Article Text

Abstract
Crowding and boarding are common issues facing emergency departments (EDs) in the USA. These issues have negative effects on efficiency, patient care, satisfaction and healthcare team well-being. Data from an audit of the admissions process at a large, urban, academic US ED demonstrated a lengthy process, exceeding national benchmarks in both length of stay and boarding of admitted patients.
We performed a pre–post study between July 2019 and July 2021 focused on the first step of the admission process at our institution, the time to bed request. All patients admitted to an internal medicine (IM) floor team from the ED were included in the study. The primary outcome was the time from decision to admit by the emergency medicine physician to placement of the bed request order by the IM physician. Quality improvement (QI) occurred in three phases: an initial preintervention process and electronic health record change to better capture admission times, a primary intervention focused on process change and provider education and a second intervention focused on improvements to provider communication.
During the study period, 25 183 patients were admitted to IM floor teams and met inclusion criteria. Prior to the primary intervention, the mean time from ED decision to admit to IM placement of the bed request order was 75.1 min. Postintervention, the mean time decreased to 39.7 min, a statistically significant improvement of 35.4 min (p value <0.0001).
This QI project demonstrates the ability of interventions to reduce the time to admission bed request order, a key step in the overall admission process and a contributor to boarding at our institution. In making process changes, the team also reduced provider handoffs and improved provider communication.
- Emergency department
- Hospital medicine
- Length of Stay
- Quality improvement
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Studies have demonstrated that rapid admission protocols can reduce emergency department (ED) length of stay and boarding.
WHAT THIS STUDY ADDS
This study focused on the handoff and transfer of care between the ED and internal medicine hospitalists.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The study illustrates that process and systems changes coupled with education and improved reporting can result in sustained improvement.
Problem
Admitting patients from the emergency department (ED) to the internal medicine (IM) floor teams at our institution is a lengthy process composed of multiple steps with different stakeholders. This likely contributes to the institution underperforming benchmarks in both length of stay and boarding times. Length of stay for admitted patients exceeded the 2020 Emergency Department Benchmarking Alliance (EDBA) 50% benchmark by 72 min for similarly sized EDs (institution 473 min, EDBA benchmark 401 min).1 Furthermore, boarding time exceeded the EDBA 50% benchmark by 44 min (institution 202 min, EDBA benchmark 158 min).
Several definitions for ED boarding exist. For the purposes of this project, we have adopted the standard definition used in the USA, that boarding starts at the time of decision to admit and ends at departure.2 3
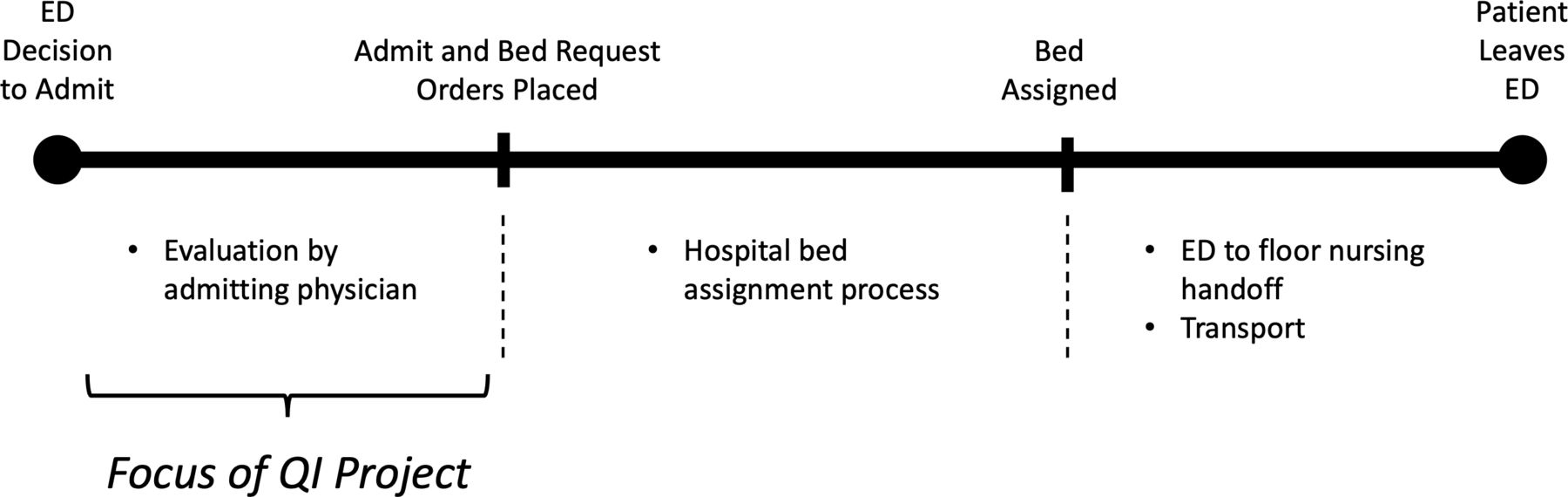
The admission process at our institution has three major steps (figure 1). The first step, and the subject of this quality improvement project, starts when an ED provider decides to admit a patient and requests admission from IM. This process step ends with IM placing admission and bed request orders.

