practice and assisting the team with the literature searches.
1b. QI faculty meetings moved to fortnightly (9 February 2021)
Aim: To allow time for more change to occur in QIPs between meetings.
Change hypothesis: Weekly meetings were felt to be too frequent and therefore a trial of fortnightly meetings was recommended. It was predicted that increasing the time between meetings would give staff more time to work on current projects, rather than reiterating the same action points week to week with little time to act on them.
Strategy for change: Fortnightly meetings in person or via MS Teams. Minutes continued to track progress and document required actions.
Outcome and learning: Fortnightly meetings were felt to be more successful by team members and allowed more time for staff to progress QIPs between meetings. Although not likely to be the sole reason, the mean score of QIPs was seen to increase after this, indicating the success of fortnightly meeting.
PDSA ramp 2: improving communication
2a. Development of a QI noticeboard (September 2020)
Aim: To effectively communicate with staff and convey key information relating to respiratory QIPs.
Change hypothesis: Signposting members of the respiratory department to key information relating to respiratory QIPs will advertise and promote QI work to all staff.
Strategy for change: Physical QI board designed and displayed on one inpatient ward area within the department. Pictures of faculty members, contact details and current QI work displayed.
Outcome and learning: Unfortunately, due to the ongoing coronavirus (COVID-19) pandemic, the physical board had to be removed due to infection prevention and control requirements. However, through PDSA 2b the faculty and its work was still promoted at each four monthly departmental induction.
2b. Promotion at departmental junior doctor induction every 4 months (9 December 2020)
Aim: To promote the respiratory QI faculty and encourage participation in QIPs throughout the department.
Change hypothesis: It was predicted that regular promotion will engage members of the department in QI within the department.
Strategy for change: Brief presentation written and delivered as part of the junior doctor departmental induction outlining the QI faculty team members; how to get involved; QI training and signposting to current QIPs within the department.
Outcome and learning: Over the 12 months, the number of QI programmes of work has increased which is likely to be due to ongoing promotion of the QI work within the department and accessible and approachable mentors. The faculty has provided a framework to ensure projects are appropriately supervised and new starters have the opportunity to join already established programmes of work. There was regular reinforcement of how to actively participate in QI during short training rotations.
2c. Registry of QIPs within the department (15 September 2020)
Aim: To keep a record of all QIPs within the respiratory department in a physical folder.
Change hypothesis: This will help us to keep a registry of all QI work within the department, document staff involved in projects and match with supervisors.
Strategy for change: QI registry to be created and located by QI information board. To contain a list of all projects, proposal forms for new starters and written support for QI methodology, for example, fishbone diagrams and process maps.
Outcome and learning: Although the folder was available, it was not felt to be used widely enough. This function would be better served online as all QIPs were registered on the LifeQI platform used by the trust, this was felt to be the best place to keep the register. This allowed regular reviews during faculty meetings, which were often held online on MS Teams, to identify projects which may have stalled and identify where further support is needed.
PDSA ramp 3: QI training
3a. Improving access to QI training (2 September 2020)
Aim: To increase the number of clinical staff who have received QI training.
Change hypothesis: Increasing access to QI training will lead to an increase in the number of staff trained in QI within the respiratory department.
Strategy for change: Staff within the department were directly encouraged to enrol in QI training by members of the multidisciplinary faculty. Two virtual QI workshops were initially organised due to COVID-19 restrictions on face-to-face teaching. Junior medical staff were informed and encouraged to join sessions and WhatsApp messages sent around on ward groups to promote the events.
Outcome and learning: This intervention led to a peak in the number of junior medical staff and ACPs trained in QI, enabling access to the LifeQI platform to progress their QI work. Feedback was collected to ensure the quality of the teaching delivered was equivalent to face-to-face sessions.
3b. Improving access to QI training during COVID-19 peaks (March 2021)
Aim: To continue to provide QI training while QI workshops are on hold due to the COVID-19 pandemic.
Change hypothesis: The progression of the COVID-19 pandemic led to the cancellation of the next QI workshop. Without intervention, this would have reduced QI participation as a LifeQI licence cannot be granted by the trust until QI training has been evidenced. A pre-recorded session was used to allow those keen to join QIPs to still access this training material.
