Article Text

Abstract
Rib fractures represent a substantial health burden. Chest injuries contribute to 25% of deaths after trauma and survivors can experience long-standing consequences, such as reduced functional capabilities and loss of employment. Over recent years, there has been an increase in the awareness of the importance of early identification, aggressive pain management and adequate safety netting for patients with chest injuries. Substandard management leads to increased rates of morbidity and mortality. The development of protocols in the emergency department (ED) for management of patients with chest wall injuries has demonstrated reduction of complication rates.
Our aim was to develop an evidence-based, multidisciplinary chest injury pathway for the management of patients presenting with rib injury to our ED.
Prior to implementation of the pathway in our department, only 39% of patients were documented as having received analgesia and only 7% of discharged patients had documented written verbal advice. There was no standardised method to perform regional anaesthetic blocks. Using quality improvement methods, we standardised imaging modality, risk stratification with a scoring system, analgesia with emphasis on regional anaesthesia blocks and disposition with information leaflets for those discharged.
Implementation of the pathway increased rates of documented analgesia received from 39% to 70%. The number of regional anaesthetic blocks performed went from 0% to 60% and the number of patients receiving discharge advice went from 7% to 70%. Compliance of doctors and nurses with the pathway was 63%.
Our previous audits showed substandard management of patients with chest injuries in our department. Through this quality improvement project, we were able to improve the quality of care provided to patients attending with rib fractures by increasing rate of analgesia received, regional blocks performed and discharge advice given.
- emergency department
- evidence-based medicine
- pain management
- quality improvement
- anaesthesia
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Morbidity from traumatic rib fractures in elderly patients is well recognised and development of multidisciplinary chest wall pathways in the emergency department (ED) has shown to reduce the rate of complications.
What this study adds
Implementation of a chest injury pathway has shown a reduction of time to analgesia, increased rate of documented analgesia and performance of regional anaesthetic blocks in our ED.
How this study might affect research, practice or policy
This study is an important addition to the expanding literature showing the benefits of multidisciplinary care pathways for patients presenting to the ED with chest injuries.
Problem
Rib fractures represent a substantial health burden. Around 20% of patients admitted after trauma will have at least one rib fracture. Chest injuries contribute to 25% of deaths after trauma and survivors can experience long-standing consequences, such as reduced functional capabilities and loss of work.1 The importance of early detection and aggressive management of rib fracture has been well described in the literature, especially in the older population.2 In the elderly, trauma to the thorax represents the second most common site of injury and mortality rates are two to five times higher compared with their younger counterparts.3 Poor pain management leads to hypoventilation, pneumonia and respiratory failure and is the main cause of morbidity and mortality in these patients. Each additional rib fracture increases the odds of mortality by 19% and of developing pneumonia by 27%.4 Early detection and aggressive pain management of these patients in the emergency department (ED) are important as even patients with initial normal respiratory status can develop complications up to 72 hours later.5 The development of protocols in the ED for management of patients with chest wall injuries has been demonstrated elsewhere to reduce the incidence of pneumonia.6
The Mater Misericordiae University Hospital (MMUH) is a level 4 teaching hospital based in Dublin’s north inner city. It provides dedicated national services for spinal surgery and cardiothoracic surgery including heart and lung transplant, and it has been recently announced to become one of the major trauma centres for the country. The ED is an adult-only department in Dublin that has an annual attendance of around 80 000 patients, it is staffed by 8 whole time equivalent emergency medicine (EM) consultants, 19 registrars, 18 senior house officers and 2 interns. MMUH did not have a specific guideline and standardised method to manage patients presenting with blunt chest injuries in the ED. Our inspiration to improve patient care with this project started with an encounter with an elderly patient who presented to the ED with torso trauma from a simple fall. She was discharged from the ED and re-presented a few days later after having developed pneumonia, which resulted in a long and complicated inpatient admission.
