Article Text

Abstract
Background Chronically ill adults insured by Medicaid experience health inequities following hospitalisation.
Local problem Postacute outcomes, including rates of 30-day readmissions and postacute emergency department (ED), were higher among Medicaid-insured individuals compared with commercially insured individuals and social needs were inconsistently addressed.
Methods An interdisciplinary team introduced a clinical pathway called ‘THRIVE’ to provide postacute wrap-around services for individuals insured by Medicaid.
Intervention Enrolment into the THRIVE clinical pathway occurred during hospitalisation and multidisciplinary services were deployed into homes within 48 hours of discharge to address clinical and social needs.
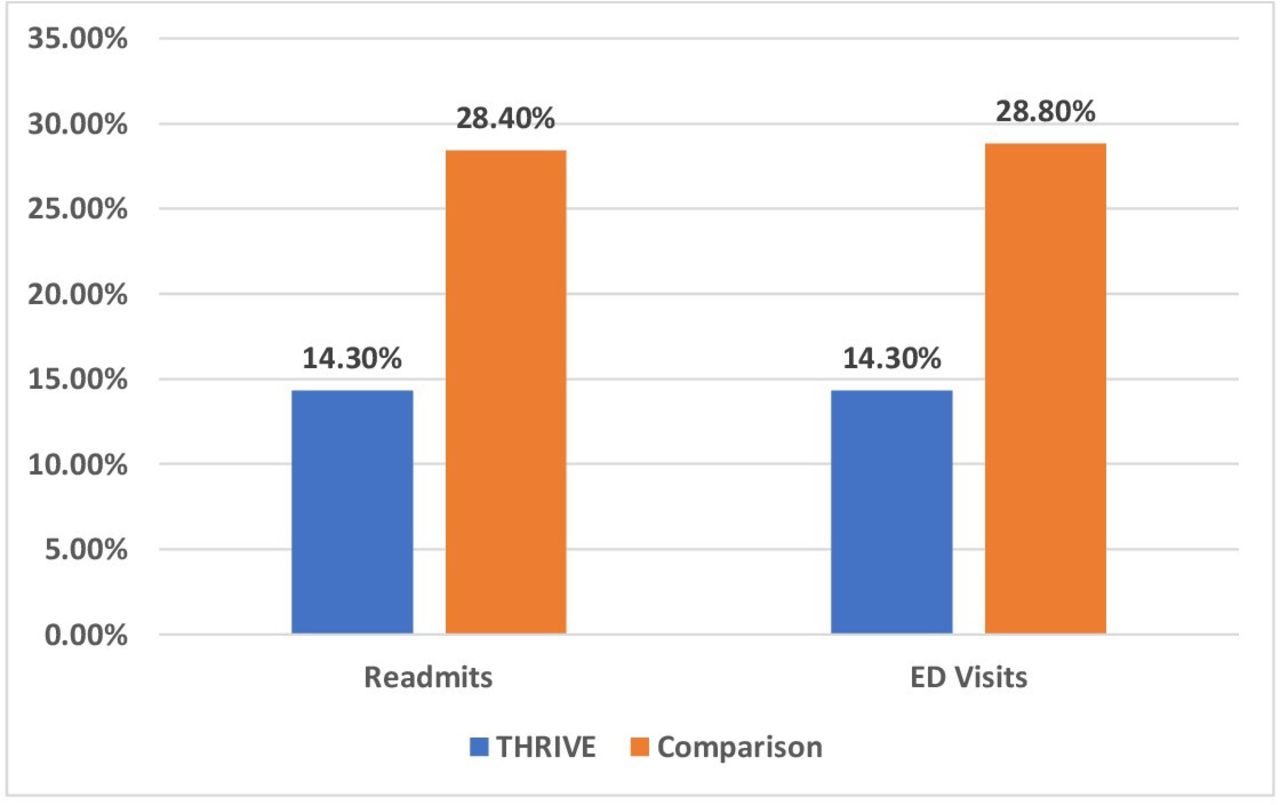
Results Compared with those not enrolled in THRIVE (n=437), individuals who participated in the THRIVE clinical pathway (n=42) experienced fewer readmissions (14.3% vs 28.4%) and ED visits (14.3% vs 28.8 %).
Conclusion THRIVE is a promising clinical pathway that increases access to ambulatory care after discharge and may reduce readmissions and ED visits.
- Community Health Services
- Continuity of Patient Care
- Health Equity
- Multiple Chronic Conditions
- Transitions in care
Data availability statement
No data are available. Our health system EHR data is not accessible.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Community Health Services
- Continuity of Patient Care
- Health Equity
- Multiple Chronic Conditions
- Transitions in care
What is already known on this topic
Health inequities among Medicaid-insured individuals are due in part to system failures attributable to care fragmentation, a lack of care coordination and insufficient attention to health-related social needs.
