Article Text

Abstract
Introduction University Hospitals of Leicester (UHL) has co-developed and deployed a novel Electronic Prescribing and Medicines Administration (EPMA) application as part of the trust electronic patient record (EPR) programme that meets specific clinical demands and interoperability standards of the National Health Service (NHS) despite clinical pressures from the COVID-19 pandemic.
Methods Following an initial limited pilot deployment, a big-bang whole site-based approach allowed transition of 1844 acute adult inpatients beds from an existing standalone EMPA to the new system. This project used a frontline driven and agile management strategy. Clinical risk was managed using a combination of standard risk logs, robust clinical prototyping and robust disaster recovery plans. Early engagement with clinical teams allowed for advanced product configuration before live deployment and reduced the need for sustained transition support for clinical staff.
Results An iterative, well-governed approach, led by a combination of information technology (IT) and clinical staff with a responsive vendor, enabled a complex new EPMA system in a large acute NHS trust to be deployed with limited resources despite the ongoing COVID-19 pandemic.
Discussion The development and deployment of EMPA and EPR systems across NHS trusts is a key enabler for better healthcare delivery. This case study shows it is possible to deploy a new clinical IT system at scale without interruption of clinical services and with a relatively modest deployment team. Sustainability of the project was also ensured through a clear clinically led governance structure to manage risk quickly and carry lessons learnt onto new developments.
- Leadership
- Healthcare quality improvement
- Data Accuracy
- Decision support, clinical
- Information technology
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Leadership
- Healthcare quality improvement
- Data Accuracy
- Decision support, clinical
- Information technology
WHAT IS ALREADY KNOWN ON THIS TOPIC
The deployment of modern information technology (IT) systems in the National Health Service (NHS) is a key mandate for the NHS Transformation programme. Electronic Prescribing and Medicine Administration (EPMA) systems are a cornerstone of any clinical digital system; however, their deployment and development present ongoing challenges for many NHS trusts in England.
WHAT THIS STUDY ADDS
This case study demonstrates a project management methodology that allowed University Hospitals Leicester Trust to develop and deliver a modern EPMA solution within the usual financial and clinical pressure all NHS organisations experience during the COVID-19 pandemic.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This case study provides a roadmap to enable other trusts in similar positions to deliver complex IT projects sustainably at pace.
Adequate preparation, careful risk management, clinical engagement and learning from pilot deployments are highlighted as catalysts, while inadequate risk management is shown to be a downfall.
These lessons are vital and must be considered in practice in the evolving landscape of digital healthcare.
Background
The deployment of modern information technology (IT) systems in the National Health Service (NHS) is a key mandate for the NHS Transformation programme. Electronic Prescribing and Medicine Administration (EPMA) systems are a cornerstone of any clinical digital system; however, their deployment and development present ongoing challenges for many NHS trusts in England.1
Report implications
This case study demonstrates a project management methodology that allowed University Hospitals of Leicester (UHL) NHS Trust to develop and deliver a modern EPMA solution sustainably within the financial and clinical pressure NHS organisations experienced during the COVID-19 pandemic.
Problem description
University Hospitals of Leicester, with acute services located at three different physical sites, was one of the first hospitals in the UK to implement Medchart Electronic Prescribing and Medicines Administration (EPMA) from the Dedalus Group in 2011. Rollout and removal of paper drug charts began on the Leicester Royal Infirmary (LRI) site in November 2011 and included the bone marrow transplant, haematology, oncology, trauma and orthopaedics units alongside associated theatres. However, rollout stalled because of technical problems and staff training requirements, resulting in the system being fully deployed across the trust by October 2018.
In parallel, OptiMed Medicines Management Service, a closed-loop medicines management solution, was trialled at Leicester General Hospital (LGH). This solution was used on four renal wards and introduced in April 2015.2 However, this project faced significant problems with software implementation and limited development. Therefore, the renal wards transitioned to Medchart EMPA software in 2018.