ED to floor admission process. ED, emergency department; QI, quality improvement.
Prior to the intervention described further, ED providers had requested admission via a numeric page sent to a central IM physician. The IM physician would return the page with a phone call, discuss admission details with the ED provider, then accept or reject the admission. Accepted admissions would be assigned to members of a rotating pool of IM physicians who would evaluate the patient and ultimately place admission orders. An initial process audit identified the lack of reliable data as a primary obstacle for quality improvement. Specifically, the manual paging process did not generate a systematically captured timestamp for the ED decision to admit (time of ED request to admit). The first improvement cycle aimed to modify the process and systems to collect this important data point.
Aided by the newly captured data outlined previously, the team discovered that, on average, 43% of the time IM-admitted patients spent in the ED could be considered boarding (occurring after the ED provider’s decision to admit). Over one-third of that time (77 min or 16% of total time in the ED) occurred after an ED decision to admit but before IM admission and bed request orders had been placed. The primary intervention aimed to decrease overall IM admission process time by reducing the mean time from ED admission request to IM bed request order from 77 to 30 min.
Background
Our organisation’s struggle with ED crowding and boarding are not unique. While the national ED census dipped during 2020, the initial year of the COVID-19 pandemic, that trend has subsequently reversed, exacerbating factors associated with crowding, including increasing acuity, percentage of patients being admitted, length of stay and boarding times.1 4 These findings are consistent with the reported experience of emergency physicians that ED boarding and crowding has continued to intensify over the years of the pandemic.5 6 This crowding is problematic due to its negative effects on patient care, patient satisfaction and well-being of the healthcare team.7–16
Over the last three decades, multiple studies have both investigated the causes of ED crowding and suggested potential solutions; these focus on one of the three major determinants of crowding, including input, throughput and output of patients. Of these, sluggish output of patients to inpatient beds (also known as ‘inpatient access block’) is widely recognised to be the largest contributing factor to ED crowding.7 16–19 A variety of tactics to improve ED output have been studied, including structural changes such as smoothing surgical operating schedules, mandating the use of inpatient hallway beds for boarding patients and providing consistent ancillary services during weekends and off-hours. Less resource intensive changes have also been studied, including active bed management and prioritising early discharges.5 7 17 The persistence of crowding despite these well-understood causes and proposed solutions demonstrates a need for continued strategies to relieve access block, particularly using strategies with low-resource costs. To our knowledge, few studies have been undertaken to speed the process for transfer of care from ED to inpatient teams. Though those studies have shown potential improvements in ED length of stay (LOS), time to admission orders and ED boarding time.20 21 The efforts described here were an attempt to expedite these processes, which represent a limited component of the access block problem over which clinicians can exert direct control.
Measurement
The first improvement cycle of this project focused on implementing a new admission request order through Epic (Epic Systems Corporation), our EHR, with associated process changes to enable systematic capture of the time of ED decision to admit. As such, no reliable baseline data existed prior to this improvement.
Baseline data for a detailed process audit were collected via retrospective data extraction from the health system EHR. All patients seen in the ED during a 6-month period (1 January 2019–30 June 2019) and ultimately admitted to IM were included in the baseline. The baseline included 6451 patients who met the inclusion criteria. Of these patients, less than 2% (126) were excluded due to errors in data captured in the EHR. These included missing time stamps and/or negative durations. The major outcome variable for this quality improvement study was time to bed request order (IM bed request order timestamp – ED request to admit order timestamp). Additional patient and encounter data were collected, specifically age, gender, ED acuity (Emergency Severity Index) and hour of presentation to the ED.
