Article Text

Abstract
Introduction Operating room (OR) management plays a pivotal role in the healthcare system due to the high cash flow it yields. Enhancing communication in the OR, which is the common root problem for delays, might improve OR efficiency and revenues for healthcare. This study aims to evaluate the impact of an OR relay strategy on turnover time (TOT).
Methods A quality improvement project was conducted. In the intervention group, a certified registered nurse anaesthetist (CRNA) remained outside of the OR, coordinating the steps to get the next patient ready. This CRNA communicated with the anaesthesia providers within the OR via a Microsoft Team chat. The TOT for the control group was recorded from the electronic anaesthesia record system.
Results/data analysis Analysis of 636 turnovers was performed with non-parametric tests. The OR relay strategy decreased TOT for most ORs, with statistically significant results for three of the ORs and the overall ORs system. A decreased in variability between TOTs was evidenced for the overall OR and the majority of the ORs evaluated individually.
Conclusion The OR relay strategy has a positive impact on TOT.
- Anaesthesia
- Efficiency, Organizational
- Information technology
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Most of the causes of delay in the operating room (OR) are associated with communication issues. Therefore, connecting the different stakeholders to improve communication might improve OR efficiency.
WHAT THIS STUDY ADDS
The relay strategy decreases the turnover time (TOT) in ORs with a baseline TOT above 40 min. However, there is a need to develop a software application to streamline efficient communication channels.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The relay strategy could aid in improving OR efficiency in academic centres with issues in TOT.
Introduction
Operating room (OR) management plays a pivotal role in the healthcare system due to the high cash flow it yields. OR operational cost varies between US$30–100 per minute, and the profit margin to hospitals is significant.1–3 The OR produces between 40% and 70% of total hospital revenue in most instances.2 4 This figure is partially explained by the fact that 40% of hospital admissions have surgical procedures.5 Therefore, initiatives to enhance OR efficiency are expected to have a financial impact on a hospital’s revenues.1 5
According to Little’s law, capacity is the maximum rate at which a process can generate an outcome, and improving the capacity would result in increased revenue only if there is enough demand for the additional output produced.6 In the OR, capacity could be defined as the maximum number of patients having surgery per day. Increasing OR capacity in the context of continuously rising surgical demand in the USA may translate into economic gains in healthcare.7 Maximising OR capacity by building more rooms is an inefficient strategy, whereas abolishing non-value-adding activities, although complex, is achievable. The goal is to find common ground between the different stakeholders to maximise the OR efficiency regardless of the conflicting priorities of a multidisciplinary system.5 8 Optimisation of OR capacity to match supply and demand will increase efficiency by either adding one more case per room or shortening the surgical schedule’s tail end. Consequently, this approach may improve revenues, cost of overtime staffing and employees’ satisfaction.9 10
The main reasons for OR inefficiency are improper patient or equipment preparation, surgeons’ unavailability, insufficient staff or room in the postanaesthesia care unit and delays in patient transportation.11 Most of these causes of delay in the OR have a common root problem: a communication issue. Therefore, connecting the different stakeholders to improve communication might improve OR efficiency.3
Different measurements of OR efficiency have been described in the literature; one of them is the turnover time (TOT), defined as the time lapse between a patient exiting the OR and the next patient entering the OR.12 13 This study aims to evaluate the impact of an OR relay strategy on the TOT.
Methods
This study has been reported according to the SQUIRE 2.0 guidelines.14 After approval by the Institutional Review Board (Protocol # 1847084), a quality improvement project with a quasi-experimental design was conducted to evaluate the effect of a relay strategy on OR efficiency. This study was conducted in an academic medical centre. TOT was collected from scheduled procedures in the main OR, which had 16 active rooms with scheduled cases when the study was in progress. The surgical services included in the study were otolaryngology, orthopaedic surgery, general surgery, urology, neurosurgery, ophthalmology, vascular surgery, gynaecology, breast surgery, plastic surgery and bariatric surgery. TOT for the control group was obtained from the electronic anaesthesia record system for scheduled procedures performed between June and July 2021. In the intervention group, a relay strategy was implemented in which a lead certified registered nurse anaesthetist (CRNA) was outside of the OR, coordinating the process activities necessary to get the next patient ready. This CRNA communicated bidirectionally with the anaesthesia providers within the OR via a Microsoft Teams software chat. The lead role was assigned to one CRNA for every four ORs included in the study. The sequential order of activities performed by the different stakeholders around the turnover period is illustrated in figure 1.