Strategy for change: To overcome this challenge until face-to-face or virtual training could resume, a recorded video of a previous QI workshop was circulated. Staff could then watch this and sign a self-declaration of completion form for the hospital audit department to enable a LifeQI licence to be granted. An additional ad hoc session facilitated by members of the respiratory QI faculty was also run just for the department when trust-wide sessions were paused due to COVID-19 activity to provide the opportunity for interested team members to still progress with QI work.
Outcome and learning: Several members of staff watched the video and completed their self-declaration to enable them to get their LifeQI licence including junior doctors and ACPs. Twelve members of the respiratory department attended the virtual QI workshop although it should be noted that although this was a multidisciplinary group including ACPs, nurses and physiotherapists, no junior doctors attended this session. This may have been due to difficulties in arranging cover/staffing issues. However, it was not possible to sustain this intervention over the year as no equivalent trust-level training was taking place during this time. Only FY2 and IMT doctors received a ‘Fundamentals of QI’ training course at the beginning of their clinical year within the trust.
Much of the administrative work within the development of the QI faculty is not covered by clear PDSA cycles, however remains integral to the success of the faculty and has embedded the QI faculty into the department for the future.
Results
Outcome measures
Total number of active respiratory QIPs registered
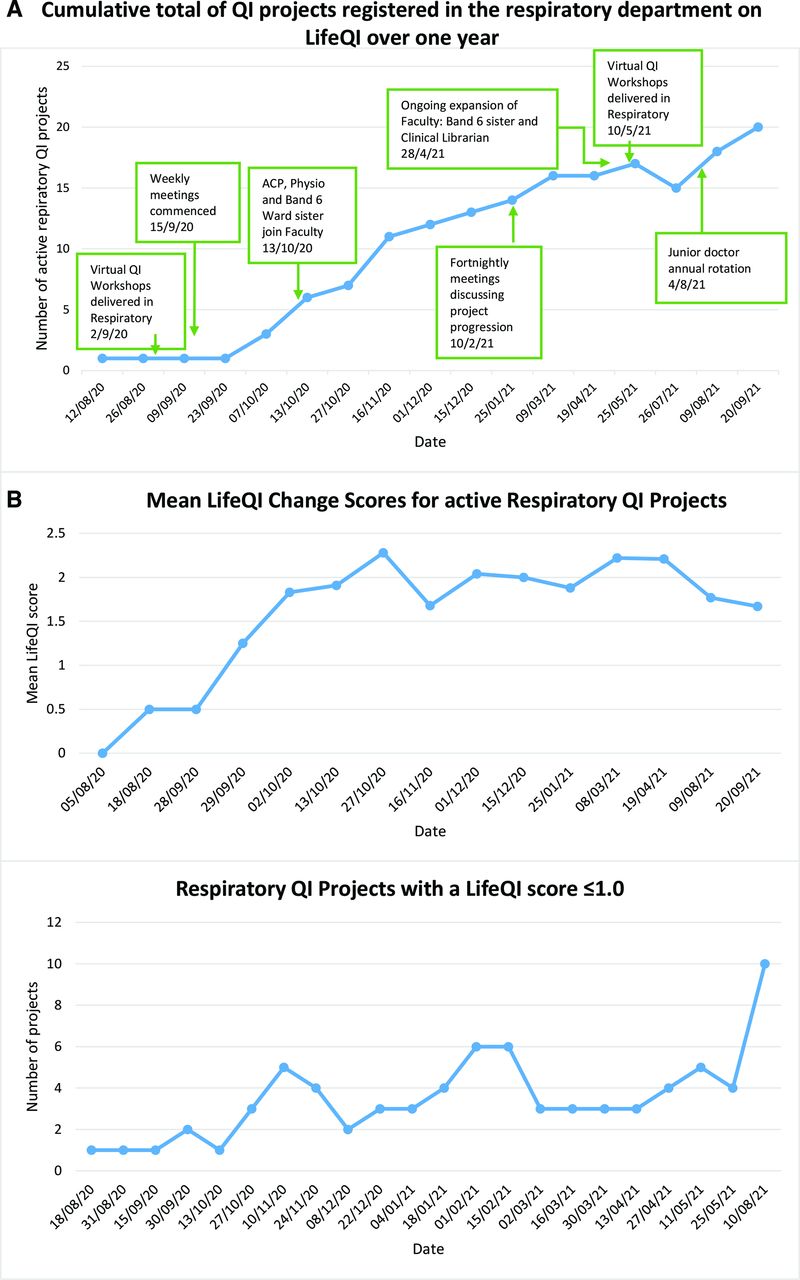
Over the course of the first year of the QI faculty 24 new QIPs were registered. Five projects were subsequently closed due to completion or lack of progression.