A detailed analysis of this dataset demonstrated 16% of total time in the ED (77 min) occurred after the ED decision to admit but before admission and bed request orders had been placed by IM.
Design
The design of this QI project relied on a three-part approach:
Improve process-related data collection.
Undertake detailed process analysis and identify opportunities for improvement.
Implement resultant process, systems and people changes.
The QI team consisted primarily of physician stakeholders from the EM and IM departments and included experts in systems/EMR and operations. This project enjoyed support from departmental leadership at the highest level. The two departments partnered on the initial EHR-related step. The ED team led the subsequent data collection, process audit and analysis. Finally, IM led the implementation of process, education and reporting changes.
The implementation team met on an ad hoc basis throughout the project to monitor results and plan the next steps.
Strategy
Our goal with this QI project was to reduce the time to bed request order. To do so, we undertook three intervention cycles.
Preintervention improvement
Our initial process change was primarily designed to capture the time of ED admission in our EHR. This timestamp allowed detailed process analysis to drive subsequent interventions. This change was realised via a new EHR order with an associated system-logged timestamp. This new order automatically triggered a page to the central IM physician that included standardised information including patient information, ordering EM provider name and provider phone number. The inclusion of this standardised information represents the second process-related improvement within this intervention. Its intent was to improve challenges ED and IM providers shared in connecting to one another to discuss a requested admission, as well as to facilitate more efficient handoffs by giving IM providers basic information about the patient in advance of the handoff conversation with the EM team.
Intervention 1
Analysis of data made possible by the change described previously demonstrated a lengthy admission process, in particular, the time to IM bed request order. Interestingly, there was wide variability among IM physicians in their efficiency in placing bed request orders. The fastest quartile was 77 min faster in placing the bed request order than the slowest quartile. This implied the possibility of sharing best practices between quartiles and other potential training-related efficiency gains. There was also variability between our academic IM services (those with residents) and private IM services (those without). Academic services took on average 13 min longer to place the bed request order.
Admitting providers shared feedback that they were not prioritising placing the admit and bed request orders early, preferring instead to interview and examine patient before completing admit and bed request orders in a batch along with all the other orders needed to provide care for the patient. Prior to our intervention, there was no clear standard or goal for placement of these orders, and no monitoring, sharing or incentivising performance.
As a result, for the first intervention, our team focused on provider education and performance tracking. IM leadership reviewed the process, obtained feedback from the admitting teams and then established a target goal. Through mandatory meetings and educational materials, all hospitalists trained on the changes. The Plan-Do-Study-Act (PDSA) cycle identified opportunities to simplify the process. The team made process changes to reduce information handoff among IM providers. After this intervention, the central IM physician would quickly chart review the proposed admission to ensure no contraindication for admission to IM, and then assign to a second IM physician (without discussion with the ED provider) who would examine and admit the patient in addition to first calling the ED provider to receive patient handoff/checkout. Examples of contraindications included patients owned by a different service and patients unstable for floor admission.
Intervention 2
Based on provider feedback, for our final intervention, we focused on better closing the communication loop between EM and IM providers. Specifically, after the central IM physician received an admission page, he or she would now message both the requesting EM provider and second (admitting) IM physician via a system that enabled Health Insurance Portability and Accountability Act- (HIPAA-) compliant encrypted group messaging (Voalte Messenger, Hill-Rom Holdings). This message would include the names of each provider and facilitate easier communication/follow-up in the event of a delay or missed phone call. By including the IM triage physician, admitting hospitalist and EM provider in a group text, this facilitated closed-loop communication among them that the admit request had been received and assigned, as well as opening an additional channel for communication about the patient. These benefits were widely viewed as being worth the extra effort for the triage provider.
Results
The primary outcome variable for this QI project was time to bed request order (ie, the time elapsed between the initial ED request to admit order timestamp and the subsequent IM bed request order timestamp). This variable was measured at the patient encounter level and averaged for each period of interest.
Preintervention process changes enabled systematic capture of time of ED request for admission in the EMR. Therefore, prior to these changes, we could not measure our variable of interest.