Our aim was to standardise the management of patients presenting with blunt chest trauma to our ED by introducing a multidisciplinary care pathway; more specifically to increase the rate of documented analgesia from 39% to 100%, to increase the rate of regional anaesthetic blocks performed in the ED from 0% to 50% and to increase the rate of discharge advice given from 7% to 100% within 1 year.
Background
Pain associated with rib movement reduces tidal volume and predisposes to significant atelectasis, increasing the risk of pneumonia. Effective analgesia prevents hypoventilation, and enables deep breathing and adequate coughing with clearance of secretions.7
Most pathways use analgesic ladder advice for initial oral analgesia with paracetamol and non-steroidal antiinflammatories (NSAIDs) if not contraindicated, followed by weak opioids and strong opioids.
For admitted patients, patient-controlled analgesia is advised if pain remains uncontrolled.
Multiple guidelines suggest that hospitals receiving patients with major trauma should have written and agreed guidelines for management of patients with severe chest wall trauma that must include multidisciplinary care with anaesthetic, pain and physiotherapy teams.6 8
Trauma centres in both the UK and Ireland are now increasingly adopting multidisciplinary care pathways to help clinicians with decision tools for analgesic strategies, specialty input and disposition of patients with blunt chest injuries presenting to the ED.6 9–11 The role of point-of-care ultrasound and, specifically, the use of regional anaesthetic techniques as an opioid alternative in pain management is becoming widespread.12 13 We wanted to introduce the early use of serratus anterior plane block (SAPB) and erector spinae plane block (ESPB) for patients presenting with rib injuries as these are well known and safe alternatives to opioids.12
Regional anaesthesia in the form of paravertebral block, SAPB or ESPB can be considered depending on location of fractures, local availability and expertise. Both SAPB and ESPB use by EM physicians have been extensively described in the literature.13 14
Thoracic epidurals can be considered for bilateral rib fractures in patients without contraindications.
Chest radiographies (CXRs) are well recognised as having a very low sensitivity for rib fractures, with greater than 50% false negative rates. In a large registry, when patients were randomised between CXR only and CT of the thorax (CTT), up to 80% of injuries like pneumothorax, haemothorax and pulmonary contusion were occult and one-third of these required a major intervention in the ED, like a chest drain insertion.15
Most chest injury pathways would suggest a low threshold for CTT in the elderly but rather than having specific indications, they often leave it to the clinician’s discretion to decide when CT is indicated.
Multiple risk stratification systems have been described in the literature.16 The STUMBL score was selected as one most widely used in UK and Ireland EDs.17 It allows prediction of risk of morbidity and it has been used as a tool to help determine safe patient disposition. The score is made of five variables: age, number of rib fractures, use of anticoagulant, presence of chronic obstructive pulmonary disease and oxygen saturation.
Most information leaflets offered in other hospitals focused on smoking cessation, to ensure early activity and when to seek medical attention. The implementation of physiotherapy in the management of patients with major thoracic trauma is beneficial and results in improved outcomes such as reduction in mortality and rate of pneumonia.6 18
Measurement
We had five Specific, Measurable, Actionable, Realistic and Timely measures, three outcome measures and two process measures.
The outcome measures were (1) 100% patients to receive analgesia on arrival, (2) reduction of time to analgesia, (3) 50% of eligible patients to receive a fascial plane nerve block performed in the ED.
We found no supporting evidence on appropriate criteria for administration of a regional anaesthetic block. Our eligibility criterion for patients to receive a fascial plane nerve block was a score more than 11 on the STUMBL risk stratification system (see online supplemental material). This was similar to previously described pathways in the UK and Ireland.10 11
Supplemental material
The process measures were: (1) 100% discharged patients to receive information leaflets, and (2) 100% compliance of doctor and nurses with use of pathway.
Our rationale was that the main intervention for improving outcome is consistent and timely analgesia. The increase in the performance of fascial plane block was also a marker of this modality of analgesia becoming more standardised for this patient population. Given the improved outcomes from early physiotherapy shown in a previous study, we thought that the delivery of patient information leaflet for home physiotherapy advice would have been an important measure, particularly as physiotherapy is not available out of hours.
