Article Text

Abstract
Introduction With the emergence of SARS-Cov-2, the Centers for Disease Control and Prevention (CDC) defined mandatory guidelines for donning and doffing personal protective equipment (PPE) among dental healthcare professionals. The study’s objective was to improve the compliance of the donning and doffing protocols for PPE among dental practitioners by the Plan, Do, Study, and Act (PDSA) cycle.
Materials and methods A quasi-experimental study was conducted on a sample of dental healthcare professionals using the non-probability purposive technique. In the first planning stage, compliance with CDC-approved donning and doffing was assessed on the clinical premises. In the second stage, an educational session was arranged with all the healthcare professionals to explain stepwise guidelines of donning and doffing to improve the quality of donning and doffing compliance. In the third stage, improvement in the quality outcome was then assessed after the session. Data were normally distributed. Qualitative variables for all the steps of donning and doffing are reported as frequency and percentages. Pareto charts were made to assess the non-compliance rate for donning and doffing protocols among dental healthcare professionals.
Results There was an improvement of 44.55% in the hand hygiene practices before wearing the PPE after the second step of the PDSA cycle. A percentage improvement of 7.4% was recorded for removing jewellery, wearing the gown and wearing a surgical cap. No improvement was seen in securing the mask/ respirator ties, washing hands after wearing the respirator, placing the goggles or face shield practices.
Conclusions PDSA cycle improved the overall compliance to PPE donning and doffing practices. Most of the protocols were followed by the dental healthcare professionals; however, some of them remained the same or worsened due to ease in SARS-CoV 2 restrictions.
- COVID-19
- Quality improvement
- Continuous quality improvement
Data availability statement
Data are available on reasonable request. Supporting data are available with the corresponding author in the form of hospital records.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Plan, Do, Study, Act (PDSA) cycle is a study design for rapidly testing a change in improvement of quality.
WHAT THIS STUDY ADDS
In this study, we used PDSA cycle on steps of donning and doffing of personal protective equipment (PPE) among dental professionals. PDSA cycle improved overall compliance to PPE donning and doffing practices.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Goal was to assess advantage of PDSA model in reinforcing mandatory protocol, steps in an emergency, in healthcare environment. Since improvement was observed in 18 steps of donning and doffing, which proves that this model can be employed globally to improve the quality.
Introduction
With the emergence of SARS-CoV2, the infection control guidelines for dentists became more stringent than ever. The coronavirus pandemic intensified rapidly after being diagnosed in China in 2019 with reportedly a wide range of signs and symptoms.1 The SARS-Cov-2 is transmitted through droplet inhalation or coming in contact with a contaminated surface and subsequent contact with oral, nasal, or eye mucosa.2 The exact clinical manifestations of SARS-Cov-19 are still unclear but some common symptoms reported include fever, sore throat, and shortness of breath while some patients may remain completely asymptomatic.3 4 Due to the risk of virus transmission from aerosol-generating procedures many countries only allowed dentists to provide emergency treatments5–7 while postponing all elective treatments.8 Preventing the spread of the infection was the most desired outcome for public health.1 9 10 Over time, the healthcare authorities were not only able to understand the viral pathology better, but several preventive measures such as social distancing, hand hygiene, wearing of a mask, use of personal protective equipment (PPE) and vaccination against SARS-Cov-2 were introduced and implemented.11
WHO declared PPE mandatory for all health workers including dentists. Based on the risk of exposure, the healthcare providers were classified using the occupational risk pyramid developed by the Occupational Safety and Health Administration department. According to this department, dental healthcare providers (DHCP) were classified as ‘very high risk’.8 12 To minimise the risk of virus transmission in dental clinics, a proper advised protocol for donning and disposing of PPE should be followed.6 The Centers for Disease Control and Prevention (CDC) then defined a mandatory protocol for donning and doffing PPE.13 Hegde reported that cross-infection can be restricted to 98% if defined donning and doffing guidelines are properly followed.14 Even slight negligence in following the protocols can lead to serious consequences to the safety of healthcare professionals as well as patients.