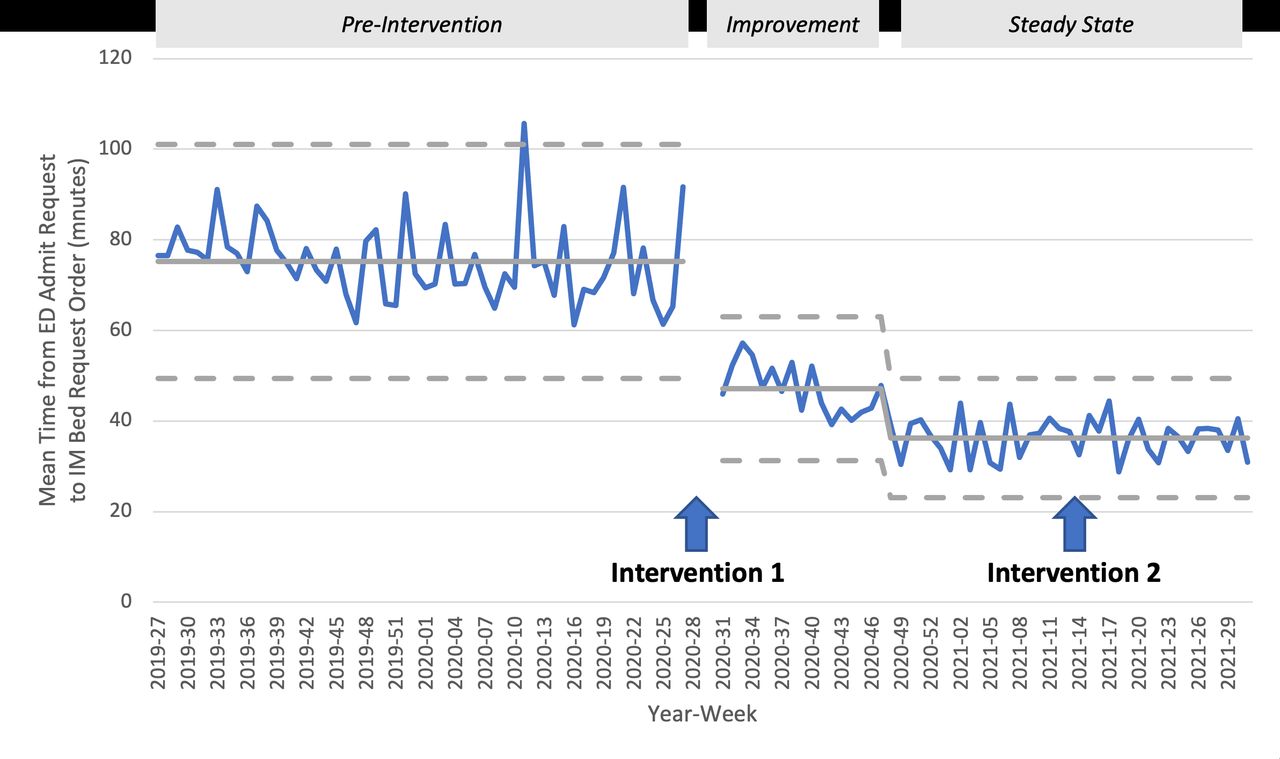
Intervention 1 represented our largest intervention and was conducted during July 2020. One year of data both preintervention and postintervention 1 was collected and analysed for this manuscript. A total of 13 263 encounters occurred preintervention and 11 920 encounters postintervention. The primary outcome variable (mean) decreased from 75.1 min preintervention to 39.7 min postintervention, a statistically significant improvement of 35.4 min (p value <0.0001) (figure 2).
