Article Text

Abstract
Background There is a need for expanded end-of-life (EOL) care education and resources for health professionals in acute hospitals to help them increase EOL care skills and knowledge, and build capacity and confidence to provide high-quality EOL care. End-of-Life Essentials (EOLE) is an Australian government-funded project, which offers free peer-reviewed online education modules and implementation resources on EOL care to health professionals in acute hospitals, aiming to help support the provision of high-quality EOL care.
Methods The development of EOLE education modules included seven major steps and two peer-review processes. In total, ten EOLE education modules and associated toolkits had been developed by the end of 2018. To evaluate the effectiveness of EOLE education modules, premodule and postmodule survey data from all ten modules and registration data were extracted from the EOLE learning management system for a 4-month period. The significance of difference in learners’ self-perceived EOL care knowledge, skills, attitude and confidence before and after module learning were tested by Wilcoxon Signed Ranks Tests.
Results Results from Wilcoxon Signed Ranks Tests revealed statistically significant improvement in learners’ self-perceived EOL care knowledge, skill, attitude and confidence after completion of EOLE modules regardless of their discipline (p<0.001). The learners from different disciplines also reported a high level of intention (median=4, IQR=1) to change their practice after completion of EOLE module learning.
Conclusion The evaluation results show a positive impact of EOLE module learning on allied health professionals, doctors and nurses, suggesting that EOLE could be a reliable and accessible online EOL care education resources for health professionals of all disciplines to improve their EOL care knowledge, skills and confidence, build up their capacities in providing quality EOL care to patients and their families, in turn, improve the quality and safety of EOL care in health settings.
- Education
- Palliative Care
- Continuing education, continuing professional development
- Healthcare quality improvement
- Health professions education
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Education
- Palliative Care
- Continuing education, continuing professional development
- Healthcare quality improvement
- Health professions education
WHAT IS ALREADY KNOWN ON THIS TOPIC
Health professionals of all disciplines in acute hospitals indicate the need to increase their end-of-life (EOL) care knowledge and skills. End-of-life Essentials (EOLE) module learning has a positive impact on health professionals; however, the effectiveness of EOLE education modules on each health professional group is unclear.
WHAT THIS STUDY ADDS
Allied health professionals, doctors and nurses all benefit from EOLE education modules.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
EOLE could be used as an online EOL care education resources for health professionals of all disciplines in acute hospitals and other health settings to improve the quality of EOL care.
Background
The Australian Commission on Safety and Quality in Health Care (ACSQHC) has highlighted that the quality and safety of end-of-life (EOL) care are imperative for the individual patient, their families and for EOL care providers.1 This has been reinforced via The Realistic Interpretation of Advance Directives (TRIAD) research studies undertaken by Mirarchi and Yealy in the emergency department in the USA and by Virdun et al in Australian hospitals, focused on improving EOL care.2 3 Most people in developed countries receive EOL care in acute hospitals4–7; however, gaps still exist in the quality of hospital-based EOL care, including insufficient communication, inability to recognise dying and interpret EOL care documents accurately.1 8 9 Healthcare professionals (HCPs) in acute hospitals indicate the need to increase EOL care skills and knowledge, including education and resources, which could support them to build capacity and confidence to provide high-quality EOL care.10–13
End-of-Life Essentials (EOLE) is an Australian government-funded project offering free peer-reviewed online education modules and implementation resources on EOL care to HCPs in acute hospitals. This project commenced in 2015, based on the ACSQHC National End-of-Life Consensus Statement.14 Between 2015 and 2020, 19 051 health professionals registered for EOLE, including 1481 doctors, 3658 allied health professionals and 13 912 nurses. Since then, 34 918 modules have been completed, with an average of 1.8 module completion for each learner. The aim of this paper is to evaluate the impact of EOLE education modules on EOL care knowledge, skills, attitudes and confidence of the HCPs that use the education.
