Article Text

Abstract
Alcohol use disorder is a constellation of symptoms and behaviours related to dependence and abuse. It is present in 11.0% of US adults and is a leading cause of death and healthcare expenditures in the USA. Medication-assisted treatment (MAT) is medication to reduce cravings, decrease rewards or limit withdrawal symptoms in combination with behavioural therapy.
A review of all patients with an alcohol-related condition admitted to internal medicine teams at an academic medical centre over a 7-month period (N=583) identified that only 1.4% (n=8) were discharged with an MAT prescription. Quality improvement methods were used to increase the proportion of patients discharged with an MAT prescription.
Implementing educational interventions and embedding a recommendation for MAT into the order sets used to treat alcohol withdrawal increased the percentage of patients with an alcohol-related condition that were discharged with an MAT prescription to 11.2%.
MAT remains an underused intervention for the treatment of alcohol use disorder. However, combining educational and structural interventions, including just-in-time teaching, can successfully increase the percentage of patients who receive an MAT prescription.
- quality improvement
- health equity
- cost-effectiveness
- medication safety
- graduate medical education
Data availability statement
Data are available on reasonable request. Raw data were generated at UC Davis Medical Center. Derived data supporting the findings of this study are available from the corresponding author LA on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Alcohol use disorder is an undertreated, common condition with significant healthcare and societal costs.
WHAT THIS STUDY ADDS
This quality improvement report demonstrates that medication assisted treatment’s (MAT) utilisation can be improved through embedded recommendations in alcohol withdrawal order sets to start MAT, brief educational interventions to relevant prescribers and adding MAT medications to the inpatient formulary.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These interventions could readily be adapted to other healthcare systems.
Problem
Alcohol use disorder is a common condition with significant healthcare and societal costs. Despite this, an evidence-based intervention to treat alcohol use disorder known as medication-assisted treatment (MAT) remains heavily underused. MAT is medication to reduce cravings, decrease rewards or limit withdrawal symptoms in combination with behavioural therapy.
Our institution is a large tertiary medical centre serving as the only academic medical centre in the region. Approximately 83 patients with alcohol-related conditions are admitted monthly to internal medicine teams staffed by the hospitalist division or the internal medicine residency programme. A review of these patients from June to December 2019 identified that only 1.4% (N=583) were discharged with an MAT prescription. We sought to increase the utilisation of MAT at discharge for patients admitted with any alcohol-related condition to 11.0% within 18 months. We chose this goal because in 2019 MAT was prescribed to 11.3% of US people who received any alcohol use treatment.1 Due to unforeseen delays from the COVID-19 pandemic, the project time frame was extended to 26 months.
Background
Alcohol use disorder, a constellation of behaviours and symptoms related to dependence and abuse, was present in 11.0% of US adults in 2020.2 Excessive alcohol use is a leading cause of death and healthcare expenditures in the USA, accounting for 1 in 10 deaths3 and an average of 29 years of life lost per death.4 Economically, alcohol use is estimated to cost around US$249 billion annually in lost productivity, healthcare expenditures and social costs.5
MAT is an approach to substance use disorders that combines medication with behavioural interventions. Currently, there are three United States Food and Drug Administration (FDA)-approved medications for the treatment of alcohol use disorder: naltrexone (available oral and as long-acting injectable), acamprosate and disulfiram. Naltrexone is an opiate antagonist that is well tolerated, with reported effects of reduced cravings, reduced relapse rates and an overall decrease in alcohol use. It is estimated to reduce the risk of return to heavy drinking by 17% and trended towards abstinence.6 Acamprosate’s mechanism is still unknown but it has been shown to significantly reduce the risk of any drinking by 14% and maintain abstinence drinking.7
MAT remains underused nationally as only 1.1% of adults with alcohol use disorder reported receiving MAT in 2020.2 While many patients may refuse medication, a survey of outpatient providers noted lack of comfort and knowledge as the most common reasons for avoiding pharmacotherapy.8 An educational intervention combined with a new discharge protocol at a tertiary medical centre showed a significant increase in naltrexone prescriptions and reduced all-cause emergency department visits and inpatient readmissions.9
Measurement
Our primary outcome measure was the proportion of patients admitted to an internal medicine service with any International Classification of Diseases, 10th Revision (ICD-10) alcohol-related condition that received either a naltrexone or acamprosate prescription at discharge, excluding patients prescribed naltrexone in an inappropriate or unsafe manner (concurrent opiate at discharge, Aspartate aminotransferase (AST) or Alanine aminotransferase (ALT) >3 times the upper limit of normal). For our secondary outcome, we measured the rate of emergency room revisit and inpatient readmissions. Data were gathered monthly using the electronic medical record. Baseline data gathering for our project started in June 2019 (hereinafter referred to as month 1). The primary and secondary outcomes were measured monthly and are reported in three distinct time periods: as a baseline (months 1–7), after the first intervention of PDSA cycle 1 (months 8–18) and after the first intervention of our second PDSA cycle (months 19–26). We also tracked how many patients were treated for alcohol withdrawal.
