Article Text

Abstract
Introduction Women from ethnic minority groups are at more risk of adverse outcomes in pregnancy compared with those from white British groups; suboptimal care may contribute to this increased risk. This study aimed to examine serious clinical incidents at two maternity units to explore causative factors for women from ethnic minorities and determine whether these differed from white women.
Methods A retrospective review was conducted of all serious incidents (n=36) occurring in a large National Health Service maternity provider (~14 000 births per annum) between 2018 and 2020. Data were collected from case records for variables which could mediate the association between ethnicity and adverse outcome. The incident reviews were blinded and reviewed by two independent investigators and data regarding root causes and contributory factors were extracted.
Results Fourteen of the 36 incidents (39%) occurred in women from minority ethnic groups, which is comparable to the maternity population. Women involved in serious clinical incidents frequently had pre-existing medical or obstetric complications. Booking after 12 weeks’ gestation occurred more frequently in women from minority ethnic groups than in the background population. There were differences in root causes of serious incidents between groups, a lack of situational awareness was the most frequent cause in white women and staff workload was most frequent in women from minority ethnic groups. Communication issues and detection of deterioration were similar between the two groups.
Discussion Although there was no difference in the proportion of serious incidents between the groups, there were differences in medical and pregnancy-related risk factors between groups and in the root causes identified. Efforts are needed to ensure equity of early access to antenatal care and to ensure that there is adequate staffing to ensure that women’s needs are met; this is particularly cogent when there are complex medical or social needs.
- obstetrics and gynecology
- adverse events, epidemiology and detection
- birth injuries
- clinical governance
- incident reporting
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- obstetrics and gynecology
- adverse events, epidemiology and detection
- birth injuries
- clinical governance
- incident reporting
What is already known on this topic
Women from black and minority ethnic groups have higher rates of maternal and perinatal morbidity and mortality.
In the whole maternity population, suboptimal care is implicated in a significant proportion of cases ending in maternal or perinatal death.
What this study adds
Women from minority ethnic groups who had a serious incident review more frequently booked later than white women.
This review of serious incidents found that underlying ‘root’ causes differed between women from white ethnic groups and those from non-white ethnic groups.
How this study might affect research, practice or policy
Larger studies are needed to understand underlying and contributory causes to serious incidents in maternity care involving women from minority ethnic groups.
Maternity care needs to address inequity in access to antenatal care.
Introduction
Between 2014 and 2018, 26% of births in the UK were to women from ethnic minority (black, Asian or other ethnic minority) groups.1 Population-level evidence indicates that women from ethnic minority groups are at more risk from adverse outcomes in pregnancy.2 3 The latest Confidential Enquiry into Maternal Deaths highlighted that the rates of maternal mortality are four times greater in women of black ethnic backgrounds and two times greater for women of Asian ethnic backgrounds when compared with white women.4 Women from ethnic minority groups are more likely to have severe maternal morbidity in their pregnancies5 6 and their ethnicity is a risk factor for progression of morbidity to mortality.7 When matched for the same illnesses, women from ethnic minorities, specifically those who were black African or black Caribbean, had a higher risk of progressing to death when compared with white women.7 Stillbirths and neonatal mortality also remain disproportionately high for babies born to ethnic minority women8 and perinatal mortality, preterm birth and low birth weight are also disproportionately higher for babies born to mothers from ethnic minorities and to mothers living in the most deprived quintile, based on the mother’s postcode at delivery.8 9
Evidence investigating risk factors associated with maternal deaths from direct and indirect causes identified seven independent variables that were associated with increased odds of maternal death: pre-existing medical disorders, anaemia during the current pregnancy, inadequate use of antenatal care, previous pregnancy problems, substance misuse, unemployment and increasing maternal age.10 However, investigating factors associated with maternal death from direct pregnancy complications found that there were some differences between ethnic groups.11 More recent work has investigated ethnic disparities in maternal mortality and found no major differences in causes of death between women from different aggregated ethnic groups.12 However, multiple areas of bias were identified in the care women received including lack of nuanced care, microaggressions and clinical, social and cultural complexity.12 For stillbirths, data are conflicting; some analyses that adjusted for known risk factors, found a higher rate for ethnic minority women13 14 whereas other studies did not,15 suggesting that the disparity in outcomes may not be fully explained by other socioeconomic characteristics.