Our leaflet, developed in conjunction with our physiotherapy service, included general advice on expected time to recovery, avoidance of strenuous activity, when to seek medical advice, contact information and breathing exercises.
We planned to perform a baseline audit and then repeat collection of data on a monthly basis throughout the project. Microsoft Excel was used for data storage and analysis.
Our ED information system recorded the use of the pathway by the treating clinician or nurse when a patient with suspected rib injuries was assessed, allowing us to collect information on the compliance of doctors and nurses with the pathway. This helped to see if the changes in result were more likely secondary to the introduction of the pathway than due to other factors.
To collect data for the audits, patients were identified by searching their triage-presenting complaint and reviewing the treating clinician note if rib injury was considered.
As a baseline audit, between November 2019 and January 2020, we looked at how patients with chest injuries were managed in the MMUH ED at the mode of analgesia used, the use of scoring system for rib injuries and the final disposition. It demonstrated that in a total of 59 patients triaged as sustaining a torso injury, only 23 (39%) had documentation of analgesia received. Median time to analgesia was 1 hour and 35 min. No patients had documentation of a regional anaesthetic block being performed. There was no documentation of the use of a scoring system as this was not part of our management at the time. A total of 43 patients (73%) were discharged, but only 4 patients (7%) had documented written or verbal advice and explanation of red flags. One patient reattended and required admission following development of pneumonia.
Design
Our team was made of four EM consultants, three EM registrars and one EM nurse with specific interest in the development of the pathway.
We created a shared online document where we posted updates, records of meetings and next steps. Key points necessary for the pathway highlighted during the meeting were to ensure timely and standardised analgesia, to include criteria for ultrasound-guided fascial plane block in the ED and to develop a discharge information advice leaflet. These became part of our outcome and process measures. Another important point was to agree a criterion for CTT with our radiology colleagues, often left to the clinician’s discretion in previously documented pathways.
Relevant stakeholders were identified and engagement with them was made through email or via separate one-to-one in-person meetings. These included a radiology consultant with a special interest in trauma, a cardiothoracic surgeon, a pain consultant and a physiotherapist.