Methods
Development of EOLE education modules
Ten EOLE education modules had been developed by the end of 2018 (see table 1), covering three main categories: (1) understanding death and dying; (2) clinical skills in EOL care such as recognising the end of life, patient-centred communication and shared decision-making, planning EOL care; and (3) EOL care with different patients such as patients living with chronic complex illness, paediatric patients and patients in emergency department.15
End-of-Life Essentials modules
The strengths of this project include: (1)the EOLE education modules and Implementation Toolkits were built around areas of knowledge gap identified in the ACSQHC’s National Consensus Statement: essential elements for safe and high-quality EOL care.14 (2) The rigorous process of education module development (see figure 1). From the inception of EOLE, quality, consultation and industry partnership have been paramount. A peer-review process was devised to ensure the quality and relevance of educational materials, and the quality of user experience was also an important focus. (3) Metacognition was employed as the underpinning framework for the education design, an approach encouraging learners to critically reflect on their practice.16 Studies showed that utilisation of metacognitive strategies in online learning environment may contribute to better learning engagement and performance.16 17
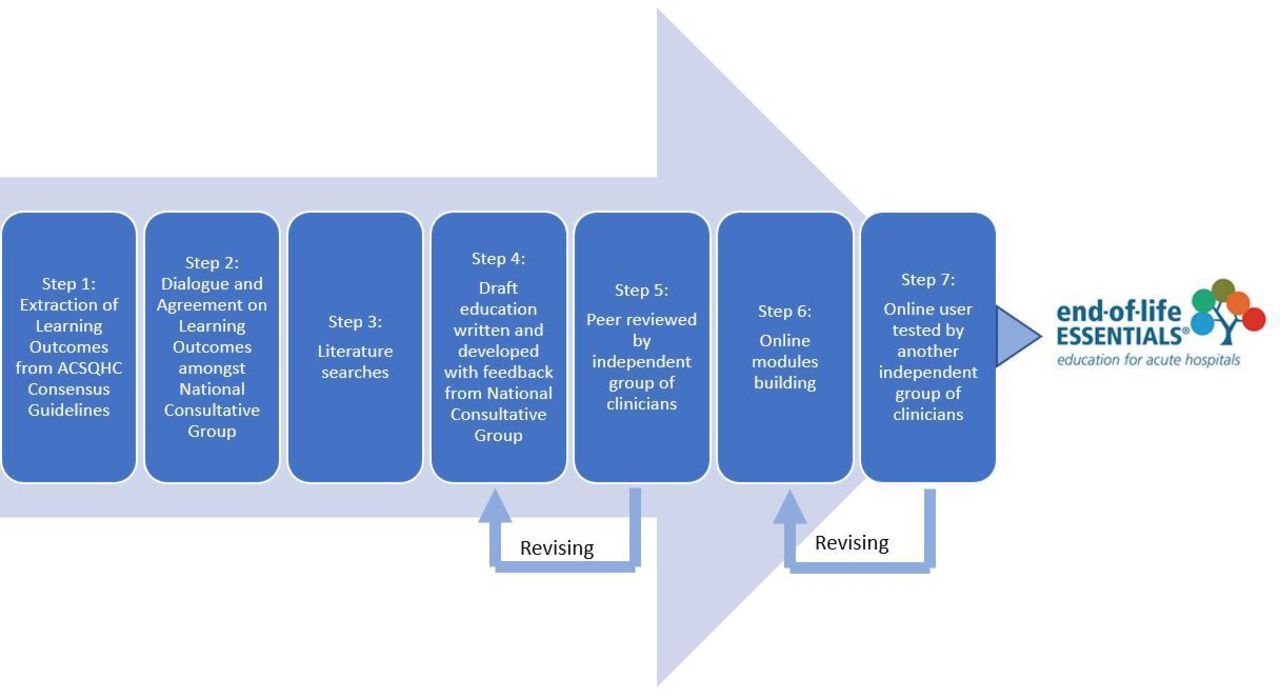
{kind=link}
Process of End-of-Life Essentials education modules development. ACSQHC, Australian Commission on Safety and Quality in Health Care.
Quizzes, videos and clinical practice-related open-ended questions were embedded in modules to prompt critical thinking and self-reflection, activities that are user friendly and easy to access. Downloadable Implementation Toolkits were developed to facilitate clinical practice change18; EOLE education modules also emphasise compassionate care (using scenarios for context), which is fundamental to EOL care19 and promotes HCPs self-care.