As the determinants of health inequalities in women from ethnic minority groups are multifactorial and not fully known,16 it is plausible that suboptimal care may contribute to the increased risk of adverse outcomes.9 In a large study of women who gave birth in the UK, women from ethnic minorities tended to access antenatal care later in pregnancy, have fewer antenatal checks, fewer ultrasound scans and less screening.17 Women from ethnic minority groups may experience barriers which make accessing antenatal care more difficult including: language barriers, lack of familiarity with the healthcare system, racism, discrimination and lack of trust in services.7 9 18 19 Many of these barriers may be further increased if women are not familiar with the UK health system.
While maternal deaths and selected perinatal deaths are reviewed at a national level in Confidential Enquiries, clinical incidents are used at a local level to review maternity cases that may have resulted in harm. As maternal deaths are rare, review of other adverse events can provide insight into how care is managed and uncover lessons to be learnt.20 Through the Serious Incident Framework, root and contributory causes are examined which can help identify fundamental issues, ensuring greater understanding of an event.21 The authors have not been able to identify any studies which examine obstetric clinical incidents and review the factors involved for ethnic minority women. This study aimed to examine high-level obstetric incidents at a large UK NHS Trust providing care for an ethnically and socially diverse population and to explore the causative factors for ethnic minority women, and whether these differ from women who are not from an ethnic minority background.
Methods
A retrospective review of serious incidents (SI) reported in a large UK NHS Trust (providing care within two maternity unit sites) was conducted. Together, the maternity units are responsible for approximately 14 000 births per year providing tertiary-level antenatal, intrapartum and neonatal services. The urban city is one of the most ethnically diverse cities in the UK with 33.3% of the population identifying as from an ethnic minority background.22 This study compared women of white British and white European backgrounds with women from ethnic minority backgrounds.
Clinical incidents are divided into five levels: 1 (no harm), 2 (low), 3 (moderate), 4 (major) and 5 (death/catastrophic) under the Serious Incident Framework.23 All level 3, 4 and 5 incidents which had an SI investigation under the NHS Serious Incident Framework occurring between April 2018 and April 2020 were included. Incidents involving information governance, temporary maternity unit closures to admissions and mislabelled blood specimens were excluded.
Variables which may mediate the association between adverse outcomes and ethnicity were identified from relevant publications2 10 and are listed in the supplementary file 1. Demographic data were obtained from maternity notes. Information on deprivation indices were provided from the postcode deprivation index tool published by the Ministry of Housing, Communities and Local Government.24
Supplemental material
The methodology for evaluation of individual reviews followed the template used previously to evaluate the impact of consultant presence.25 Each SI investigation report was anonymised by SR. An independent retrospective review of the SI investigation reports was undertaken by two members of the team (DF, KF). Data regarding the root causes and contributory causes reported by the investigation were collated. A root cause was defined as a fundamental issue that underpinned the SI (ie, why the SI occurred) and contributory factors were defined as issues that led to the SI problem (ie, how the SI occurred), a list of contributory factors is included in online supplemental file 2. Further demographic and clinical data were collated from the maternity information system and health records and then once collected, matched to the anonymised SI report. The team included midwives (KF, KW), obstetricians (DF, SV, AH) and members of the risk management team (HB, SR). All have worked in the maternity unit being studied and have experience in providing maternity care for the population for between 1 and 20 years. One investigator was from a black British background and the others were white British/other.
Supplemental material
Patient and public involvement
As this was an analysis of serious clinical incidents, it was not felt to be appropriate to involve patients and the participants in the conduct of this study.
Results
Between April 2018 and April 2020, there were a total of 36 serious incidents (level 3 or above) which met the inclusion criteria. In total, there were 7 level 5, 5 level 4 and 24 level 3 cases reviewed.
Fourteen incidents (39%) involved women from ethnic minority groups. In the same period, there were a total of 23 350 births at the Trust, and 8455 (36.2%) were to women from ethnic minority groups.
Table 1 shows the ethnicity breakdown of births and women involved in high-level obstetric incidents.
Breakdown of women involved in high-level obstetric incidents by mother’s ethnicity compared with the distribution of births at the maternity service
Most (18/36, 50%) of the cases occurred in women of white British ethnic origin and this group are slightly under-represented in incidents when compared with the background birth rate of the trust (56%). Conversely, there was a trend towards a higher frequency of Pakistani, Bangladeshi, black African and black Caribbean women involved in the clinical incidents when compared with the background birth rate. Table 2 summarises the characteristics of the women who were involved in the incidents and compares women from ethnic minority backgrounds with white British/European women.