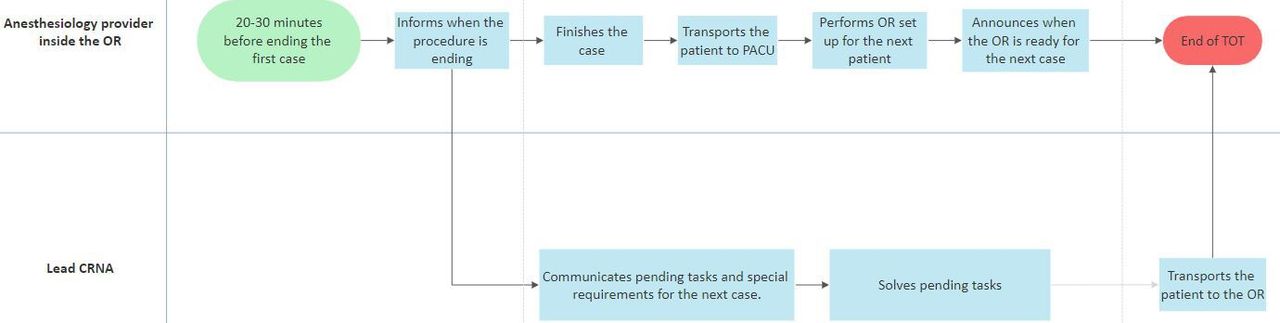
Process flow chart of the activities performed by the anesthesiology providers involved in the relay strategy. CRNA, Certified Registered Nurse Anesthetist; PACU, Post Anesthesia Care Unit; OR, operating room; TOT, Turnover time.
Statistical analysis
All statistical analyses were performed using JMP V.16.0.0 (SAS Institute Inc). The χ2 test was used to evaluate equal distribution of turnovers between the different ORs. Descriptive analysis was used to assess the median and IQR of TOT before and after the intervention. Distribution of TOT was evaluated with a histogram. A normal quantile plot and Shapiro-Wilk test were performed to assess for normality of observations. A logarithmic transformation was used to try to obtain a distribution close to normal. Due to the right-skewed distribution of TOT, Wilcoxon test was employed to make comparisons between groups. Before interpreting the data displayed in the non-parametric tests, a Levene test was performed to test for equal variances.
Patient and public involvement
No patients were involved in this study.
Results
A total of 636 turnovers were collected, 317 in the intervention group and 319 in the control group. The number of turnovers per OR was equally distributed between the intervention and control groups. Before the intervention, median TOT was 47 (30) min for the overall OR system. The frequency histogram for TOT displays a right-skewed distribution. After logarithmic transformation of the data, the skewness was reduced. However, the Shapiro-Wilk test and normal quantile plot demonstrated non-normality for the data.
Most of the ORs with a baseline TOT above the institutionally accepted threshold of 40 min exhibited a decrease in median TOT after the intervention (figure 2). The drop in TOT was statistically significant for the overall OR system and three ORs evaluated individually (p value<0.05). However, a decrease in variability between ORs was demonstrated by an F-test, showing a statistically significant difference in variance between the intervention and control groups (table 1).

Mean turnover time per OR in the control group and intervention group (Relay strategy). OR, operating room.