Another recent quality improvement (QI) project15 conducted on donning and doffing used evidence-based literature and QI tools to design and operationalise donning and doffing areas with a focus on people, tasks, and environment among ward healthcare providers.
The Plan, Do, Study, Act (PDSA) cycle is an accepted study design for rapidly testing a change in the improvement of quality.16 Methodology of this systematic study is planning it, trying it, observing the results, and acting on what is learnt. It is a scientific method used for action-oriented learning. Once the changes are thoroughly tested, PDSA cycles can be used to implement or spread these changes and improve the quality ofany system or organisation.17
In this study, we used the PDSA cycle on the steps of donning and doffing PPE among dental healthcare professionals. The short-term outcome of this PDSA model was to increase the compliance of donning and doffing of PPE among dental healthcare professionals. The long-term goal was to assess the advantage of the PDSA model in reinforcing any mandatory protocol, steps to be followed in an emergency, and novel protocols being introduced in the healthcare environment.
Materials and methods
The study design was quasi-experimental with a non-probability sampling technique.
A total of 27 participants including Faculty, Residents, dental hygienist, and dental assistants were included in the study. The sample size was calculated using the formula n= (8 ([CV]2 [1+[(1-PC)]2].)/[PC]2 with the value of coefficient of variation in per cent (CV) as 20 and percentage change (PC) in means as 15.18
Inflation of 10% for the non-response rate was added to achieve 80% power. All dental care professionals aged over 18 years including faculty members, hygienists and dental assistants regularly dealing with patients during the pandemic were included in the study from December 2020. We excluded the professionals who were allocated by the department to assess donning and doffing of the PPE. The evaluating team consisted of a dental floor supervisor, a dental resident, and a consultant. All of these evaluators had a minimum 3 years of work experience.
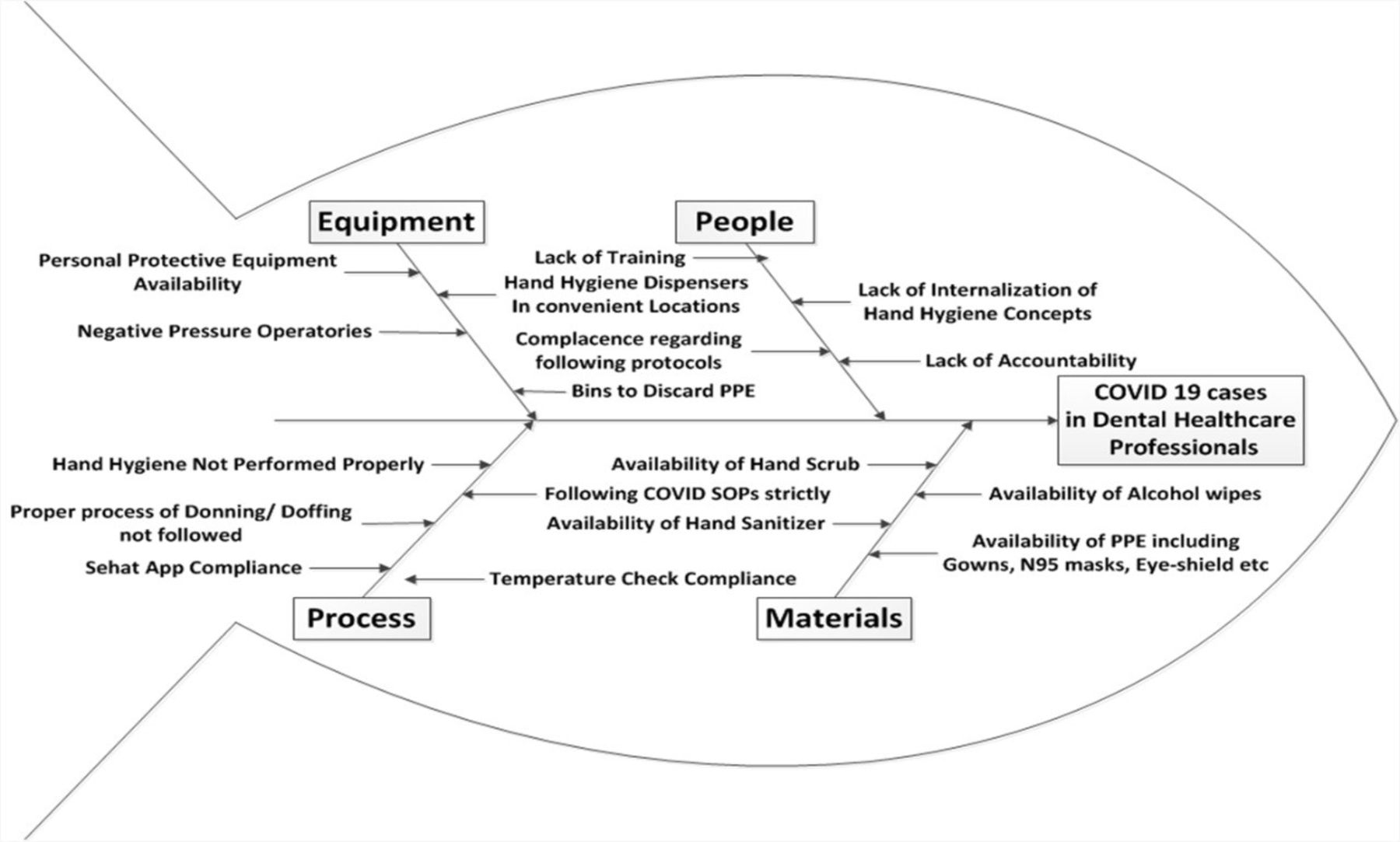
The fishbone diagram was used to assess the potential causes of non-compliance to the PPE guidelines among dental healthcare professionals (figure 1). Data were collected by well-defined guidelines of CDC and approved by AKUH of donning and doffing of PPE steps were recorded (table 1).

Fish-bone diagram. PPE, personal protective equipment.
Percentage of compliance of guidelines of donning and doffing of PPE dental care professionals
The first phase of planning started in the beginning of the surge of SARS-CoV 2 cross-pandemic, the data of compliance of donning and doffing of PPE by dental healthcare professionals were recorded in December 2020. In January 2022, the second stage of the Do