Characteristics of women involved in clinical incidents
For pregnancy-related factors, there was a greater proportion of women involved in incidents who had pre-existing medical problems (61%, 22/36) and obstetric problems in the current pregnancy (64%, 23/36%). When broken down by ethnicity, findings suggest risk factors occur more frequently in white women than women of ethnic minorities: 68% (15/22) vs 50% (7/14) for pre-existing medical problems and 73% (16/22) compared with 50% (7/14) for obstetric problems in the current pregnancy. However, none of these differences were statistically significant. All women in the sample were registered with a GP. Overall, inadequate use of antenatal services (defined as concealed pregnancy, booking after 12 weeks, or not receiving recommended minimal levels of antenatal care) occurred in 19% (7/36) of pregnancies compared with 18% of pregnancies overall in the maternity units. All of these were due to booking after 12 weeks which occurred more frequently in ethnic minority women (36%, 5/14) compared with in white women (9%, 2/22; p<0.001); the proportion of women from minority ethnic groups booking later in our group was also higher than the overall proportion for ethnic minority women booking late within the maternity units (32%). Women from ethnic minority backgrounds were significantly less likely to smoke cigarettes (p<0.001) and were younger than white women (p=0.006). A high proportion of women (47%, 17/36) involved in incidents were from the poorest two deciles in the UK. A greater proportion of these women were from ethnic minority groups (57%, 8/14 vs 41%, 9/22) and more women from ethnic minority groups were unemployed (43%, 6/14 vs 14%, 3/22). Many ethnic minority women involved in incidents were not born in the UK (57%, 8/14).
Table 3 summarises the breakdown of levels of severity and harm by ethnicity.
Total number of incidents in ethnic minority women compared with white women organised by level of severity and harm
There was no statistically significant difference in the proportion of women from ethnic minority backgrounds involved in the highest severity category (level 5) when compared with white women (21%, 3/14 vs 18%, 4/22; p=0.12). The most common category of clinical incident was an unexpected transfer of a term baby to the neonatal intensive care unit with 11 cases. There was one case of maternal death, one neonatal death and four cases of stillbirth. A full list of clinical incident categories can be found in figure 1.
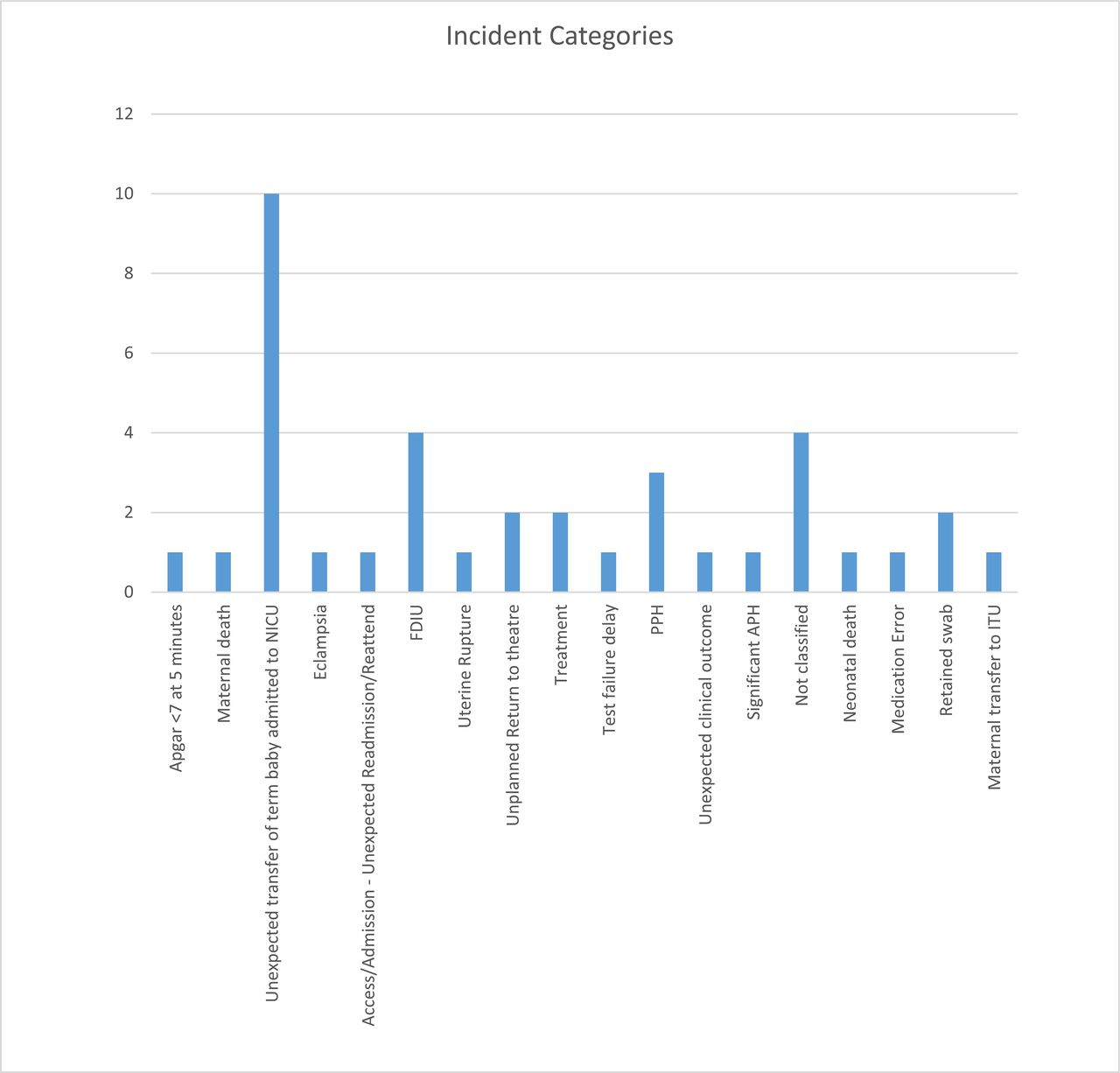
Categories of serious incidents reviewed in this study. APH, Antepartum haemorrhage; FDIU, fetal death in utero; ITU, intensive therapy unit; PPH, postpartum haemorrhage; NICU, neonatal intensive care unit.