The largest change was seen in the autumn of 2020 as the faculty became established and the core multidisciplinary group was formed. This change was sustained through the rest of the year as shown by the progress chart in figure 2A.
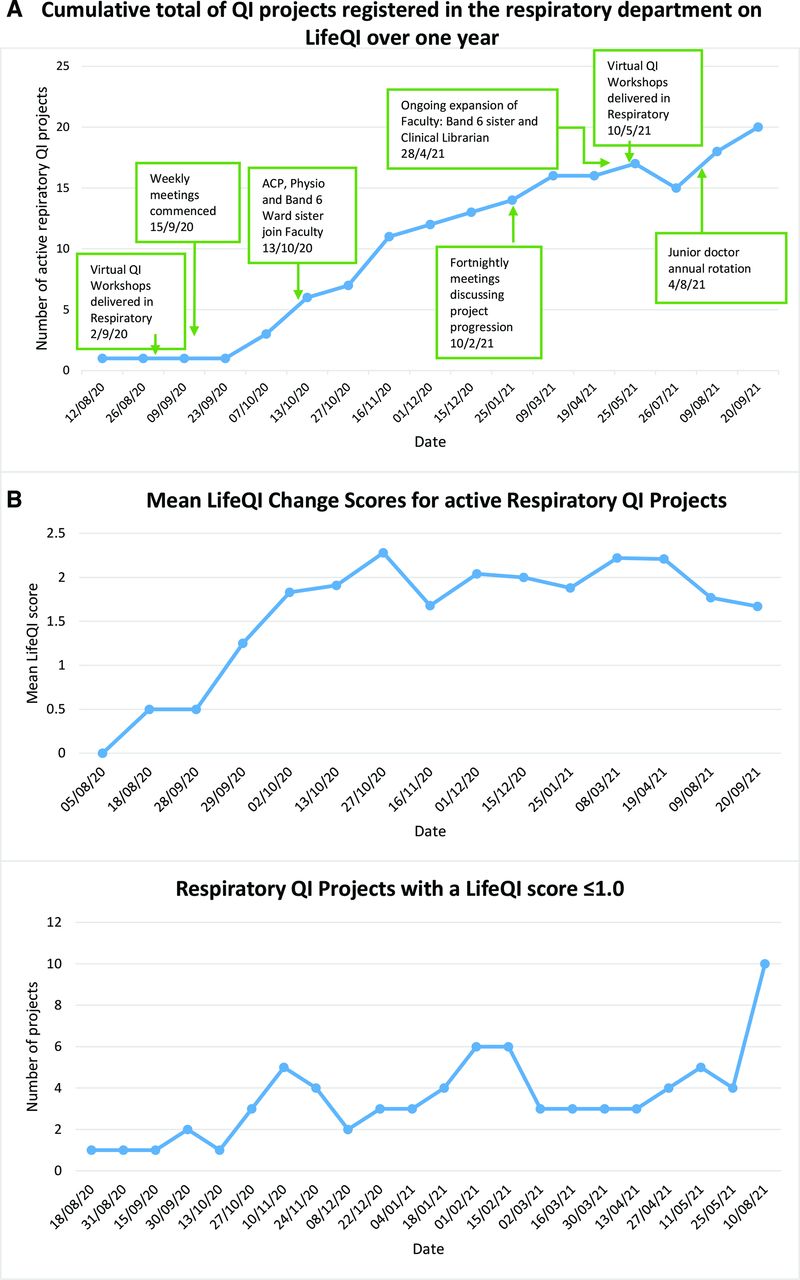
(A) Outcome measure 1: chart of active respiratory quality improvement projects (QIP) over time with interventions. (B) Outcome measure 2 and balance measure: mean LifeQI change scores and respiratory QIPs with a change score ≤1. ACP, advanced clinical practitioner.