In 2018, UHL commissioned Nervecentre to develop a new NHS specific EPR (electronic patient record), after ongoing technical issues with existing EPMA systems in the trust. This EPR needed to be deployed across three hospitals sites and 1844 inpatient beds during the COVID-19 pandemic.
Methodology
A collaborative development project with the EPMA module, eMeds, was viewed as an essential first step for the EPR project. An agile approach to project management was taken, with front-line engagement from with pharmacists, nurses and doctors inputting into board meetings chaired by the information technology (IT) department and vendor representatives.
After extensive technical and clinical testing, in September 2019, a pilot of the Nervecentre EPMA application started at LGH within the renal unit. This pilot was very successful and used as a test bed for wider trust deployment methodology.3 Wider trust deployment of the EPMA module was completed in June 2021 despite the COVID-19 pandemic by a conservative number of transition staff using a remote transition process.
Controlling and monitoring the remote transition progress
A specific protocol allowed for learning and accurate governance. The team used a paper checklist process to record key components of transcription and verification (online supplemental content 1). The transition team personnel (transcribers, then verifiers) were given the paper checklist with a bed location on a ward to transition across EPMA applications. They then found the patient identifier details for the patient in that bed. These paper checklist data were collated and recorded on a computer spreadsheet held in Microsoft Teams (online supplemental content 2), summarising patient and ward transition progress. Therefore, the team were able to monitor transition progress electronically (via the Teams spreadsheet) and share these live data if required. Care was required not to miss patients who were in transit and not allocated a bed on the primary application.
Supplemental material
Supplemental material
Training
Data from the pilot in the renal wards indicated the new EMPA system was easy to use and identified specific areas of training to help staff transition. All clinical staff were expected to complete 1.5 hours of online Nervecentre EPMA training prior to rollout in their areas. This consisted of a series of short videos covering key functionality of the EPMA application and highlighted the differences in appearance, navigation and functionality of the desktop and the app. Staff were encouraged to try using the new application in the online training environment and posters were displayed in clinical areas with key points and QR codes linking directly to these short training videos. All clinical areas were asked to nominate champions to help support uptake and engagement alongside the team also offering online training sessions aimed at basic users and champions.
Results
The team were able to transition to a new EPMA system, during a 09:00–17:00 day using a minimal number of staff, across multiple sites base through the protocol. Table 1 demonstrates the numbers of staff required for each site and go-live date.
Workforce needed during the transcription process
Transitioning team composition
Ensuring transition staff were available for each day was a major challenge for the team. Doctors and pharmacists were released from clinical duties or paid overtime. Transcribing started around 08:30 with the planning assumption being for four charts per hour per transcriber/verifier. The first site to go live used the four charts per hour but this proved to be an overestimate and reduced the aim to three charts per hour. To improve the pace of prescribing, staff were re-used if they had been involved on another other site. Moreover, support from senior clinicians and specialist practitioners helped address any prescribing concerns.
The EMeds project team included the deputy chief operating officer who worked closely with the site management teams. This interaction proved useful during the LRI and Glenfield transition as the Trust was at OPEL 4 escalation with significant operational pressures. The oversight team coordinated with the Trust tactical command to ensure patient flow was not compromised during the transition process. The following transition order principles were critical for success and will be utilised in future deployments of the EPR:
Emergency admissions areas first followed by medical base wards and then surgical wards.
All new admissions (including elective surgery) to start on the new application from 07:00.
All patients going to theatres to have prescribing done on the new application thus avoiding dual EPMA application use in the theatre department.
All transcribers start transitioning when the old EPMA prescribing function was turned off. Once all verifying was complete, then the old EPMA drug administration function is turned off. The average duration of transcribing and verifying for a ward is 1 hour.
Once the old EPMA ward prescribing function is turned off, all the patients drug records are made on the new EPMA application quickly, minimising the risk of selecting the wrong application.
Posters placed above the patient’s bed effectively alert the ward staff which system to use for which patient.