phase was conducted where DHCP were educated about the protocols of donning and doffing of PPE by a session conducted on zoom link by a member of the infection control team. Leaflets were distributed and posters were pasted on the walls of the staff lounge, resident and faculty room, and clinical premises. Not only this, weekly emails were forwarded with CDC approved e-posters on the steps of donning and doffing. In May 2022, the third study phase data of compliance to follow steps of donning and doffing of PPE was recollected and compared to analyse the difference. In the final phase of Act, quarterly seminars will be conducted on based on the results obtained by the PDSA cycle.
Patient and public involvement statement
Patients were not involved in the design, recruitment, and conduct of this study.
Statistical analysis
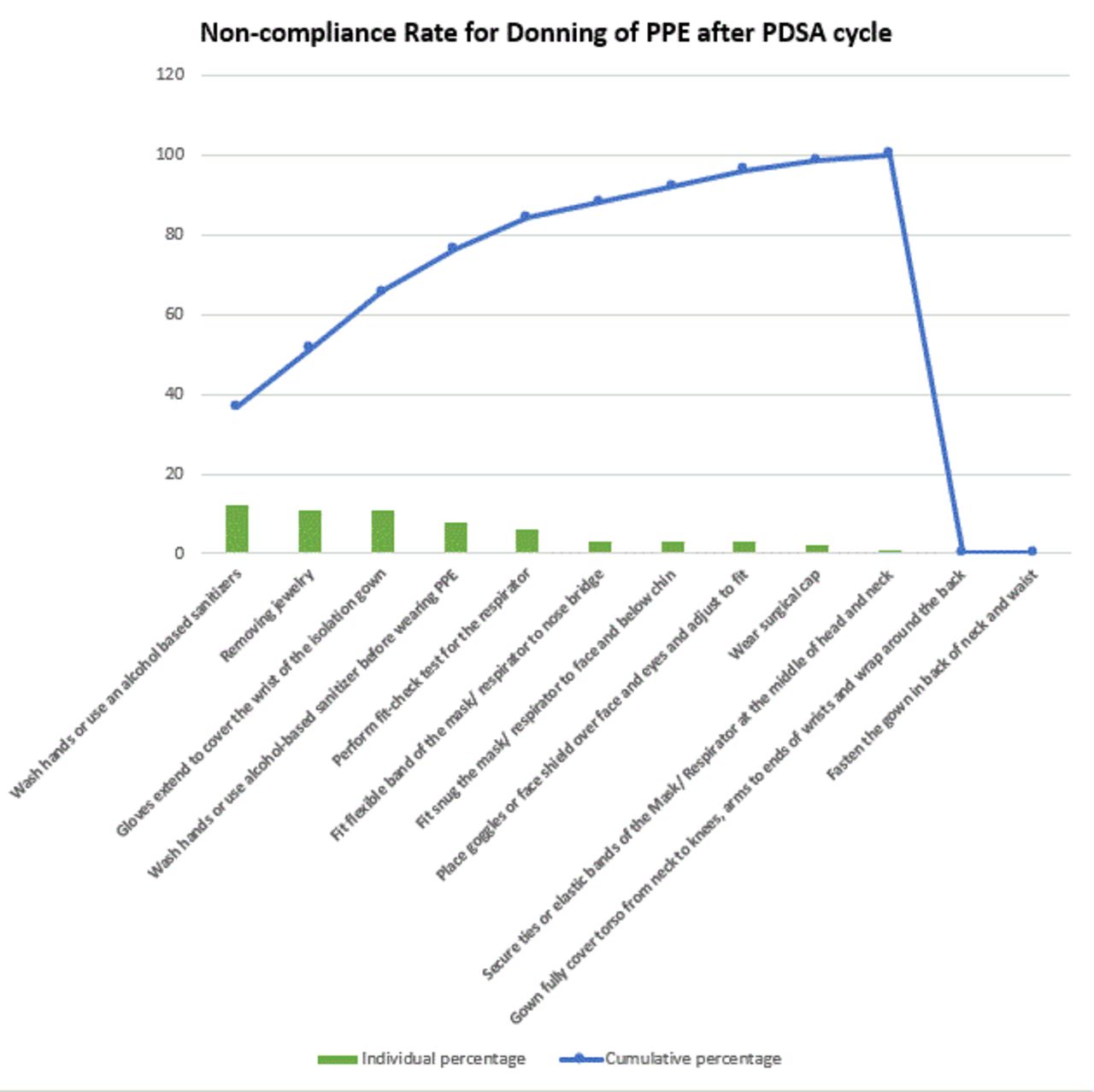
Data were double entered and analysed in SPSS for windows (V.20.0, SPSS). Frequencies and percentages were calculated for the steps of donning and doffing before and after the PDSA cycle. Pareto charts were made to assess the non-compliance rate by the dental healthcare professionals for the quality of steps of donning (figure 2) and doffing before the PDSA cycle (figure 3) and after the PDSA cycle (figures 4 and 5).

Non-compliance rate for donning before PDSA cycle. PDSA, plan, do, study and act.

Non-compliance rate for doffing before PDSA cycle. PDSA, plan, do, study and act.
