Article Text

Abstract
Background Swansea Bay University Health Board (SB UHB) has been trialling a primary care audiology pathway since 2016. The pathway enables patients with hearing, tinnitus or wax problems to be triaged directly to the audiology department acting as the first point of contact, freeing up general practitioners, Ear, Nose and Throat consultants and nurses to see patients with more complex health conditions.
Purpose To evaluate the efficiency of the SB UHB primary care audiology pathway.
Particular focus Clinical outcomes of patients seen through the SB UHB primary care audiology pathway.
Overview The vast majority of patients seen through the SB UHB primary care audiology pathway are managed without the need for onward referral (≥87%).
- Healthcare quality improvement
- Primary care
- Staff Development
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Over the last decade, the Welsh Government has published and acted upon strategic frameworks to radically change the way National Health Service (NHS) Wales services are provided,1 2 ultimately shifting the emphasis of healthcare provision away from preservation and towards prevention and early intervention.3 Primary care (PC) services will play a vital role in achieving the goals set out in ‘A Healthier Wales’ and are in the process of being transformed to integrate services historically considered secondary care into community settings through the formation of multidisciplinary team (MDT) PC clusters.4 To support the development of MDT PC clusters, the Welsh Government provides funding through Pacesetter and Transformation Programmes to pilot innovations in PC.5 Trials to provide audiology services in PC settings are ongoing throughout Wales.6 This short report outlines the approach taken by Swansea Bay University Health Board to implement PC audiology services.
Swansea Bay PC audiology model
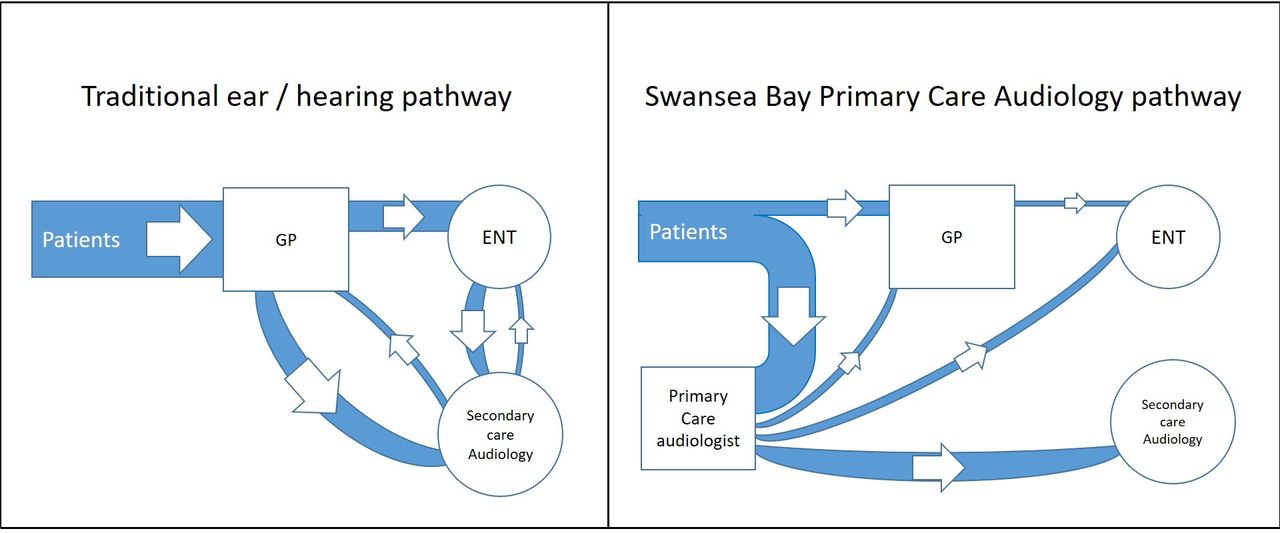
The Swansea Bay PC audiology model replaces the general practitioner (GP) with an advanced audiology practitioner (AAP) as the first point of contact for patients with concerns about hearing, tinnitus or wax (figure 1). With routine wax removal being the most common request, these patients are triaged to an associate audiologist who works in parallel with an AAP. This parallel working model allows audiology to deliver a first contact hearing and tinnitus service alongside an efficient and modern integrated wax removal pathway. It is the first of its kind in audiology and is an example of leading the way in modern community healthcare settings.