Mean score of respiratory QIPs
The mean LifeQI change score improved from 0 in August 2020 to 1.67 in September 2021 as shown in figure 2B. This is a modest mean increase in score and reflects the variety of QI activity in the department.
There were a number of successful projects leading to embedded system changes; however, there were also a number of projects which struggled to progress for a variety of reasons, not limited to junior doctor/ACP rotations, the impact of COVID-19 and workforce pressures.
The most successful projects were noted to have QI faculty members as part of their teams.
Anecdotal discussions during faculty meetings indicated lots of active QI work, yet the change scores do not completely correspond to this. This may have occurred as additional time is needed to transfer data onto the online platform and update the change score. Additionally, as scores are self-reported and can only be updated by project members, these results may not have been accurate if project members did not update the LifeQI database in a timely fashion.
Process measure
Number of staff members in the respiratory QI faculty
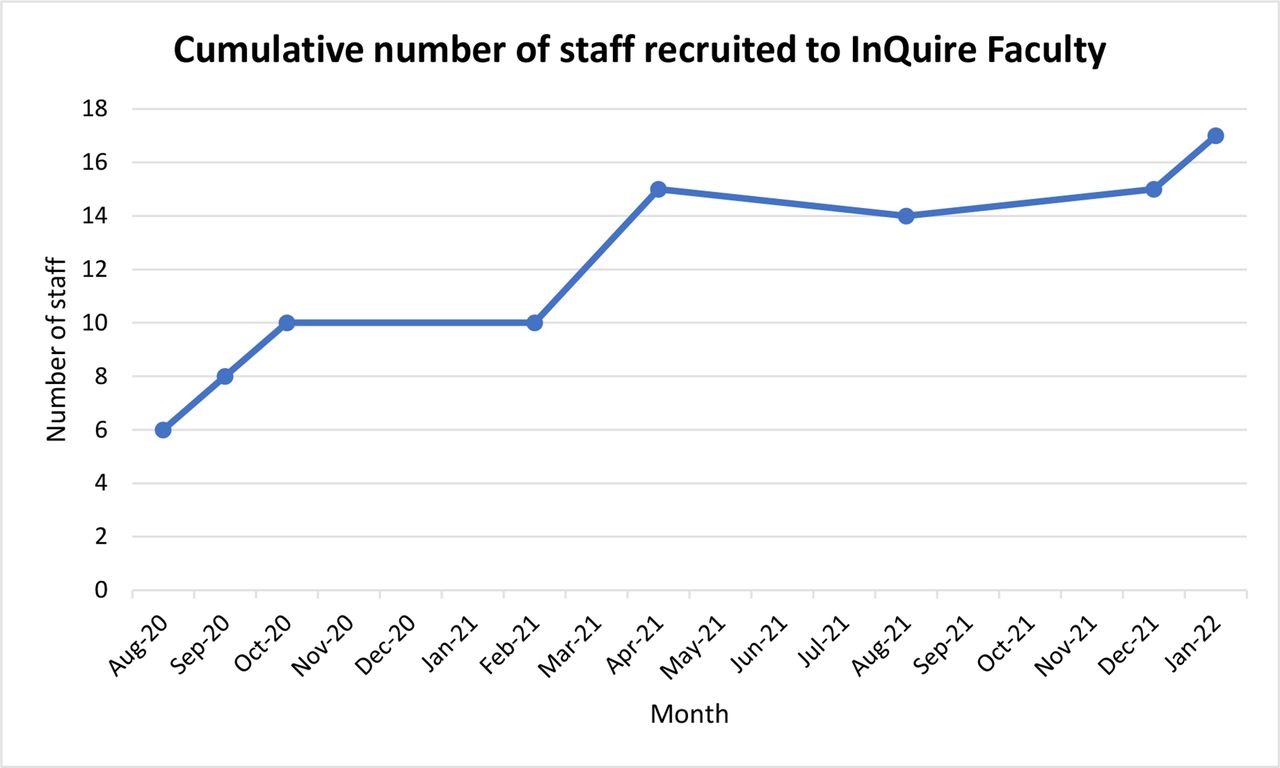
The faculty began as a team of six doctors in August 2020. It has steadily grown over the course of 18 months as shown in figure 3. It was quickly recognised that in order to improve access and involvement in QI across the department, representatives from all disciplines should be included in the faculty. Our MDT faculty increased inclusivity for staff interested in getting involved in QI and helped to create more rounded and considered projects which tackle key issues. One staff member subsequently stepped down from the faculty due to challenges with current clinical workload, two staff members rotated out of the trust but one position was replaced by their incoming counterpart. At the time of writing this article there are 16 faculty members: 7 doctors, 1 ACP, 2 nurses, 2 physiotherapists, 1 pharmacist, 2 clinical librarians and 1 trust improvement facilitator. Fifty-six per cent have been actively involved in at least one departmental QIP in the last year. Some staff members do not have individual projects but contribute logistical, managerial or library support to the existing departmental projects.