Figure 2 demonstrates the multifactorial nature of the root causes listed in cases involving women from ethnic minority groups compared with those from white ethnic groups. For three of the cases, care was deemed appropriate, and no root cause could be found (eg, placental abruption occurred prior to admission), but many cases involved more than one root cause. Throughout all clinical incidents the most common factors identified as root causes for these incidents were: decision-making (n=15, 21.7% of root causes), lack of situational awareness (n=12, 17.4%) staff workload (n=10, 14.5%) and guidelines, policies and procedures not being adhered to/followed (n=9, 13%) (see box 1 for examples).
Examples of clinical factors attributed to the most frequently attributed root causes
Decision-making
The consultant gynaecologist could have been called 20 min earlier and the decision to proceed to laparotomy made sooner.
Lack of situational awareness
There was a lack of recognition of patient X’s clinical observations when she attended on XXX. The diagnosis of pre-eclampsia was not considered. At her attendance, patient X had new-onset proteinuria with hypertension.
Staff workload
Multiple staff statements refer to simultaneous complex medical issues arising (across all areas including triage, delivery unit and gynaecology). This may have affected staff decision-making.
Guidelines or policies not being adhered to
The Trust guideline was not followed and a urine sample was not sent. The appropriate management was admission and induction of labour within 48–72 hours, which did not happen.

{kind=link}
{kind=link}
Root causes identified in serious incident reviews grouped according to whether the affected person was from a white or minority ethnic group.
There were differences between root causes identified in women from minority ethnic groups and women of white ethnicity (p<0.001, χ2 test). Lack of situational awareness was the largest group in white women (23% of root causes) and staff workload (30%) was the most listed root cause in women from minority ethnic groups. Other root causes more frequently identified in women of white ethnic groups were lack of adherence to guidelines and decision-making. The frequency of issues relating to communication and detection of deterioration were similar between the groups. The contributory issues showed a similar pattern to the root causes with lack of situational awareness being the most common issue, followed by guidelines not being adhered to and finally overall workload being high on the unit. In terms of communication, lack of information given to women was seen as a contributory cause in one case of a mother whose first language was not English—‘There was no evidence of discussion with patient X regarding the proposed procedure (rupture of membranes at 20 weeks gestation) and its risks and benefits’.