Descriptive analysis and non-parametric test for turnover time per OR
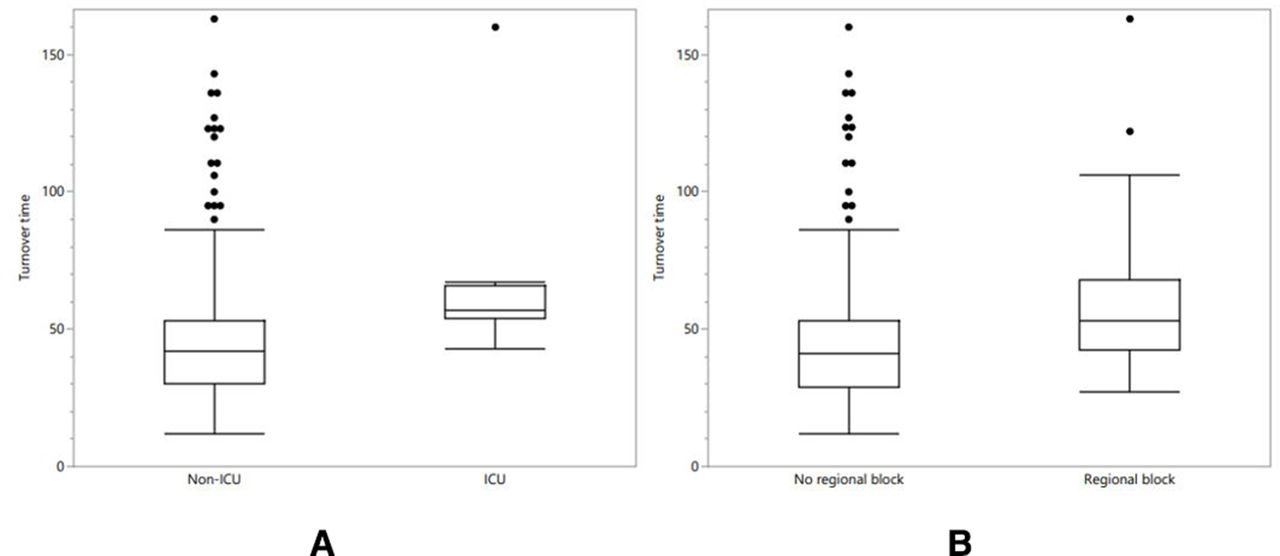
The factors that contributed to a higher TOT after the relay strategy were analysed with a Wilcoxon test. Patients coming from the Intensive Care Unit (ICU) and those requiring a regional block prior to surgery had a statistically significant higher TOT with a p value of 0.0002 and <0.0001, respectively. The box plot in figure 3 shows the increase in TOT for each of these groups.

{kind=link}
{kind=link}
{kind=link}
Box plot displays the distribution of the turnover time. (a) ICU patients. (b) patients requiring a regional block. ICU, Intensive Care Unit.
In the intervention group, the reason for the delay was reported in the Microsoft Teams chat by anaesthesia providers whenever it was encountered. The reason for the delay was reported in 152 turnovers. One-third of the delays were attributed to surgery-related causes. Within the surgical causes, pending tasks such as unsigned consent were the main culprits for the delay. Holding area and equipment-related delays accounted for another third of the reasons for higher TOT. The remaining delays were related to scheduling, patient-related causes, OR nurse delays and cleaning issues. The documented causes for delays encountered after the relay strategy are displayed in table 2.
Description of the delay causes in the intervention group
Discussion
The relay strategy positively impacted median TOT and IQR for overall OR system and individual ORs with a baseline TOT above the institutionally accepted threshold of 40 min. After the intervention, a significantly higher TOT was noticed in cases needing a regional block before surgery and in patients coming from the ICU. In this study, most stakeholders involved in OR processes were implicated in causes of delay. In addition, surgery-related issues were identified as the main reason for delay.
In our study, the reduction in TOT may not be sufficient to add another case to the daily schedule; however, it could positively impact revenue by reducing overtime staffing needs. Furthermore, decreasing the workload may positively affect workers’ satisfaction.9 10 In order for revenue to increase as a result of the relay strategy, the cost of a lead CRNA must be offset by other cost savings. In our study, the lead CRNA did not raise the expenses, given that the role was assigned to one of the floating CRNAs. These CRNAs in our institution are available for level one trauma cases, relief of anaesthesia residents for academic purposes and to give breaks to anaesthesia providers directly involved in patient care. The flexibility of these floating CRNAs allowed us to conduct the study without negative effects on OR coverage; however, future research should address cost-effectiveness of this strategy.