{kind=link}
{kind=link}
{kind=link}
Total number of respiratory staff in In-hospital Quality Improvement for Respiratory (InQuIRe).
All QI faculty members are required to regularly attend meetings and the faculty membership is regularly reviewed by the senior leadership.
Balance measure
Total number of respiratory QIPs with a LifeQI change score ≤1
The number of projects with a change score of ≤1 increased and decreased over time during the first year of the faculty, as shown in figure 2B. This reflects new projects registering on the platform before progressing through their QIP.
It is pleasing to see these are transient rises and confirms that new projects are actively progressing after registration (see online supplemental appendix 1 for change score descriptions). The peak at the final data entry is likely to represent the new project registrations at the start of the new training year.
Lessons and limitations
We found a need to reframe QI training for doctors. There is an expectation that trainee doctors should participate in QIPs as part of their continuous professional development.19 Foundation and internal medicine training curricula state the QI learning objectives and assessment requirements for the Annual Review of Competency Progression (ARCP) process.6 7 However, there may be limited constructive alignment as to how QI training is delivered, with individual healthcare organisations often being left to fill the opportunity and training void. Doctors may experience limited opportunities to participate in QI, leading to unwanted behaviours, such as treating QI as a ‘tick box’ exercise at ARCP, and having to ‘do’ a ‘QIP’ to progress to the next stage of training.
Our QI faculty has enabled a clear process for rotating medical staff to join existing projects aligned to departmental issues, rather than starting new, superficial or unsustainable projects. Oversight of all QI work across the department with fortnightly meetings and the use of QI methodology to measure the impact of this has certainly encouraged projects to progress and ensure sustainability. This is most marked in projects in which faculty members are directly involved.
It has been suggested that allocating a faculty mentor to every project would allow even further support for projects; however, it is important that staff are empowered to complete QI work independently for their own learning and development with mentoring support. Therefore, we have not yet incorporated this model; rather the faculty is available to support all projects within the department, and will liaise with project mentors as required.
Our initial primary driver was to improve training in QI; however, this project is limited by the lack of sufficient data available to show this improvement and therefore it is not presented as a process measure.
In August 2020, four junior doctors/ACPs had received training in QI. By the end of the rotation in November 2020 this had increased to 17 through the provision of targeted QI training for those team members. Subsequent to this, further data were not regularly collected. Due to the four monthly rotations of junior doctors and trainee ACPs, it was difficult to maintain an accurate run chart of the number of staff trained. Additionally, the impact of the COVID-19 pandemic significantly affected improvement training, as sessions were cancelled at short notice due to workforce pressures.