Avoid transitioning a ward over the lunchtime drug round or removing drug administration function on the old EPMA during a drug round.
Safety
Through a retrospective Datix (clinical incident) review, five reported adverse events were uncovered. One incident caused minor harm to a patient as their dose of medication was delayed by a day resulting in a delayed discharge. The other four adverse events caused no harm to patients. These were two transcription prescription errors; a patient being missed during transcription and a patient being transferred between two sites using different systems without a printout. Posters indicating the system at use were not placed above patient’s bed in Glenfield Hospital, thus leading to confusion and some wards using the wrong EPMA during drug rounds. Overall, this complex transition successfully maintained patient safety.
Floor walking and telephone support for clinical teams
A team of ‘floor walkers’ were briefed on common questions and solutions to help with clinical transition during the deployment phase (table 2). The floor walking support team consisted of nurse clinical IT facilitators, medicines management nurses, pharmacists, members of the IT department and trainers from Nervecentre. The team moved throughout a transitioning hospital and was able to focus their support on recently transitioned areas and ward drug rounds. The team was available from 07:007 until 21:00 onsite. During the weekend, there was less on-site support; however, there was telephone support assisted by specialist WhatsApp groups.
Floor walking support needed during the transition
Disaster recovery planning
The project team placed clear disaster recovery plans before the start of any deployment process. The disaster recovery planning was persistently reviewed during board meetings to ensure clinical work could continue in the event of a catastrophic systems failure.
Discussion
The deployment of novel IT clinical infrastructure in the NHS is difficult even with fully developed products.4 The project team had learnt, from past IT deployments in the trust, that system preparation, clinical engagement and careful risk assessment were all key prerequisites to successful deployment and will be essential in future EPR rollout. As a result, the new EMPA system was deployed in the three-site trust with relatively modest resources and no compromise to clinical care.
Project timeline and team engagement
The rollout took approximately 2 years to plan and implement. This was longer than expected due to pandemic delays and unexpected software challenges. It was essential to keep engagement with all clinical management groups through sharing the project plans and appointing local EPMA to ensure ongoing clinical awareness. To manage expectations of users, the project was discussed in numerous clinical medical, nursing and pharmacy forums to keep clinical stakeholders aware of reasons for delay. Moreover, this engagement ensures that the decisions made were felt to be sustainable for all groups involved.
Executive support and project management
In addition to the project board, a weekly Operational Task & Finish Group (chaired by the chief operating officer) was initiated to oversee the local preparation of each hospital site before the rollout. The project had support from executive boards to use an agile approach to deployment. There was significant concern that the change process associated with the new eMeds application would slow patient flow through the hospital and delay discharge. However, by deploying agile methodology, the project team was able to demonstrate incremental improvements in the deployment plan and implement clear risk reduction strategies as the project developed. Local service managers and senior nurses who had valuable frontline experience were used to help in deployment planning. This methodology helped reduce concerns at the executive board level and lays a roadmap for future success.
Clinical area preparation
The total number of hours spent on pre-roll out preparation work for all three hospital sites was 1688 hours. The IT nurse facilitators and IT hardware team walked around all clinical areas before rollout and spoke to staff about the project and were able to address any computer hardware issues, therefore reducing the chance of failure during deployment day.
Discussions took place with other large NHS trusts that had transitioned EPMA applications to help guide internal strategy. All had different challenges including transition speed and how to mitigate clinical risk during translation. There were broadly four models of transitioning pathways identified (figure 1).