Discussion
This study reviewed all serious incidents occurring in a single tertiary maternity unit to determine whether there were patterns that could account for the observed increased maternal and perinatal morbidity and mortality in women from ethnic minority backgrounds. High-level obstetric incidents occurred in approximately 0.15% of births in the study, with one case of maternal death. We did not find any difference in the proportion of women from ethnic minorities involved in high-level incidents compared with white women. However, there were some notable differences in both pregnancy-related factors and sociodemographic factors between the groups and in the themes of root causes identified by the serious incident reviews.
Strengths and limitations
Analysis of clinical incidents has allowed an expansion of criteria to measure both harm and the potential of harm for women during their maternity care. This study has given us insight into a cohort of women who are at risk of morbidity and mortality but have not yet been studied in the literature. Of the women who gave birth at the maternity service, 36.2% identified themselves as black, Asian or of minority ethnicity compared with 24% in England.1 Performing the study within a maternity service serving a diverse population is advantageous as it allows a greater number of ethnic minority women to be included. However, the increased diversity may limit our ability to detect or find examples of racial bias as it is possible that the staff may be more culturally sensitive as they are used to caring for women from ethnically diverse backgrounds and other services, for example, interpretation services are embedded in practice.
The main limitation to this work is the study size. Despite being one of the largest maternity units in the UK, high-level clinical incidents only make up a small proportion of births. There are no comparable studies to indicate if the relative frequency of serious incidents is similar in other maternity units in the UK to determine whether this proportion is generalisable. With limited cases, this study does not have sufficient statistical power to determine the relative risk of involvement in clinical incidents based on ethnicity. Conducting the study at one maternity service is also a limitation as the ethnic diversity in the wider population is not reflected at many other Trusts across the UK. However, a multicentre study is likely to be difficult as the quality of review of clinical incidents and subsequent investigation reports varies between Trusts. The UK Healthcare Safety Investigation Branch Maternity Programme has sought to provide standardised independent review of serious incidents in order to identify common themes and influence systemic change.26 Further detail on the theme of cultural considerations in serious incidents is due to be reported on.27
It is acknowledged the term ‘ethnic minority groups’ is limited in its applicability as it may overlook the heterogeneity of all the groups under this aggregated term and dilutes the richness of the different ethnic groups and their experiences. Larger studies using differing methodologies (including qualitative) are required to determine whether there could be differences in care-delivery and experiences of care between women of different minority ethnic groups and indeed between different groups of white women. We were unable to assess the educational level of the women involved in the incidents as this is not routinely collected data. Additionally, some risk factors for adverse outcomes were likely to have been under-reported (such as substance misuse and domestic abuse). These factors may have affected women’s access to care.
We are aware of limitations in the study design to detect unconscious and conscious bias against women of black, Asian and ethnic minorities. Investigations were led by senior members of the maternity multidisciplinary team providing an objective overview into cases. Despite the level of clinical expertise in the review of cases, reviewers may not have been sensitive to issues that from the perspective of the woman could have been attributed to differential treatment based on ethnicity or culture. Specific training on cultural awareness in maternity care may be able to tackle this and align the perspective of clinicians and childbearing women on this sensitive topic. Although not within the scope of this study, we understand the importance of listening to women’s experiences and the limitations that surround work of this type that do not address the individual concerns of the women involved.
Clinical implications
There was no difference seen in the proportion of ethnic minority women involved in high-level incidents when compared with the background maternity population (38.89% vs 36.21%). There was a trend towards higher frequency of Pakistani, Bangladeshi, black African and black Caribbean women but this increase was not statistically significant. Findings suggest there are risk factors which make women, regardless of ethnicity, more likely to be involved in serious clinical incidents. For example, having a pre-existing medical problem (61.1%) or developing an obstetric problem (63.9%) during the pregnancy. Women within the ethnic minority group had lower frequency of pre-existing medical problems or obstetric problems than white women however, and this may indicate an over-representation of women in the ethnic minority group being involved in high-level investigations, but numbers are too small to confirm this. If confirmed, further work is required to understand why women from ethnic minority groups have similar numbers of adverse incidents in the presence of fewer risk factors than white British women. Nevertheless, our small population reflects other findings already published in the literature—women from deprived backgrounds, women with poor antenatal care and women born abroad are at an increased risk of poor pregnancy outcomes.