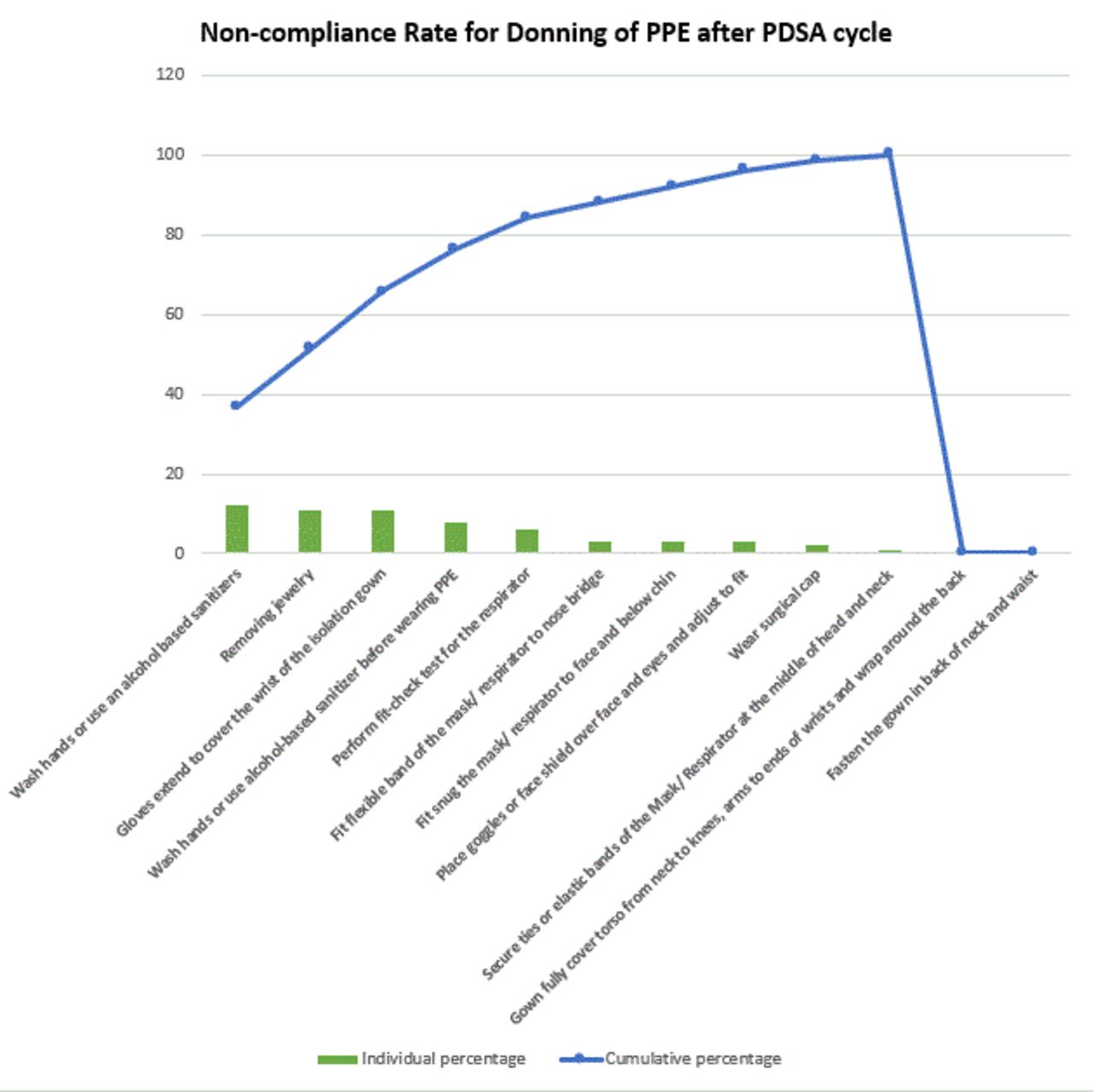
Non-compliance rate for donning after PDSA cycle. PDSA, plan, do, study and act.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Non-compliance rate for doffing after PDSA cycle. PDSA, plan, do, study and act.
Results
Frequencies and percentages of the donning and doffing of PPE before and after the PDSA have been summarised in table 1. Improvement (44.55%) was recorded in the hand hygiene practices before wearing the PPE. On the contrary, the participants did not wash their hands after placing goggles and face shields as recommended by the CDC and the university protocol. A percentage improvement of around 7.4% was recorded for removing jewellery, wearing the gown, and wearing a surgical cap. 70.4% (n=19) of the participants were checking their temperature and filing the Sehat check application before the PDSA cycle was implemented in the facility. The app was developed by the University and was available for the employees. During the pandemic, it was made mandatory for every employee to mark symptoms like fever, sore throat and myalgia before coming to the hospital. In case of any positive symptoms, the employee was asked to stay isolated, monitor symptoms, and get PCR tested to rule out the chances of COVID-19. However, the participants were not recording these parameters after the PDSA cycle. The last two protocols of the checklist that is, saving the mask following the guidelines and performing hand hygiene at the end of doffing did not improve, in fact, they worsened after the PDSA cycle. No improvement was seen in securing the mask/ respirator ties, washing hands after wearing the respirator or placing the goggles or face shield practices (table 1).