Comparison of the former Swansea Bay University Health Board adult hearing loss pathway with the primary care audiology pathway. ENT, Ear, Nose and Throat; GP, general practitioner.
As AAPs are non-medical healthcare professionals, it is essential that there are clear pathways in place for patients to obtain appropriate levels of medical advice should any red-flag symptoms (eg, bleeding, discharge, sudden sensorineural hearing loss) be identified. Criteria prompting onward referral from PC audiology were developed using guidelines produced by the National Institute for Health and Care Excellence alongside discussions with local Ear, Nose and Throat (ENT) colleagues and are provided in online supplemental information 1.7 The full scope of practice of the AAP and associate audiologist is provided in online supplemental information 2.
Supplemental material
Supplemental material
Clinical outcomes of care
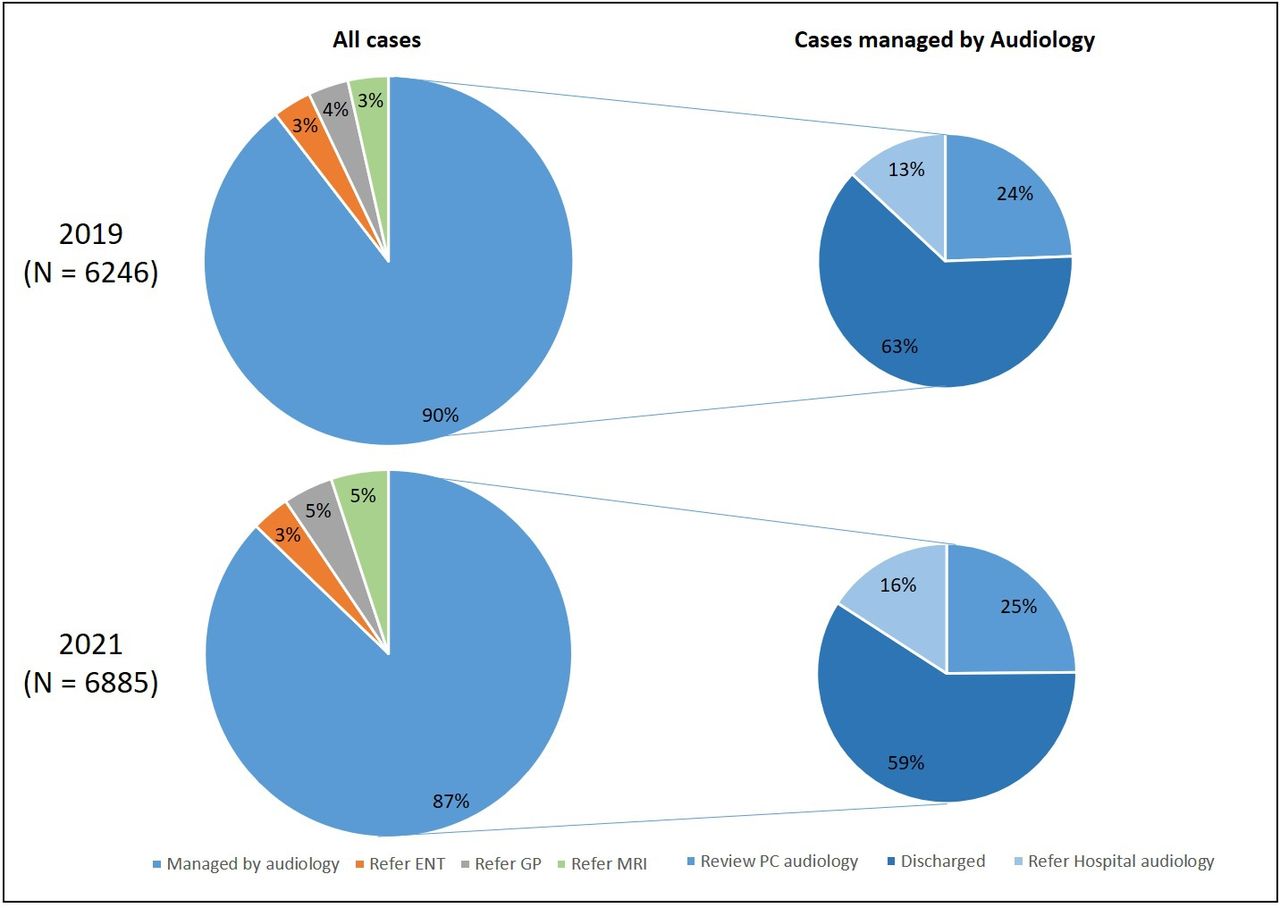
Analysis of patient outcomes in 2021 reveals that 87% of cases seen through the Swansea Bay PC audiology pathway are managed by the audiology department, either within the PC setting or referred on for secondary care. Further, only 5% of patients require a consultation with the GP and 3% generate an ENT referral. These statistics have remained consistent over time with little variation compared with pre-pandemic patient outcomes (figure 2).