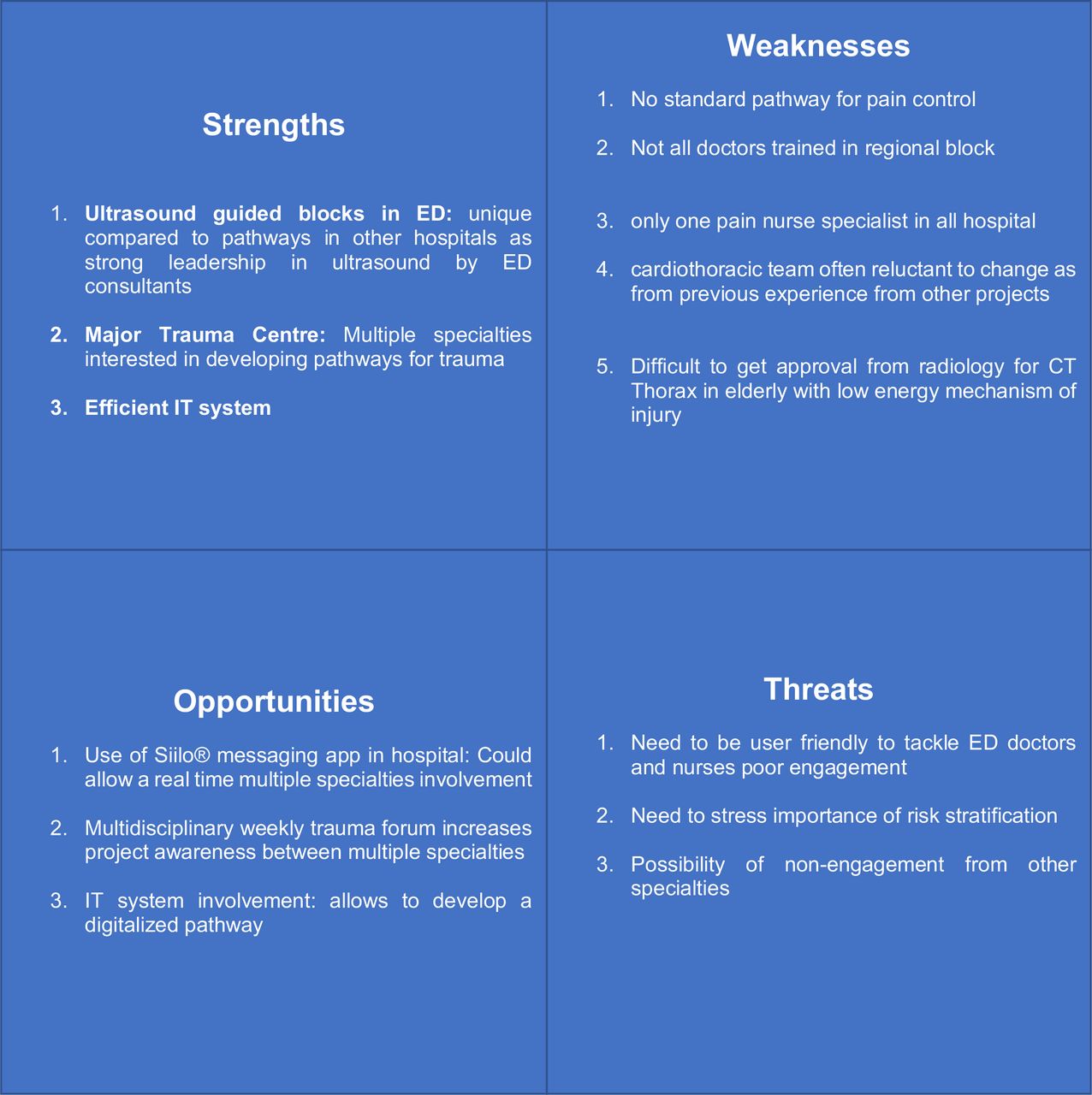
A Strenght, Weakness, Opportunity and Threat (SWOT) analysis was performed to analyse the problem (figure 1). It was clear that our department had unique strengths and opportunities that made the project particularly suitable. A clear strength was the expertise within our consultant group with the use of regional anaesthetic blocks in the ED, allowing our pathway to be unique in not having to rely on our anaesthetic colleagues. One of the initial challenges was that the thoracic surgery team and cardiac surgery team shared the same on-call rota for the ED resulting in variation in the level of interest in the group to be involved. One of the main threats was the potential loss of interest by specialties and EM doctors and nurses in using the pathway. This analysis helped to design a pathway that was tailored to our setting.

SWOT analysis. ED, emergency department; IT, information technology.
A process map helped to focus on where interventions were beneficial and where solutions could be found.
Triage was the first point where administration of analgesia happened, so here an intervention of educating nursing staff about the importance of early analgesia in this patient group was thought to be important.
After assessment by a physician, the patient had their severity of pain further evaluated and the chest injury score can be calculated to help standardise how the analgesic strategy should be. At this point, patients would receive a regional fascial plane block if not contraindicated. Lack of operator experience with the procedure and poor acknowledgement of the importance of pain relief in chest injury were considered major limitations for this step. For both, education of staff and increasing awareness were used as interventions.
Disposition was another area where there was poor documentation of discharge advice given so the development of a patient information leaflet was deemed necessary.
Strategy
We used the Plan–Do–Study–Act (PDSA) cycles from the Institute of Healthcare Improvement as a framework.
PDSA cycle 1: team formation and first draft of the pathway
The first PDSA cycle was performed during the month of March 2021. After the first meeting, analysis of the problem, formation of a team and engagement of the stakeholders, an initial draft of the pathway was developed, including a patient information leaflet. Our aim was to test our initial pathway to see if it would have improved outcome and to gather feedback from the healthcare staff. The ED medical and nursing staff were informed through a departmental educational session about the implementation of the pathway. We then analysed our results for the following months and compared them with our PDSA cycles data.