Evaluation of EOLE education modules
Ongoing EOLE module evaluation is embedded in a learning management system (LMS), including pre-evaluation/postevaluation surveys consistent across all modules and individualised free-text questions asking learners about their clinical practice.20 This multimethods approach allows breadth and depth of module evaluation.21 As the aim of this paper is to evaluate the changes of learners’ self-perceived EOL care knowledge, skills, attitude and confidence after completion of the modules, the pre-evaluation/postevaluation methods will be described.
The pre-evaluation and postevaluation questions were developed based on Kirkpatrick’s Model of evaluation,22 in which four levels of learning outcome were assessed, including: ‘(1) reaction, (2) learning, (3) behaviour and (4) results’.22 The pre-evaluation/postevaluation questions are specific to the context of each module (eg, pre: in thinking about providing EOL care for patients living with chronic complex illness/post: since completing this module, in thinking about providing EOL care for patients with chronic complex illness20).
In the pre–post evaluation, all modules include four identical statements about EOL care knowledge, skill, attitude and confidence. There is also a postevaluation statement “I intend to change my practice in end-of-life care”, aiming to explore the impact of EOLE module learning on learners’ intention to change their practice. Learners are asked to select ‘strongly disagree’, ‘disagree’, ‘neutral’, ‘agree’ or ‘strongly agree’ for each of the statements in a simple five-point Likert scale, with ‘1=strongly disagree’ and ‘5=strongly agree’.20
Data extraction
Premodule and postmodule survey data from all ten modules and registration data between 1 July 2020 and 2 November 2020 were extracted from the EOLE LMS. The date range for this data collection was pragmatically driven by the need for useful project knowledge linking the data with higher level decision-making processes in project organisation.23 All datasets were deidentified and imported into SPSS version 25.00 separately, then the premodule and postmodule data were merged into registration data using SPSS merge function with the key variable userID. In total, 2408 health professionals registered for EOLE from 1 July 2020 to 2 November 2020, of these 1946 learners completed at least one pre-evaluation/postevaluation question of the modules and were included for data analysis.
Data analysis
Data analyses were conducted using IBM SPSS V.25.00. The combined scores of self-perceived EOL care knowledge, skills, attitude, confidence and intention to change practice were calculated as average out of modules undertaken by learners (maximum 10 modules). The higher scores indicated higher level of self-perceived EOL care knowledge, skills, attitude, confidence and intention to practice change. A value of p<0.05 was considered statistically significant. Descriptive statistics were summarised as frequency with percentage for demographic variables. The significance of difference in learners’ self-perceived EOL care knowledge, skills, attitude and confidence before and after module learning were tested by Wilcoxon Signed Ranks Tests as data were not normally distributed, these tests were undertaken for the entire learner group and each health professional group separately. Median and IQR typically reported for non-normally distributed data were provided. Furthermore, to explain the change across the time, the means were also listed. Effect size (r=z/  ) was calculated based on the method recommended by Fritz et al24 and Pallant,25 0.5 was deemed a large effect, 0.3 was deemed a medium effect and 0.1 was deemed as a small effect.24 95% CIs of the effect size were calculated via the calculator online.26
) was calculated based on the method recommended by Fritz et al24 and Pallant,25 0.5 was deemed a large effect, 0.3 was deemed a medium effect and 0.1 was deemed as a small effect.24 95% CIs of the effect size were calculated via the calculator online.26
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
Of the 1946 learners, the majority were nurses (74.2%, n=1443), followed by allied health professionals (15.0%, n=291) and doctors (10.9%, n=212). Of these, 63.2% learners (n=1229) worked in acute hospitals while 36.8% (n=717) learners worked in other settings. Demographics also showed that 84.4%(n=1643) learners were from Australia, and 15.6%(n=303) learners were from other countries.
Impact of module learning on learners’ self-perceived EOL care knowledge, skills, attitude and confidence
Wilcoxon Signed Ranks Tests revealed statistically significant improvement in learners’ self-perceived EOL care knowledge, skill, attitude and confidence after completion of EOLE modules regardless their disciplines(p<0.001). The effect size of improvement in self-perceived EOL care knowledge, skills and confidence ranged from 0.36 to 0.53, demonstrating a medium to large effect and the effect size of improvement in self-perceived EOL care attitude ranged from 0.28 to 0.37, showing a small-to-medium effect (table 2).