{kind=link}
{kind=link}
Comparison of primary care audiology patient outcomes, collected before and during the COVID-19 pandemic. ENT, Ear, Nose and Throat; GP, general practitioner.
Referrals that are made to ENT from an AAP have the benefit of full audiometric assessment, otoscopy images if applicable and referral for MRI investigation of internal auditory meatus where indicated, maximising available information for ENT triage. This is a stark contrast to an ENT referral from a GP which would typically include a brief clinical history and list of medication. Furthermore, development of the AAP’s clinical licence has meant that patients historically requiring ENT management such as those with unilateral tinnitus and sensorineural asymmetry can now have all routine investigations coordinated entirely within a PC setting. Consequently, only patients with identified neoplasms—typically <2 per 100 000 persons per year—require ENT input.8
Future developments
Although still in its infancy, PC audiology services have scope to increase the services that can be offered and further reduce demand on GPs and ENT departments as the role of the healthcare scientist develops and expands. Dizziness is one of the most common presenting complaints to GP practices,9 10 and vestibular-trained AAPs could assist in diagnosis, further reducing pressure on GP services. Benign paroxysmal positional vertigo (BPPV) is a leading cause of dizziness in older populations,11 and consequently a basic BPPV assessment and treatment service would benefit both patients and GP practices.
From the data collected in 2021, ear infections were the most common reason for GP involvement despite being seen by an AAP. Developing the role of the AAP to allow them to prescribe topical antibiotics when required would drastically reduce the need for GP intervention in patients seen by the PC audiology team. Further, patients with complex ear canals (eg, following surgery) who also require wax removal are typically reviewed for regular microsuction in the ENT department. Additional training for AAPs on how to safely manage complex ears will serve to reduce this demand and prevent the need for ENT review.
Limitations
Patient-reported outcome measures (PROMs) and patient-reported experience measures are increasingly being used in routine practice throughout NHS Wales as a means of service evaluation.12 This short report solely focused on recorded clinical outcomes as there are currently no validated PROMs for PC audiology services. Having a validated PROM for PC audiology services would enable patients to participate in the evaluation of this service in line with value-based healthcare principles.3 Given the resources and time needed to develop questionnaires, it is prudent to explore whether any pre-existing PROMs can be used for this purpose before designing a new instrument.13
Conclusions
The Swansea Bay PC audiology pathway has been shown to reduce demand on GPs, practice nurses and ENT consultants, not only saving clinical and patient time but also reducing the patient pathway by up to 6 months in some cases. This naturally increases GP and ENT consultant availability to see patients with more complex health conditions.
The pathway also improves patient accessibility to audiology services by creating more points of access in community settings closer to home. This means that audiological investigation is available to patients sooner, improving pathways for time-sensitive conditions such as sudden sensorineural hearing loss.7 With continued development of the AAP role, the percentage of patients requiring GP or ENT referral will likely decrease further.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors would like to thank Sarah Theobald, Head of Audiology, Swansea Bay University Health Board, for providing oversight of this short report.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JackAllum1
Contributors All authors contributed to the manuscript equally. TL and NP undertook data acquisition. TL, NP and JA completed analysis and interpretation of results, and production of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.