OR processes involve several stakeholders that contribute to OR inefficiencies. Hence, to decrease the delays in the OR, all of them must be involved to maximise the effect of interventions. Therefore, the sole involvement of anaesthesia providers in our relay strategy may have limited its impact.2 4 Although delays in the OR are multifactorial, poor communication is the root problem in several cases. Improvement of communication between different team members has been shown to decrease OR delays.3 Our findings are in agreement with previous studies, where surgeon availability accounted for a significant proportion of the delays. However, other causes of delay such as nursing and anaesthesia staff unavailability, unprepared patients, cleaning delays and congested holding areas were not as frequent in our study as compared with previous studies.11 15
In the healthcare industry, technology has helped deliver a better quality of care to patients by minimising the effect of human errors and assisting in improving process efficiency.3 16 17 Efficient and safe patient care delivery involves the coordination of several processes that happen simultaneously and in sequence. These multitude of activities are constantly generating data whose proper and timely analysis helps providers to develop and implement interventions aimed at improving the service offered and ultimately promote healthy patient-related outcomes. However, despite the availability of technology designed for this purpose, there is still a significant gap between data repositories and products of analysis that could lead to actionable insights.18–20 In this study, the use of Microsoft Teams software chat allowed to enhance communication in the OR, and it was a sustainable intervention. However, automated data collection possible and the format of the chat lent itself for communication of non-essential information that was sometimes redundant. Therefore, to enhance the impact of our intervention, we consider necessary the development of a software application to streamline efficient communication channels that improve team dynamics and generate data that can be transformed into knowledge through data analysis.
One major limitation of this study is the sample size. Even though we included 636 observations, the number of study cases was drastically reduced when we analysed each OR separately. Therefore, we consider that the drop in TOT was not significant for most of the individual ORs due to insufficient sample size per OR. The small sample size per OR is also related to the non-normal distribution of our response variable. We recognised that the normality assumption was not valid, even after a logarithmic transformation of the TOT. We used non-parametric tests for analysis. The scope of our study was not to determine the robustness of the non-parametric tests in our population; however, Monte Carlo simulations could have added value to our analysis as we might have been able to identify the validity under violation of underlying assumptions.21 Alternatives for analysis are generalised additive models for location, scale and shape and generalised linear models with extension to mixed models.22 23 In light of this limitation, we reported location and spread measures as median and IQRs. Additionally, the use of non-parametric tests is practical, and the results are still valid.
Furthermore, with the obtained data, we were not able to quantify the cost-effectiveness of our intervention. Another major limitation of our study is that the results cannot be extrapolated to other centres with different complexity levels and different types of surgeries or to non-academic centres.
This study focused on an intervention implemented for the general OR. However, each subspeciality has different turnover rates due to the length and complexity of the procedures. Consequently, further studies must be conducted to assess the effect of customised interventions directed to specific subspecialties. Likewise, future quality improvement projects need to focus on personalised interventions for patients requiring regional blocks before surgery and inpatients coming to the OR from the ICU, as we acknowledge that these circumstances may lead to prolonged TOT.
Conclusions
The relay strategy improves efficiency in rooms with a baseline TOT above the institutionally accepted threshold and decreases variability in each room and for the overall OR system. However, to maximise the effect of this strategy, we consider necessary the development of a software application to streamline efficient communication.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The Augusta University Committee B has determined this project does not meet the definition of human subject research under the purview of the IRB according to federal regulations 45CFR46.
References
Footnotes
Contributors RK, NL and AW contributed to the process of data collection and implementation of the relay strategy. BA-M and SK contributed to data analysis and article writing. ERP project coordinator. ERP project guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.