Learners’ self-perceived end-of-life care knowledge, skill, attitude and confidence
Impact on intention to practice change
Overall, learners who completed at least one of the intention to practice change postevaluation question of the modules (maximum 10 modules) (n=1478) reported a high level of intention (median=4, IQR=1) to change their practice after completion of EOLE module learning, regardless of their discipline, with level of intention to practice change from allied health professionals (n=196, median=4, IQR=1), doctors (n=178, median=4, IQR=1) and nurses (n=1104, median=4, IQR=1).
Discussion
Evaluation results showed that EOLE learners were HCPs from different disciplines, including allied health professionals, doctors and nurses, although the majority were nurses. Learners were from Australia and other countries, showing that EOLE was an accessible online course for HCPs. EOLE online education modules allow a flexible, self-paced way for HCPs to update their EOL care knowledge and skills based on their individual needs. This online learning style is particularly important during the current pandemic environment where the traditional face-to-face training might be challenging and the demand for EOL care knowledge and skills have increased.27
Evaluation results indicated a positive impact on learners’ self-perceived EOL care knowledge, skill, attitude and confidence after completion of EOLE modules, which may help HCPs build their capacity in providing quality EOL care in hospitals.10 28 Module learning also prompted HCPs’ intention to change their clinical practice, with intent considered a predictor for behaviour change.29 These results further support the positive impact of EOLE module learning.4 20 30 More importantly, addressing the aim of this evaluation, learners from these varied disciplines demonstrated statistically significant improvement of self-perceived EOL care knowledge, skills, attitude and confidence, and reported a high level of intention to change their practice after completion of the module learning, suggesting that all HCPs could benefit from EOLE education regardless of their discipline. These results demonstrated the suitability of EOLE education modules for all HCPs as a quality education course which are consistent with the scope and aim of EOLE project. Having said that, the degree of benefit gained by allied health professionals and doctors should be considered cautiously due to the small sample size compared with the nurses. Future studies are needed to further explore the effectiveness of module learning on these two groups.
There are some limitations to this study. There was a lack of demographics details such as age, gender, years of experience in EOL care due to the limited capacity of the data collection platform (LMS). The nature of voluntary participation might contribute to selection bias, as the perspectives of non-responders to the evaluation components might be different.20 31 Again, evaluation questions were self-perceived, which may not reflect the objective changes.32 To also note is that the learning objectives for each education module were not specified, nor drawn out in the evaluation. The evaluation questions are standardised across the different modules and not designed for each of the learning objectives in individual modules. The advantage of this approach is that the education module could be evaluated broadly in a similar way, while the disadvantage is that the evaluation does not breakdown to focus on the nuance of individual modules. Furthermore, we acknowledge that the positive impact of education itself may not reflect the improvement of actual clinical practice.33 An ongoing longitudinal study is in progress to further investigate the influence of EOLE education module in clinicians’ clinical practice.
Conclusion
EOLE modules were designed for all HCPs regardless of their experience in EOL care, and the evaluation results demonstrate a positive impact of the EOLE modules on HCPs from different disciplines. Therefore, EOLE could be a reliable and accessible online EOL care education resource for HCPs of all disciplines in acute hospitals and other health settings to improve their EOL care knowledge, skills and confidence, build up their capacities in providing quality EOL care to patients and their families.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank all people who contributed to the development and evaluation of End-of-Life Essentials education modules.
References
Footnotes
Contributors KD leads the development and evaluation of End-of-Life Essentials (EOLE) education modules, and critically reviewed and revised the manuscript. HY collected and analysed the data, drafted the manuscript. DR is coprincipal investigator for the EOLE project, contributed to the development and evaluation of the education modules, critically reviewed and revised the manuscript. All authors have read and approved the final manuscript. All authors have read and agreed to the published version of the manuscript. KD is responsible for the overall content as guarantor.
Funding End-of-Life Essentials (EOLE) is funded by the Australian Government Department of Health, National Palliative Care Projects Agreement ID 4-E1NRR7S. Some authors (KD and HY) are part or wholly funded to conduct the EOLE project.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.