PDSA cycle 2: development of the pathway and introduction in the ED Information system
The second PDSA cycle was performed in the month of April 2021. We gathered feedback from the initial pathway and agreed a final version between our team members and the stakeholders. We found that one of the barriers was access to the pathway by doctors and nurses in ED. To tackle this, we engaged with our information technology (IT) staff and incorporated the pathway into our ED information system so it could be opened in a patient’s episode. We also led a departmental teaching session with doctors and nurses to advertise its use. We hoped that easier availability would improve utilisation of the pathway.
PDSA cycle 3: hospital and trauma group education
On 26 May (week 11), we presented the pathway to the hospital trauma group. This gave us the opportunity to introduce it to a wider hospital audience with shared interest in trauma and increased the awareness of the topic. By involving not only ED doctors and nurses but also other hospital doctors, nurses, advanced nurse practitioners and allied healthcare staff, we hoped to increase compliance with the pathway.
PDSA cycle 4: regional anaesthetic block education
The last PDSA cycle was performed in June 2021.
By gathering further feedback from doctors, it seemed that more teaching to senior ED staff could have increased the rate of fascial blocks performed. In-person ultrasound teaching had to be halted due to the COVID-19 restrictions and at this time it was deemed safe to restart. A practical teaching session for use of SAPB and ESPB in the ED was organised. Our aim was to increase the performance of regional plane blocks in the ED.
Also, the clinical nurse facilitator pointed that nursing staff had no access to the pathway in the information system. As a result of this, we asked the IT staff to make the pathway available to nurses and led a dedicated teaching session on its use.
Results
The results from the PDSA cycles are plotted in the run charts (figures 2 and 3).

Run chart, analgesia received and discharge advice given (%). Dotted lines indicate overall trends. PDSA, Plan–Do–Study–Act.
{kind=link}
{kind=link}
{kind=link}
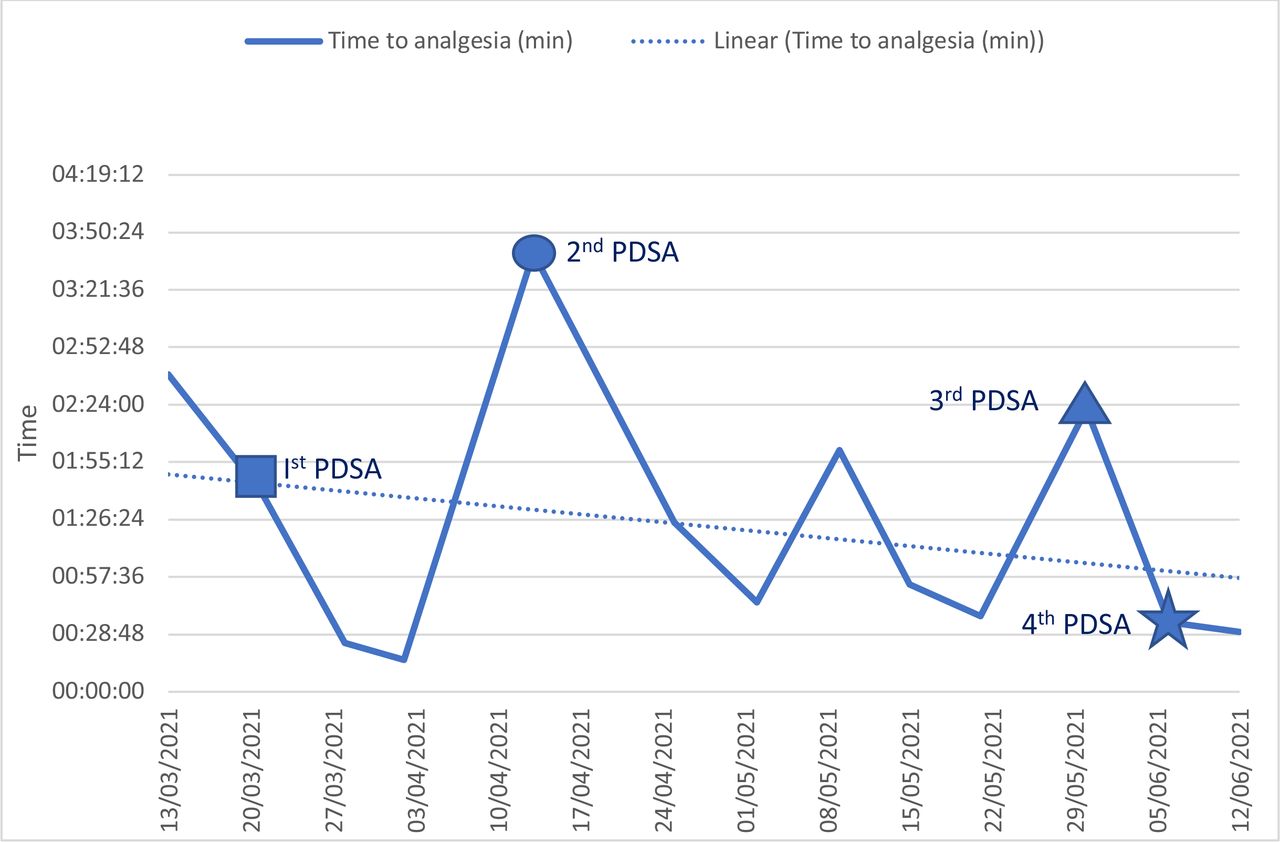
Run chart, time to analgesia (min). Dotted line indicates overall trend. PDSA, Plan–Do–Study–Act.
Prior to the first cycle, the baseline documented number of patients been given analgesia was only 39% and median time to analgesia was around 2 hours and 40 min. Documentation of specific chest injury discharge advice occurred in 14%.