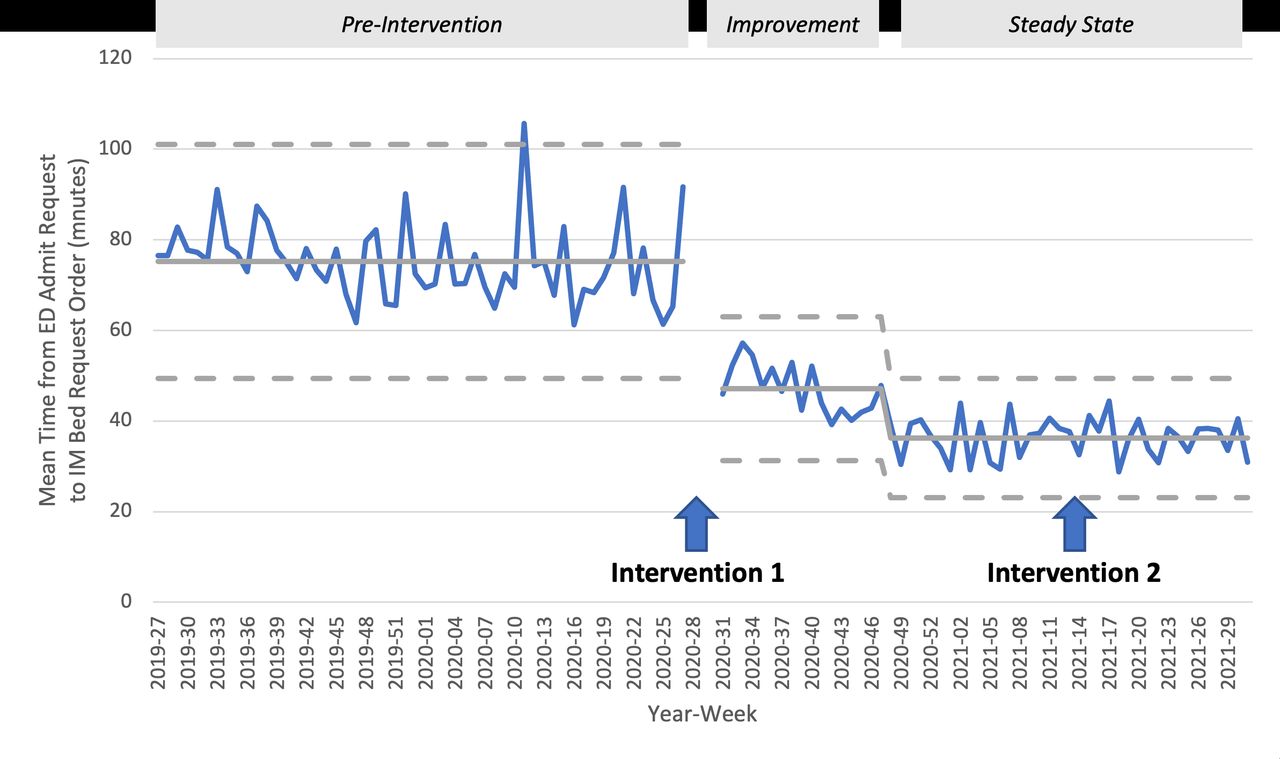
Control chart, time from ED admission request to IM bed request order, July 2019–July 2021. ED, emergency department; IM, internal medicine.
Based on the control chart, the postintervention 1 period appeared to have two distinct phases: an ‘improvement’ phase with a mean of 47.2 min and relatively wider control limits and a ‘steady state’ period with a mean of 36.3 min and relatively narrower control limits.
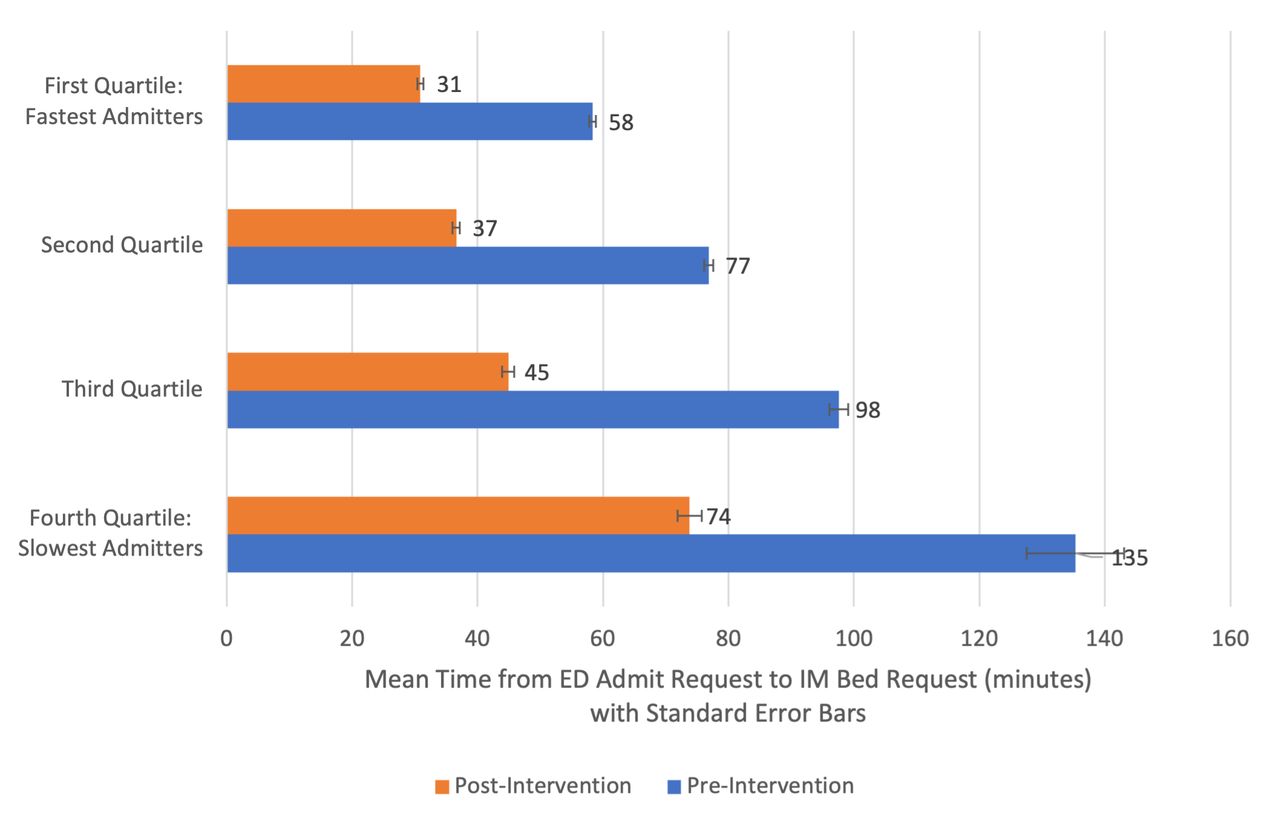
Subanalysis of IM admitting physicians demonstrated that all quartiles demonstrated statistically significant improvement (p value <0.0001) and that the slowest admitters improved by larger absolute amount. Interestingly, all admitters improved by approximately the same relative amount (45%–54% improvement) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Time from ED admission request to IM bed request order by quartile, July 2019–July 2021. ED, emergency department; IM, internal medicine.
Likewise, subanalysis of IM admitting physicians by service type demonstrated that both service types demonstrated statistically significant improvement (p value <0.0001) with near-identical mean absolute improvements of 35.7 min. Interestingly, the mean difference in admitting performance between academic and private services was 13.2 min both before and after intervention 1. This number appears to represent the efficiency cost of residents performing admissions at our academic institution.
Intervention 2 represented a small intervention and occurred on 1 April 2021. While this intervention improved communication between EM and IM physicians, the control chart demonstrated no obvious change in primary outcome variable.
Lessons and limitations
The project aim was to improve the time to admission for ED patients at the handoff point between EM and IM. As such, partnership was a necessary key to success. Role definition and delineation within this multidisciplinary team was equally important. Boarding of admitted patients affects the ED more directly than IM. As a result, the EM team played the larger role in the initial data collection, process audit and analysis necessary to develop the problem statement. In addition, the EM team developed an initial set of high-level recommendations. As the organisation responsible for the hospitalists who place the admission and bed request orders, the IM team played the larger role in development of detailed recommendations as well as the implementation of these process, education and reporting changes. The collaboration between EM and IM partners on this project provided valuable insights into efficiency and how communication and care quality could be enhanced by careful design and implementation of our interventions. Our work, including timely support from our informatics team, was supported at the highest level by senior health system and departmental leadership committed to driving change.
This project reaffirmed the management adage, ‘if you can't measure it, you can't improve it’. Prior to the initial process and EMR changes, the organisation did not accurately capture the time of ED decision to admit. This lack of data prevented the ED from measuring the time to bed request order. The success of this project required an initial systems change to track and measure this data. This was foundational, providing justification for the subsequent interventions that delivered measurable process improvement.