Design
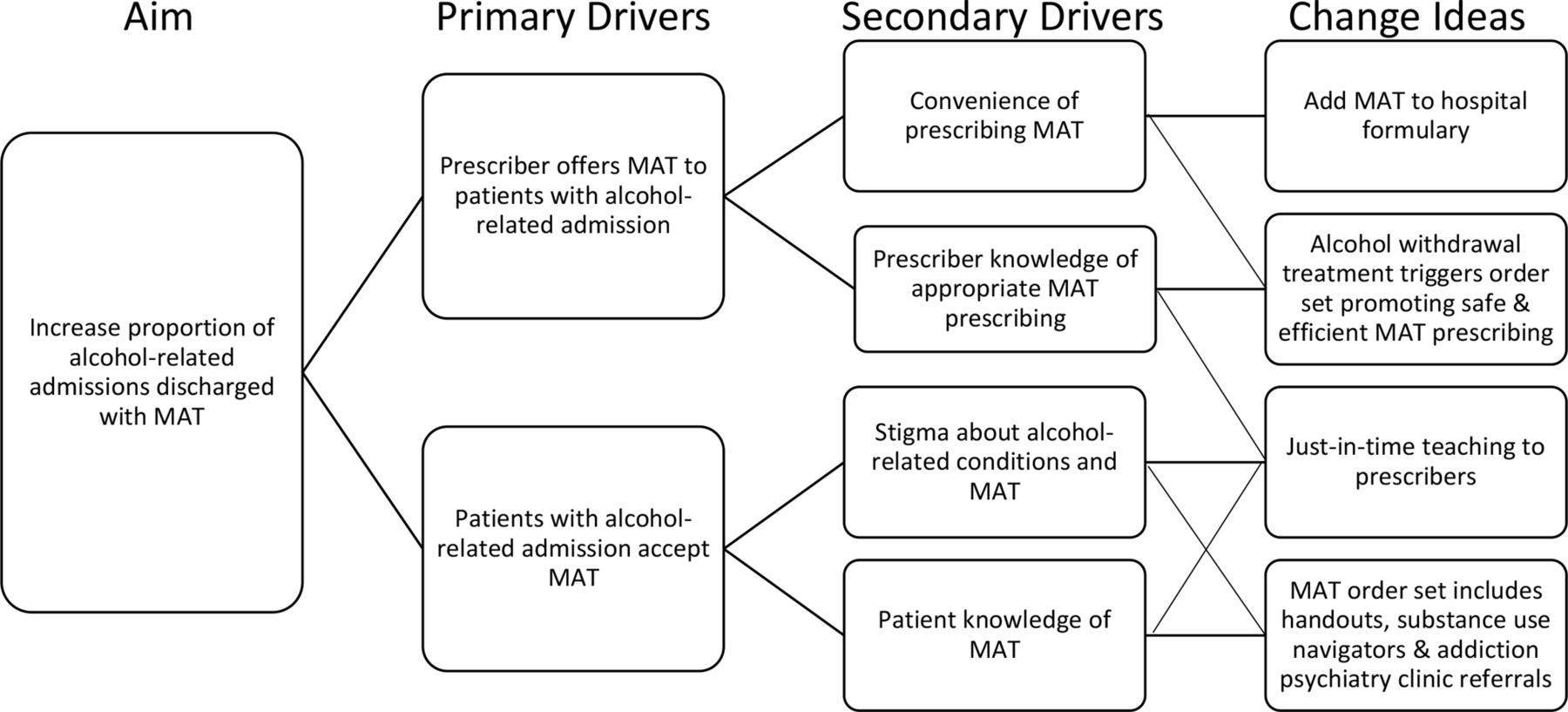
We assembled a multidisciplinary team including representatives from internal medicine, psychiatry, emergency medicine and pharmacy. See figure 1 for our team’s driver diagram. Given the low prescribing rate in the months preceding our intervention and the absence of naltrexone or acamprosate from the inpatient formulary, we anticipated significant obstacles to identifying patients with alcohol use disorder and adopting MAT. With sustainability in mind, we sought to combine structural (adding MAT medications to the formulary, using triggered order sets) and educational interventions to create a cultural shift in the treatment of alcohol use disorder at our institution. Our initial PDSA cycle focused on the existing discharge order set to include naltrexone, acamprosate or disulfiram prescriptions with handouts to local resources (see online supplemental materials). To target those patients who were expected to have a moderate to severe alcohol use disorder, we programmed a modification to the discharge order set that only triggered if a physician had ordered an alcohol withdrawal order set during that admission. Our second PDSA cycle focused on interventions throughout the hospital course. It incorporated modifications to the alcohol withdrawal order sets themselves to include a prefilled order to begin in the hospital for naltrexone or acamprosate with guidance on its use. We also included a preselected consult order for a new substance use navigator service that coincidentally started at our hospital around that time. This is a consult service of healthcare navigators with