To try to tackle this, one of our other PDSAs was to move QI training online. The COVID-19 pandemic mandated a change to the delivery of educational sessions to prioritise the safety of teachers, learners and patients and adapt to new learning environments,20 with 53% of all new educational development initiatives since the COVID-19 pandemic being transferred to an online educational delivery system.21 We developed a virtual interactive workshop during the first wave and used a 5-point Likert scale to collect learner feedback. Comparing this to data already collected for our face-to-face workshops we demonstrated the immediate educational impact of a shorter interactive virtual workshop was similar. Likert scale score for understanding the ‘Principles of QI’ was 4.47 for virtual training compared with 4.43 for face to face (p=0.653).
The virtual workshop was also subsequently paused due to study leave cancellation. We tried to overcome this challenge by circulating a pre-recorded video of training; however, this is much less interactive than normal training workshops and may not leave learners with the same level of understanding as a result. Additionally, the delivery of ad hoc department-specific sessions is not a sustainable method of teaching as it is not part of faculty member job plans and can be challenging to fit in to busy clinical schedules. Trust-wide QI workshops have now restarted and we hope this will train more staff in the coming months.
The creation of the faculty and facilitation of regular meetings, mentoring and individual QIPs has required a significant amount of personal time investment by all faculty members. Attendance at regular faculty meetings has been challenging for all staff, especially during the COVID-19 pandemic, as the QI faculty is currently not protected time for clinical staff. A faculty should ideally be supported by dedicated administration support and time allocated for members to engage with this work in order to be sustainable in the future. More recently, we have introduced educational speaker sessions and are using action learning sets22 to provide peer support and progress current QIPs. Our faculty continues to expand and now includes a pharmacist and a member of the trust improvement team.
A number of large-scale successful multidisciplinary projects have been initiated and supported by the faculty which have led to significant improvements in patient care. One respiratory QIP on treating tobacco dependency in hospital has successfully progressed into a sustainable trust-wide roll-out.
We have presented our work at executive trust level and we have subsequently been contacted by a number of other departments interested in replicating a departmental QI faculty in their own areas. All faculty members have developed advanced skills in QI and a number of faculty members have progressed to become local or national improvement leaders. Individuals have also been supported to successfully present QI work at four regional or national conferences.
Intensive improvement data were only collected for projects during the first year as part of this QIP, therefore it is not possible to extend charts to present day. However, the faculty is now in its second year and continues to grow, with wider nursing representation, therapy, pharmacy and library support.
At the time of writing this article, we have demonstrated sustainable change with fully established fortnightly meetings where projects are reviewed, an established QI induction for new staff and a robust process for rotating staff to join existing QIPs within the department. We have achieved sustainability through embedding the faculty into the department with support from the senior leadership and multiple permanent members of staff from across the MDT.
Conclusion
The development of our multidisciplinary QI faculty enabled us to achieve our aim of increasing the number of registered QIPs with an increase in mean QI progression score. We have sustained the QI faculty during the COVID-19 pandemic and continue to increase the number of projects overseen by QI faculty with an expansion of faculty members.
Use of QI methodology to plan and evaluate delivery of QI has been a novel approach to a well-recognised issue within medical training at present. We have shown that a multidisciplinary QI faculty can lead to sustainable departmental QIPs, allowing rotating staff to join and build on existing projects with built-in senior support and oversight.
The development of a departmental QI faculty has been an extremely valuable model for improving access, organisation and project progression across a large department. We have helped to support the creation of similar specialty-based QI faculties within our hospital and this concept may be transferrable to other departments within a National Health Service organisation.
We anticipate the faculty will continue to grow and expand over the coming months, with an increasing focus on developing our multidisciplinary staff members, their QI knowledge and sharing our QI work across our organisation.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge all the staff that have supported and been involved with the improvement work within the respiratory department. The authors would like to acknowledge all current and former members of InQuIRe faculty for their hard work and commitment to developing the faculty. We acknowledge Lindsay Snell for her assistance with the literature review. Evidence Search: QI faculties (LS150). Lindsay Snell (2021). Derby, UK: University Hospitals of Derby & Burton NHS Foundation Trust Library and Knowledge Service.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AklakC
Contributors AC and JAH proposed the idea. All authors contributed to the implementation of the proposal and contributed to data collection and analysis. AC and JAH acted as mentors for the quality improvement programme. LAB and AC drafted the manuscript. All authors have reviewed and approved the final manuscript. AC is responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.