Furthermore, the success of this QI project rested largely in convincing individual providers to change their behaviour, which can be exceedingly difficult. This team felt that our success in doing so rested first on explaining the reason for change. This required providing hard data to illustrate an opportunity, but also concretely demonstrating why change matters to the patient and the organisation. Second, the team felt that transparency in performance was necessary to motivate individual change. Specifically, the team provided data to individual hospitalists showing them how they compare with their peers and continues to share individual and group performance as part of the monthly scorecard. This scorecard includes their personal performance, average department performance and the departmental goal of 30 min. As new providers are hired, these detailed are covered both during their orientation and prior to their first shift. IM leadership monitors individual and group performance. These factors have all helped to sustain this improvement over time.
Having separate bed request and care orders enabled much of the improvement realised in this project. At our organisation, IM hospitalists place both the bed request and patient care orders. Postintervention, in many cases, hospitalists placed the bed request order immediately after speaking with their emergency medicine colleague, allowing the hospital bed placement team to work in parallel with the hospitalist who then interviews and examines the patient before placing care orders. This parallel processing and quicker bed placement contributed to the throughput gains described in this paper but in rare situations resulted in the need to resubmit a bed request when patients needed a higher (or lower) level of care at the time the patient was examined by the hospitalist. Though not measured directly in this study, this circumstance was rare.
The project demonstrates that interventions initially conceived to improve easily measured process metrics also provide opportunities for unmeasured positive impacts on patient safety. This project focused on the time to bed request order. In making process changes to deliver improvement in this metric, the team also made changes to reduce the number of provider handoffs by changing the process to have admitting hospitalists contact the admitting ED physician directly, rather than through a centralised attending on duty. In addition, the team improved provider communication by implementing a system-generated page to IM that included more consistent, richer information than the previous free-form and typically numeric-only pages. Furthermore, after positive feedback and constructive suggestions from ED and hospitalist providers, communication via a closed-loop group message was introduced as our third intervention. These changes to reduce handoffs and improve provider communication no doubt contributed to increased patient safety and were well received by our providers.
In terms of limitations, this project resulted in a significant reduction in the time to bed request order. However, while IM is the largest admitter from our ED, they only account for approximately 60% of our ED admission volume. Additional interventions will need to be designed and implemented to apply to other services to maximise potential benefits from this type of intervention, though this project does provide a roadmap for success.
Due to competing organisational priorities, this project suffered a lengthy delay prior to intervention 1. In addition, while the initial process audit and data analysis was completed prior to the COVID-19 pandemic, the major interventions (interventions 1 and 2) occurred during the changing phases of the pandemic with unknown effects on project outcomes. The institution experienced significant swings in ED patient arrivals and hospital census, a significant confounder in measuring this project’s effect on LOS and boarding times.
This project focused primarily on reducing the time to bed request and admission orders. We cannot know whether this pressure to admit quickly changes the quality of care provided by admitting hospitalists or whether this pressure changes the quality of resident–faculty and student–faculty education on the admitting teams.
This QI project focused on improving the time from decision to admit to placement of a bed request. At our institution, these steps are completed by different physicians. EM drives the initial decision to admit while IM ultimately places the bed request. At other institutions, EM both initiates the decision to admit and enters the bed request order, limiting the generalisability to all hospitals.
Finally, this was a single academic centre, before–after study with specific improvements enabled by our EHR and secure group messaging platform which may also limit generalisability.
Conclusion
Through three improvement cycles, the multidisciplinary project team was able to reduce the time to admission bed request order, a key step in the overall admission process. In making process changes, the team also reduced provider handoffs and improved provider communication. To sustain this improvement, the team added admission process cycle time to individual monthly performance scorecards, with tracking of trends and comparison with the entire group. As a result, this improvement has already been sustained for 12 months. While IM admissions comprise most admissions from the ED at our institution, other services account for a material number of admissions. This project can serve as a framework for similar improvements within our institution (and beyond). At our institution, further work is being done to extend these results to the next most frequent ED admission service, family medicine.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors BI performed the initial data gathering and preliminary analysis. AP and MP designed and oversaw the interventions. NN provided comprehensive statistical analysis. BI drafted the manuscript, and all authors contributed substantially to its revision. BI takes responsibility for the manuscript as a whole.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.