backgrounds in social work or psychotherapy specialising in substance use disorder assessments, health education and the referral process for local residential and outpatient substance use treatment programmes. We focused on naltrexone and acamprosate due to their outcomes in reducing drinking or maintaining abstinence, tolerability and inclusion in a 2018 practice guideline from the American Psychiatric Association recommending their use in moderate or severe alcohol use disorder.10 Due to its daily dosing rather than three times daily, we recommended naltrexone. We later chose not to encourage disulfiram due to its frequent use in supervised settings and the need for patients to be free from intoxication to avoid adverse effects. This quality improvement project did not involve patients or the public in design, conduct, reporting or dissemination.
Supplemental material
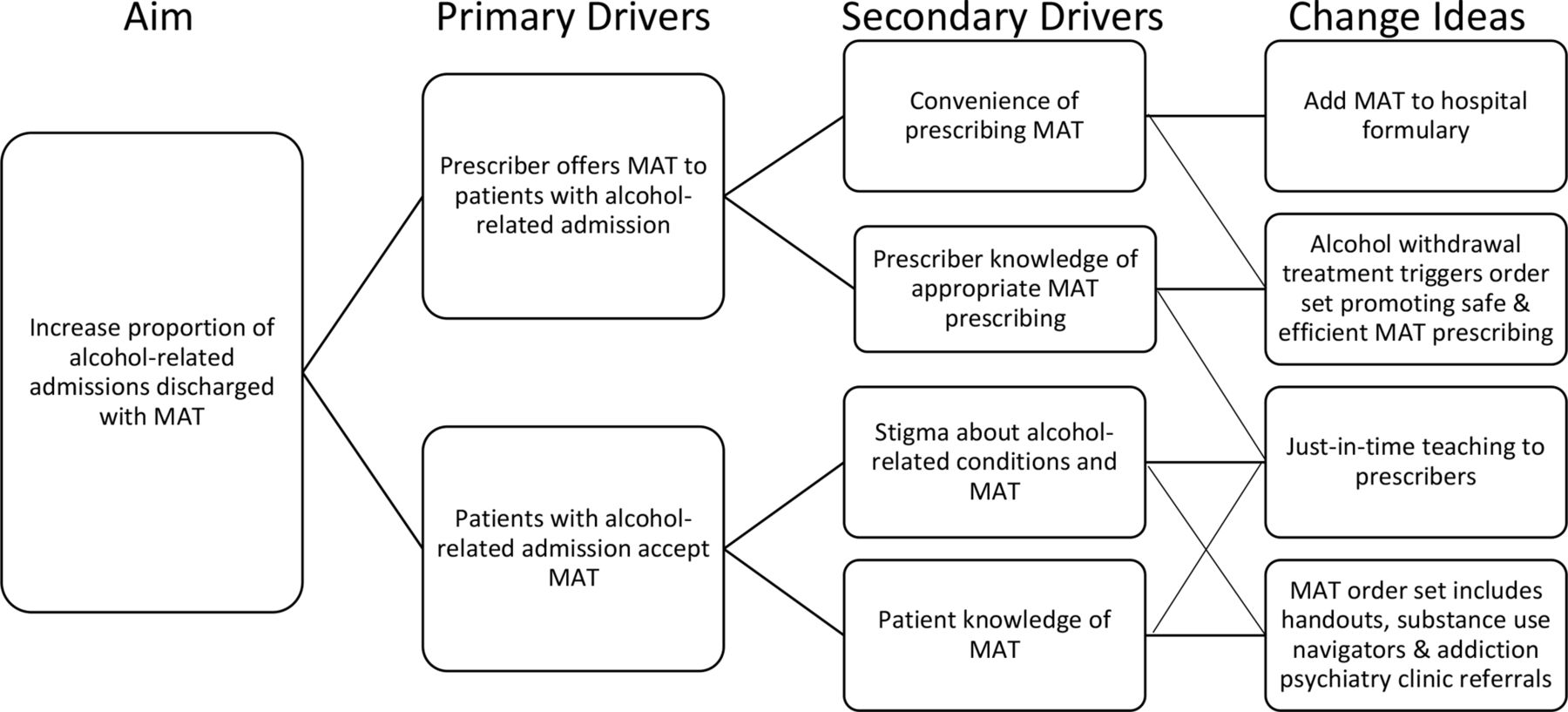
Increasing utilisation of MAT driver diagram. MAT, medication-assisted treatment.
Strategy
Our project aimed to increase the utilisation of MAT for patients admitted for any alcohol-related condition with a moderate to severe alcohol use disorder. Some unexpected hurdles included the lack of any MAT option on the formulary and the COVID-19 pandemic, which delayed and deprioritised our interventions.
PDSA cycle 1: Our initial PDSA cycle incorporated three main interventions: addition of naltrexone and later acamprosate to the inpatient formulary, a brief talk to the hospitalist division and modification to the discharge order set, which is used for all discharges at our hospital. Before any interventions were instituted, we applied for naltrexone’s inclusion in the inpatient formulary, which was granted during month 7. Modifications to the discharge order set also occurred in month 7. The brief talk, which included background information on alcohol use disorder, diagnosis and treatment occurred in month 8. In the months after our interventions, we saw a rapid increase in the proportion of patients prescribed MAT, followed by a modest and sustained increase. Informal feedback from prescribers was obtained but not quantitatively measured by a survey. This feedback noted a lack of convenience and comfort with starting a new medication only at discharge after plans had been finalised.
PDSA cycle 2: Due to the feedback we received during PDSA cycle 1, we altered the alcohol withdrawal order set to facilitate earlier physician–patient discussions about the potential benefits of MAT and encourage initiation of MAT treatment in the hospital rather than only at discharge. In month 18, the alcohol withdrawal order sets were altered to recommend either naltrexone or acamprosate with just-in-time teaching on when either therapy would be most appropriate. This intervention was intended to improve prescriber knowledge of MAT and make prescribing more convenient. The order set also included a referral to the new substance use navigator service. A brief talk was again given to the hospitalist division in month 20, and the project was introduced to the internal medicine residency programme in month 22. We again tracked our primary outcome measure and saw a rapid and sustained increase in the proportion of patients receiving MAT after our interventions.