Importantly, booking late in the pregnancy occurred more frequently in women from ethnic minorities who were involved in high level incidents. This is particularly important in that it places women from minority ethnic groups at greater risk of not having adequate antenatal care (with 36% of ethnic minority women booking after 12 weeks compared with just 9% of white women in our study population) and is something that is potentially modifiable. Background rates of booking after 12 weeks of pregnancy for the two maternity sites indicate an overall rate of 18%; the rate for non-white women was 32% and white women 16% (p<0.001). Booking late for antenatal care may be linked with discrimination and racial microaggressions,28 29 as well as economic status.29 Reasons for late booking are complex, involving both service user and healthcare factors, and may include poor reproductive health knowledge and delayed pregnancy recognition, previous pregnancy experience and the perceived value of antenatal care.30 31
Poverty is inextricably linked to maternity health outcomes, and it was notable that a greater proportion of women in our cohort (47.2%) were from the most deprived quintile compared with women who died (32%) in the latest Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries across the UK (MBRRACE) report.4 Our findings suggest that access to and engagement with antenatal care may need to be adapted for women from minority ethnic groups, particularly in those who also come from social disadvantage. Integrated public health strategies that address the complexities contributing to inequalities in outcomes for women living in communities of social disadvantage and ethnic diversity is urgently needed.32
Women from ethnic minority backgrounds did not appear to be the subject of a more severe level of harm incidents than white women. There was no clear evidence in this study to make the argument that conscious or unconscious bias has impacted the care of women from minority groups. However, the SI investigations were not designed to specifically look at ethnicity and whether conscious or unconscious bias could have been a contributing factor. This may have been missed by the investigators. Analysis has shown that the causes of high-level obstetric incidents were multifactorial. In many cases, similar themes occurred despite ethnicity and were often a combination of team, staff and task factors. Despite communication being suggested as a potential barrier to good quality healthcare for ethnic minority groups, lack of communication to women and their families only occurred in a small proportion of cases and was seldom identified as a root cause. In the cases of serious incidents affecting women from ethnic minority groups, more frequently cited root causes related to staffing levels and workload, and a failure to seek support from more experienced staff. This may suggest that when there are problems on an institutional level, women who are already disadvantaged or at-risk suffer more. This requires more detailed study, potentially adopting an ethnographic approach to observe staff behaviour. Furthermore, as the root causes of adverse events may occur at multiple, different time points, we were not able to evaluate whether staffing levels (both in terms of absolute number and seniority) differed between women of different ethnic groups. However, this also merits further examination to determine whether the difference in the number or experience of carers led to the staffing issues and problems with decision-making identified in the incident reviews. This level of analysis could be achieved using the approach employed by MBRRACE Confidential Enquiries applying forensic examination of the case records.
Conclusion
Overall, this study has demonstrated that women from ethnic minority groups in this Trust were not at an increased risk of being involved in high-level maternity incidents, however there were differences in the root causes of adverse incidents. Despite no overall increased risk, the data support findings that women from more deprived backgrounds, women who initiate pregnancy care late; women born abroad or women with previous medical problems are at an increased risk of being involved in a serious incident. These factors affect women from minority groups disproportionally and need to be urgently addressed and tackled to improve maternity outcomes in those groups. Although limited, the data do not suggest that women from ethnic minority groups are being treated or cared for differently, however there are recurring themes contributing to poor outcomes, occurring in the care of all women.
Maternal health remains a public health issue and a priority. This work demonstrates the increased risk that marginalised and disadvantaged women are facing. Maternal mortality data alone are limited and do not fully capture the scope of the issue. If we are to reverse the trend of widening inequalities in maternal health outcomes, we need to truly understand the complexities of the problem and support the most vulnerable women which also encompasses in-depth reviews of morbidity and near misses as well as mortality.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @kykywatson, @MCR_SB_Research
Contributors The project was planned by SV, KW and AH. Severe incidents were identified by HB and SR. Data were extracted by DF, KF, HB and SR. Data were analysed by KF, KW and AH. DF, KF, KW, SV and AH wrote and edited the manuscript. SV is the guarantor for this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.