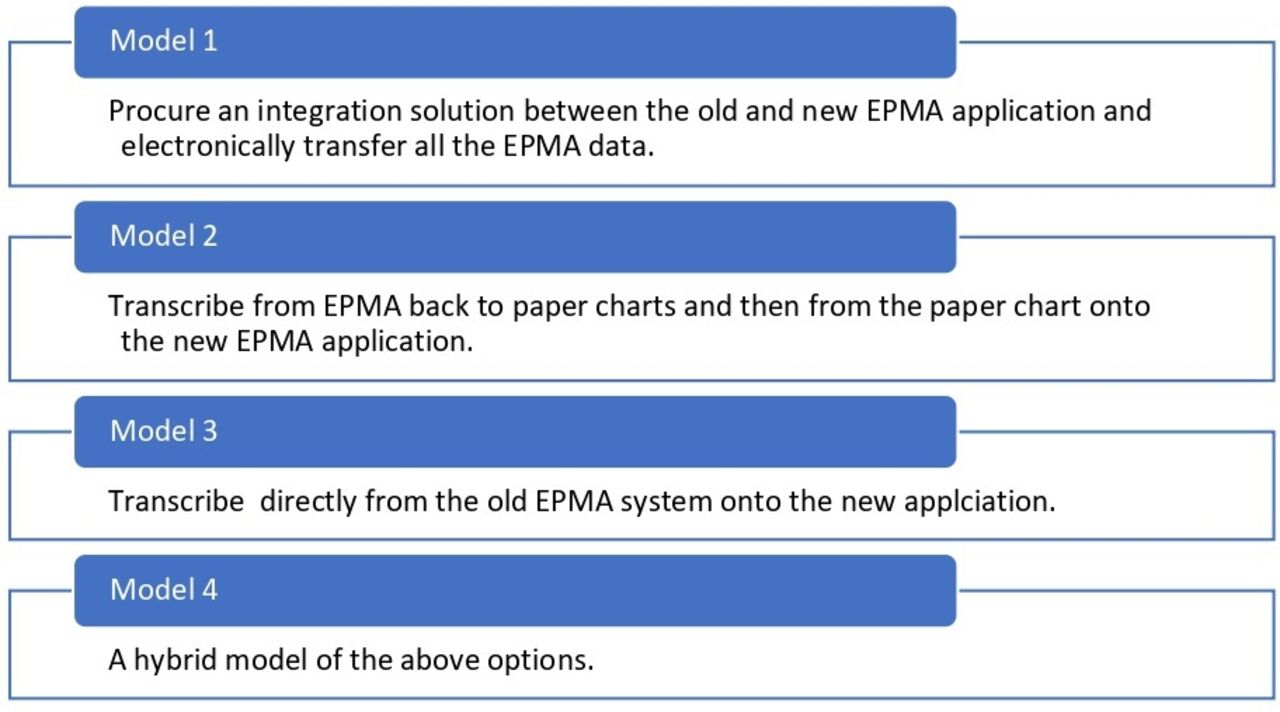
Models of transitioning Electronic Prescribing and Medicines Administration (EPMA) applications.
Deployment planning
To ensure smooth deployment, the project team also focused on clinical process change engagement. Previous experience of ‘Top down’ IT-driven projects demanded a high level of clinical support to engage front-line staff. The focus of the project team was therefore to ensure a ‘front-line lead’ approach to deployment; therefore, reducing the IT supported needed to deliver the change process in the long term. Clinical staff, including doctors, nurses, pharmacists, made up to 50% of members in board meetings along with IT and vendor representatives. The board implemented an agile approach to project management,5 with a focus on the deployment of rapidly evolving prototypes rather than a focus on ensuring final technical product specifications. The front-line lead approach engaged service users early ensuring clinical buy-in, and the agile pilot projects identified and addressed issues before the final rollout.
Alongside the agile management approach for project planning, the team decided on a modified ‘big bang’-based approach (model 3) for transitioning. This decision was justified through risk assessment and analysis of the initial ‘pilot’ deployment.5 The three sites have 1844 beds (360, 441 and 1043). A review of the pilot project confirmed a ‘big bang’ method at each different hospital site minimised the number of patients who moved between clinical areas using different EPMA applications. The main clinical risk was ensuring no patient had two ‘active’ prescriptions on different systems during translation process.
Clinical risk management and mitigation were a major challenge that required resolution to ensure rapid project deployment. A careful balance between risk management and pushing back deployment timelines due to unknown risks was met through effective project planning. Therefore, the eHospital team now uses a Patient Administration Services (PAS) deployment to help with future project planning and innovative developments.