In the first PDSA cycle, after the introduction of the first draft of the pathway, there was a marginal improvement in the proportion of patients receiving analgesia (from 39% to 44%) and a reduction of median time to analgesia. Also, there was an increase to 20% in documentation of patient information leaflet and of advice given to patients. There was no increase in the number of fascial plane blocks performed in the ED even though five patients had a total risk stratification score of more than 11, indicating a need for regional anaesthesia as per our protocol.
The second PDSA cycle had a low percentage of patients documented as receiving analgesia (40%) and a sharp increase in median time to analgesia above 3 hours. The percentage of patients receiving discharge leaflets went up to 100% and quickly dropped down the following week to 30%. Still, there was no block performed in three patients where it was indicated.
During the third PDSA cycle, there was again a slight improvement in documented analgesia administered (from 50% to 75%), even though it was still below the predetermined target of 100% and a decrease in time to analgesia to a median of 30 min. Three blocks were performed in a total of seven patients where it was indicated (43%). The discharge advice given was below the target (50%).
At the end of the fourth and last PDSA cycle, there was an increase in the rate of regional blocks performed in the ED, going from 43% to 60% of patients who met inclusion criteria, reaching the predefined target. Time to analgesia and discharge advice showed some improvement while the analgesia received remained grossly unchanged.
The percentage of patients with documented analgesia went from 39% to 70% and the median time to analgesia went from 2 hours and 40 min to 28 min. The percentage of patients receiving discharge advice went from 7% to 70%. Fascial blocks performed went from 0% to 60%. The compliance of doctors with the pathway rose from 25% in the month of May to 63% in the month of June, suggesting an overall improvement.
Lessons and limitations
As a result of this project, a multidisciplinary departmental pathway for patients with blunt chest injuries was developed. This standardised the level of care provided to the best available evidence, with significant improvement in the management of these patients. This was the primary aim.
Because of the restrictions put in place by the hospital infection control staff due to the COVID-19 pandemic, in-person interdisciplinary meetings were not allowed, so bringing many different specialists to a final agreement made the task very challenging.