Results
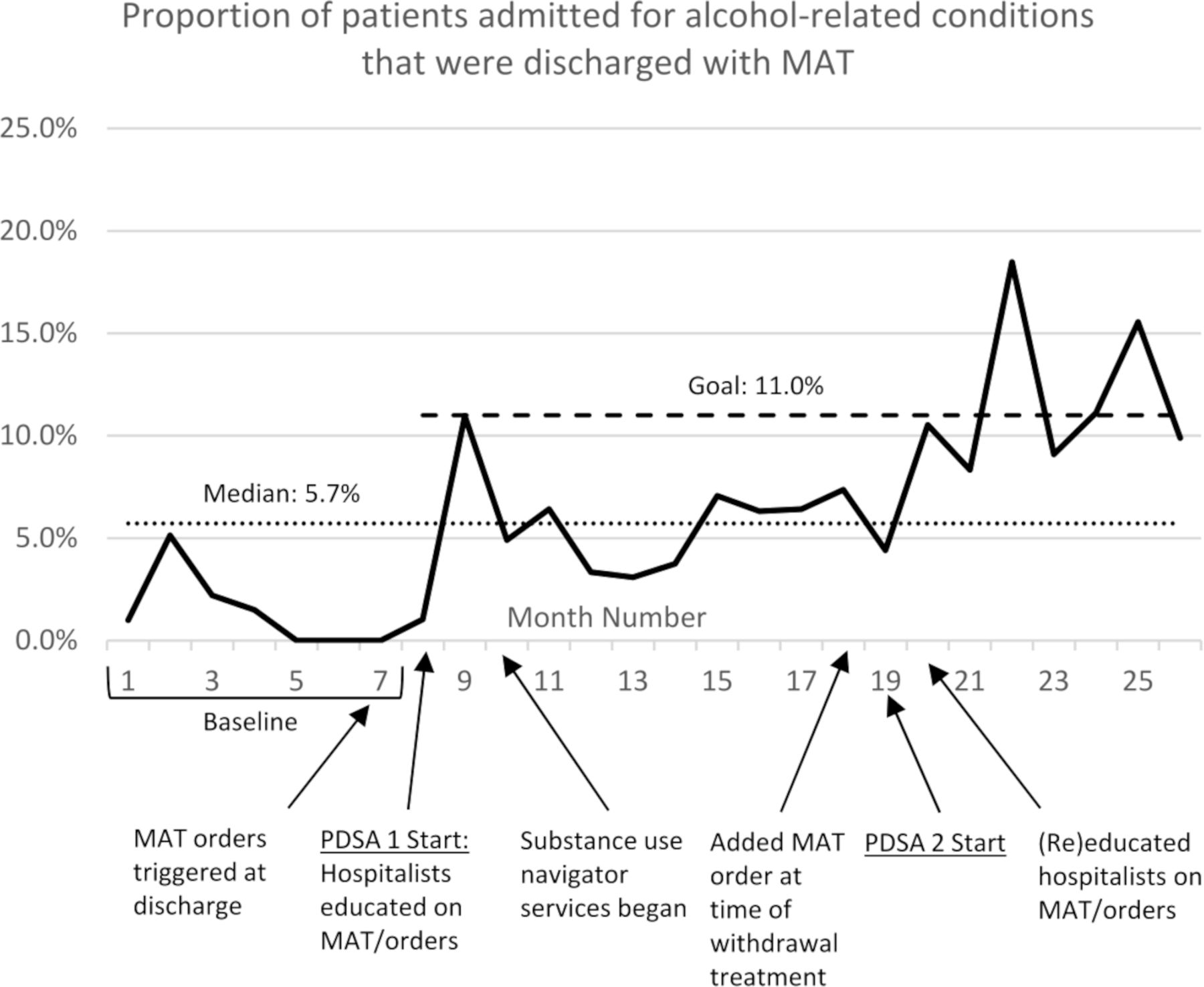
Our primary outcome measure was the proportion of patients treated for any ICD-10 alcohol-related condition that received one of two MAT prescriptions at discharge. At baseline, 1.4% (N=583) of patients admitted for alcohol related conditions were prescribed MAT (see figure 2). After PDSA cycle 1 began (months 8–18), this proportion increased to 5.4% (N=970) despite minimal education outreach during the COVID-19 pandemic. After PDSA cycle 2 began (months 19–26), the proportion of patients receiving MAT increased to 11.2% (N=686). Of those treated for withdrawal during this period, 18.3% (N=421) were discharged with an MAT prescription. The inpatient and emergency room readmission rates did not significantly change during any of the time periods.
{kind=link}
{kind=link}
Run chart showing the proportion of patients admitted for an alcohol-related condition who were prescribed MAT at discharge, by month. MAT, medication-assisted treatment. PDSA, Plan-Do-Study-Act Cycle.
The proportion of all naltrexone prescriptions that were potentially inappropriate or unsafe was 50.00% (N=12) at baseline, 5.7% (N=35) after PDSA cycle 1 and 14.3% after PDSA cycle 2 (N=63).