While recording the participant’s compliance to the doffing protocols of the PPE, the highest percentage improvement (22.2%) was seen in removing the goggles and the face shield from the back by lifting the headband or earpieces followed by a percentage improvement of 11.1% for removing and discard the surgical cap. Out of 11 steps suggested for the doffing of PPE, participants’ practices worsened while performing six of the steps (step number 12, 13, 20, 22, 23, 24) (table 1).
Discussion
Data were collected for 27 participants and based on that, 2 major issues were identified in the donning practices. Majority of the study participants were not removing jewellery and only 7 out of 27 were washing their hands before wearing the PPE. The major issues identified for the doffing of the PPE were taking off the gloves following the proper protocol, unfastening the gown ties taking care that the sleeves don’t touch the body, and performing hand hygiene after doffing the PPE. All DHCP were educated about the protocols of donning and doffing the PPE.
In this study, Pareto charts were used to compare the non-compliance rate of donning and doffing before and after the PDSA cycle. The Pareto charts are based on the 80–20 principle, that is, 80% of the problems come from 20% of the causes (Vital few).15 We used them in our study to identify the major problems in donning and doffing in our department. Once the major issues were identified they were addressed in the training sessions. Since we did not observe major improvements in these, they should be again reinforced in the next PDSA cycle.
After the implementation of a PDSA cycle, data were recollected for the same group of people. We found major improvements in the donning protocol in our study sample, 7.4% improvement in removing jewellery practices, and 44.55% in hand hygiene practices before wearing the PPE. However, we noticed that some of the protocols worsened when we recollected the data. It can be attributed to various factors, among which the most important is an ease in COVID-19 restrictions as the pandemic got better. Decreased COVID-19 surge and mortality rate, availability of vaccinations and increased awareness regarding the spread of this cross-infection with time, gradually decreased strict compliance of dental healthcare professionals for donning and doffing.
Leaflets were distributed in the department and quarterly seminars were conducted so that the dental practitioners continue following the protocols.
The findings of our study coincide with that of Meisha. She also reported not following hand hygiene practices after removing gloves as the most common violation.8 Tysiac-Mista and Dziedzic, in their study, explored the attitudes and professional approaches of dental practitioners in Poland and reported that 71.2% of the dentist suspended their practices during the COVID-19 outbreak due to a shortage of PPE.19 A study conducted in India reported that one-third of their study subjects were not aware of the PPE protocols when the pandemic occurred.20
We will extend the PDSA cycle again and analyse improvement in donning and doffing after conducting further seminars. With the emerging new variants of the COVID-19 virus, WHO guidelines for donning and doffing are also changing hence, seminars and sessions will be conducted again according to the new guidelines. The major strength of our study is that it is the first study conducted in Pakistan that utilised the PDSA cycle to improve the donning and doffing protocols in a dental setting. It will serve as a basis for conducting future studies. However, the limitations of this study are it is a single centred study, descriptive statistics of dental healthcare professionals were not recorded, and the results cannot be generalised. Since improvement was observed in 18 steps of donning and doffing, which proves that this model can be employed globally to improve the quality.
Conclusions
In conclusion, most of the PPE donning and doffing protocols improved after educating the DHCP. The majority of the protocols were followed by the study participants, however, few of the steps either did not improve or worsened after the educational sessions. The major reason for this could be the decline in the COVID-19 cases and the ease in COVID-19 restrictions worldwide.
Data availability statement
Data are available on reasonable request. Supporting data are available with the corresponding author in the form of hospital records.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted in the dental clinics of the Aga Khan University Hospital (AKUH) after obtaining ethical approval from the Ethical Review Committee (ERC # 2022-6748-20374) of the university.
References
Footnotes
Contributors HQ: topic selection, protocol writing, ERC approval, data analysis. FA: data analysis, data interpretation, and manuscript writing. NB: Data collection. RHS: topic confirmation, data analysis and data interpretation. RHS is the author responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.