Another challenge due to the restrictions was that departmental ultrasound training was not possible because it would have entailed large gatherings in an enclosed space, so this caused a delay in providing teaching sessions for ultrasound blocks in the ED. The restrictions could have brought some opportunities: team members were meeting with virtual platforms, and this might have facilitated attendance and possibly made some decision quicker than with in-person meetings.
Each PDSA cycle brought improvement in outcome and process measures, with a trend towards increase in analgesia, block performed, discharge advice and a reduction in median time to analgesia. Interventions were mainly aimed at educating doctors and nurses and facilitating the use of the pathway. Compliance rose consistently.
Throughout the project, only the original target of 50% of blocks performed in ED when indicated was achieved, while the targets of 100% patients receiving analgesia and discharge advice were not met. On reflection, these aims might have been too ambitious and if we were to repeat this quality improvement project (QIP), we would probably consider using lower targets. ED crowding, time of the day and workforce could also have been contributing factors to not having reached the targets, but these data were not analysed. Also, there was substantial variation of the numbers of patients presenting throughout the different months during each cycle and this could also have had an impact on the final result.
It took a few months for EM doctors to use regional anaesthetic blocks more regularly in patients with blunt chest injuries. This is understandable, as an introduction of a new procedure takes time. Although the pathway brought an increase in the number of patients who received regional anaesthetic blocks, it will take time for this to become more embedded in routine practice.
We hope that the introduction of this pathway will increase the routine performance of these regional anaesthetic blocks by other doctors in the future and become part of standard practice.
The increasing pathway used by doctors and nurses was reassuring and indicative of engagement of staff with the project.
Future developments of the pathway could be the introduction of physiotherapists in the ED as part of a comprehensive multidisciplinary team for patients with rib injuries, as this has shown substantial benefit from previous literature. Currently, their role in the ED is limited to the care of patients with frailty but as the hospital transitions towards becoming one of the national trauma centres, we hope that their role will expand into delivering care to this cohort of patients as well.
This QIP has some limitations. The information system allowed only to search words in triage notes and not in doctors’ notes, so it was only possible to collect data of patients where the triage nurse suspected a blunt thoracic injury. Another limitation is that the measures used in our study were surrogate outcomes and did not measure reduction of morbidity or mortality in these patients. An alternative more robust outcome measure could have been reduction in reattendance rate due to complications (pneumonia, haemothorax) following introduction of the pathway. This would have required a larger collection of data before and after the intervention that was too complex to obtain within our target time frame, so it was decided not to pursue this.
Similarly, measurement of pain scores before and after introduction of the pathway and before and after administration of a nerve block was considered; however, within the current resource availability, it was not possible to do so.
Finally, public and patient involvement could have also been considered as one of the outcome measures through surveys or questionnaires as it would have brought a unique patient-centred insight into the development of this pathway, although this was considered difficult to perform during the COVID-19 pandemic.
Conclusion
In summary, implementing a multidisciplinary chest injury pathway for patients presenting to our ED brought an important improvement in process and outcome measures. We believe that this improved the quality of care of patients with rib injuries. Further auditing will be needed to ensure consistency in the use of the pathway and to identify potential future improvements.
To ensure sustainability, a dedicated clinical lead for the project is delegated by the department audit lead every year.
Quality improvement never ends. These data offered only a snapshot and as such will need to be constantly reviewed in the future.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
According to the Health Service Executive policy, ethical approval for quality improvement projects was not required.
Acknowledgments
The authors would like to acknowledge all the doctors, staff nurses and allied health professionals of the Mater Misericordiae University Hospital for their support, in particular Dr Leeza Little and Dr Mohammed Qotb for their contribution to the literature research and valuable insight.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CDV and TB both conceived and designed the study. CDV is guarantor of the study. CDV performed and collected data from audits, assembled a team, contacted and liaised with stakeholders, analysed the final data and drafted the first manuscript. CMD, FO'K and VR contributed to the design of the pathway. All authors contributed to the revision and final approval of the manuscript. Both CDV and TB accept full responsbility for the overall work and conduct of the study
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.