Lessons and limitations
Our project aimed to improve the utilisation of an effective treatment for alcohol use disorder to reduce unhealthy drinking and decrease the healthcare and societal costs of excessive alcohol use. We anticipated significant barriers to using MAT for alcohol use disorder, given low rates of use nationally. However, a key lesson from our project was the success in combining structural changes and education interventions. Adding MAT medications to the formulary and automatically recommending MAT through the EMR during the hospitalisation improved the convenience of prescribing MAT. Just-in-time teaching, handouts and brief talks to relevant prescribers helped reduce stigma and improve prescriber and patient knowledge of MAT.
During PDSA cycle 1, we received feedback that discharge was an inconvenient time to discuss and initiate a new medication. This could have been reflected in the rapid increase in our primary outcome measure after the educational interventions, followed by a more modest increase as time progressed. During PDSA cycle 2, we sought to create an opportunity to discuss and initiate MAT earlier in the hospital course, including at admission when the suspicion for alcohol withdrawal is often the highest. These further interventions led to a rapid increase in prescribing to meet our project goal.
While we achieved our goals, there still may be opportunity to increase MAT usage among our patient population. Nearly all patients treated for withdrawal also received a consult from the substance use navigator service, indicating at least some openness to decreasing their use. While the navigators are not prescribers, including familiarity with and regular suggestion to discuss MAT with their prescriber in their practice may lead further patients to initiate MAT. As previously discussed, only 11.3% of US people in 2019 who received any treatment for alcohol use disorder were prescribed MAT. In our study, a sizeable proportion of patients who sought treatment may have preferred psychotherapy or peer support groups without medication due to safety concerns or other considerations. We were unable to track referrals to therapy or peer support for this intervention but doing so is an opportunity for future study. In addition, while the patients that we targeted who were treated for alcohol withdrawal meet at least some of the criteria for alcohol use disorder, we may have missed a sizeable portion of patients with moderate to severe alcohol use disorder who are not treated for withdrawal. Besides our education interventions to prescribers, our project did not directly target these patients. Our project did not see an effect on readmission rates, yet as the use of MAT increases, we hope to understand better which patients are more likely to receive MAT and why they are readmitted.
The sporadic timing of our interventions limited our study, and our data were gathered monthly, so it was challenging to discern the direct associations. The overall number of patients treated with MAT was also low, leading to our results' variability. Furthermore, our healthcare system treats patients from many different insurances, primary care networks and geographical regions, which hampered our ability to collect long-term follow-up data, such as fill history and adherence at follow-up.
Finally, we would like to discuss project transferability to other health systems and sustainability. The MAT order set (available as online supplemental file 1), which we set to be automatically triggered by alcohol withdrawal orders, could readily be adapted to other electronic medical records and required minimal effort on behalf of the project members. The brief prescriber education on alcohol use disorder and MAT was done live with minimal graphics. To make the education piece more sustainable or transferable, future efforts could develop a brief online module, perhaps as part of periodic hospital training.
Conclusion
This project used educational outreach and multiple structural interventions to spread awareness and identify patients who may be candidates for MAT in real time. These interventions increased the utilisation of MAT for alcohol use disorder, gains which we expect will sustain as familiarity with naltrexone or acamprosate increases. We believe these changes can be implemented at any institution that uses an order set to treat alcohol withdrawal.
Data availability statement
Data are available on reasonable request. Raw data were generated at UC Davis Medical Center. Derived data supporting the findings of this study are available from the corresponding author LA on request.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Connor Reilly, Eddie Eabisa and Hao Zhang (UC Davis Health Department of Quality and Safety) for support with data gathering and project management; we thank Dr. Joshua Elder and Dr. Daniel Colby (UC Davis Health Department of Emergency Medicine) for input on project design; we thank Kathie Le, Julia Munsch and Rebecca Hoss (UC Davis Health Pharmacy Department) for assistance adding naltrexone to the hospital formulary; we thank the UC Davis Health Internal Medicine Residency Program for dedicating training time to quality improvement. This work was supported by the 2019-2020 UC Davis Medical Center GME High Value Competition Award from the UC Davis Health Department of Quality and Safety.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LA led the design of the project, coordinated implementation, performed outreach to prescribers, gathered and analysed data, and drafted and revised the manuscript. He is the guarantor. HJ assisted with project design, facilitated implementation of the electronic medical record order set changes and revised the paper. JD assisted with project design, troubleshooting, manuscript writing and revisions.
Funding UC Davis Health Department of Quality and Safety 2019-2020 GME High Value Competition Award US$7000 (no award or grant number).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.