A risk log was used to quantify clinical risk. The following questions were considered about the transition process (table 3).
Transcription considerations
The team chose to run the drug chart transcription process from a single location on site but remote to the wards affected. Clinical teams at all three sites were consulted on the best day for deployment to avoid busy clinical times and planned staff rotations.
Leicester General Hospital: 308 active beds transitioned on a Tuesday.
Leicester Royal Infirmary: 913 active beds, transitioned across 2 days. Surgery and theatres on a Tuesday and Medical areas on the following Thursday.
Glenfield Hospital: 444 active beds transitioned on a Wednesday.
The initial plan of each site to adopt the new EPMA system within 2 weeks of each other would have prevented manual transcription between systems for patients that had inter-site transfers. However, clinical pressures from the COVID-19 pandemic meant go-live dates between each site had to be significantly staggered. The value of risk log therefore showed with temporary clinical pathways being adopted to avoid clinical errors associated with having two active EPMA systems within the trust. Such risk logs are thus essential in all future EPMA deployments.
Drug configuration
In the months prior to rollout, all specialities and their lead doctors, pharmacists and nurses were consulted to ensure the correct drug configuration. Drug order sets were geared towards efficient standardised prescribing. This piece of work was essential to avoid prescribing delays during the rollout. Most prescriptions are based on predefined drug sentences (name, dose, route, frequency) as this is the quickest and safest way to use the application.
Clinical engagement was a key item identified on the project risk log, and front-line clinicians, nurses and pharmacists were invited to attend all board meetings to give input on system configuration and staff training requirements. The eHosptial team now actively allocate resources to ensure local clinical teams can be released to help with local system configuration in future developments.
Remote transition during deployment
Alongside abiding by key principles of the transcription process (figure 2), the team undertook various activities to calculate the number of transcribers and verifiers required for deployment of eMeds at each site:
Specialities analysed for the average number of drugs per patient.
The team tested the duration of time it took to transcribe from Medchart to Nervecentre on a single laptop.
During the pilot, the team monitored the time for chart transition.
The team used examples from other hospitals described in the literature.

{kind=link}
{kind=link}
Key principles of the transcription process. EPMA, Electronic Prescribing and Medicines Administration; EPR, electronic patient record; IT, information technology.
The team found patients ranged from 0 to 35 prescriptions on their chart, with an average of 20 prescriptions for medical areas, 17 for surgical and 6 for obstetrics. Testing showed transcription took between 0.5 and 1 min per prescription. On this basis, transcribing and verifying rates were estimated at of between three and four drug charts per hour.
There are many variables that had to be account for during the deployment day.
Experience and speed of transcribing/verifying workforce.
Unexpected drug configuration issues.
Empty beds.
Volume of day-case patients.
Number of new admissions on the day (which would not need transcribing).
The team generally used junior doctors for transcribing and pharmacists for verifying. This maximises their skills for efficient working. Consideration was given to other staff groups including final year medical students and nurse prescribers. However, it was recognised these groups may require more supervision and possibly work slower.
Conclusion
The development and deployment of EMPA and EPR systems across NHS trusts is a key enabler for better healthcare delivery. Adequate preparation, careful risk management, clinical engagement and learning from pilot deployments allow for complex EPMA systems to be deployed in the NHS with moderate resources. However, resources dedicated to project planning with executive support is vital, as large IT projects require adequate clinical input and configuration to be deployed successfully and sustainably.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We thank the eMeds Team at University Hospitals Leicester for their support on this project.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Permission People: All individuals have given their consent for the images and figures to be published. Brands: All brands have given their consent for the images and figures of their brands to be published.
Contributors All authors were involved in the implementation and write up of the project. G.S acts as the guarantor of the above project.
Funding Funding for the project was provided by University Hospitals Leicester and Nervecentre. No award/grant number.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.