What this study adds
Healthcare system and process innovations that provide a holistic and integrated approach to care that centres physical, social and emotional needs of chronically ill low-income patients offers an opportunity to reduce inequities among Medicaid-insured individuals.
Early results from year 1 of the THRIVE clinical pathway suggests increasing home care referrals and reductions in 30-day readmission and ED use compared with baseline.
How this study might affect research, practice or policy
Improvements in posthospitalisation outcomes for Medicaid-insured individuals enrolled in the THRIVE clinical pathway signal the value of innovative improvements in healthcare delivery and system processes as a lever to reduce health disparities.
Background
Individuals with multiple chronic conditions require complex care management and often experience significant challenges when transitioning from hospital to home. These transitions are compounded for the nearly 8 million hospitalised individuals, insured by Medicaid who are disproportionately Black, Indigenous, People of Colour (BIPOC) and experience a higher burden of chronic disease and disparities in postacute care outcomes.1–7 In the USA, adults insured by Medicaid have incomes 138% below the Federal Poverty Level (FPL) (roughly $17 800 annually) or up to 155% of the FPL for households.8 They are 15% more likely to be readmitted than privately insured individuals citing significant health-related social needs such as financial stress, high out of pocket medication costs and housing instability.9 10 Compared with individuals insured by Medicare, they are more likely to experience complications and emergency department (ED) visits following hospitalisation, owing in part to foregoing care due to costs and a lack of access to longitudinal community-based care, including specialists.11–15 Postacute outcome disparities experienced by Medicaid-insured individuals are also the result of care occurring during hospitalisation or immediately thereafter. For example, despite substantial evidence linking improved postacute outcomes to care coordination and continuity of care, transitional care practices vary across acute care settings16 with most lacking tailored approaches for patients with multiple chronic conditions and economic disadvantage.17
The lack of comprehensive transitional care support for low-income individuals insured through Medicaid, who are largely BIPOC, represents an example of how healthcare infrastructures, service delivery and the allocation of resources may advantage or disadvantage some groups over others and result in health inequities. Health inequities are unjust differences in health and well-being between and within groups of people caused by socially structured, and thus avoidable, marginalising conditions such as poverty, that are historically rooted in systemic racism.18 The impact of marginalising conditions is heightened during the period of transition from hospital to home when individuals are required to obtain medications or durable medical equipment, schedule and access follow-up appointments and understand and execute treatment orders all while coping with competing economic needs.19 In addition, low-income, individuals have repeatedly recounted experiences of discrimination based on socioeconomic and racial status during interactions with healthcare providers.20 These experiences may result in avoidance of healthcare settings and paradoxically increase ED utilisation or avoidable hospitalisations due to inadequate management of chronic illnesses.21
Persistent health inequities among Medicaid-insured individuals demand focused innovations that are centred in equity principles and bridge coordination and continuity between acute and community health providers. Such equity-centred innovations may include technology but should also embrace system and process improvements in care delivery.22 From our perspective, equity-centred principles also acknowledge the history of structural inequities that lead to disparate outcomes.23 24 With this understanding, equity-centred interventions must be contextually tailored to address organisational polices, practices and community contexts.
By necessity such interventions should also include stakeholders from diverse backgrounds with intimate knowledge of the local community and healthcare systems. This helps to ensure that the intervention is viewed as meaningful and will be accepted by participants and adopted into clinical workflow. Finally, because inequities experienced by lower status individuals are systemically linked to denied opportunities and resources, innovations that are centred in equity must redirect and or intensify these resources while addressing the health-related social needs requiring attention.
In the following, we present our early results of an innovative clinical pathway developed with a focus on health equity and a goal of supporting a growing population experiencing adverse outcomes, resulting from complex chronic illness, poverty, and structural inequality.
Local problem description
Our healthcare system, Penn Presbyterian Hospital (PPMC), is a Level 1 Trauma centre located in a large city in the Northeast, USA and serves over 300 000 residents of the local community.25 Approximately 75% of individuals on our Medicine Service are Black/African American, 58% are insured by Medicare and 24% are insured by Medicaid.25 26 Results from a study conducted by our team using machine learning and 2017 PPMC discharge data, found that one in five (21%) individuals with Medicaid experienced a readmission within 30-days compared with 6% of commercially insured individuals.27 Similarly, 17% of individuals with Medicaid experienced an ED visit within 30-days of a prior hospitalisation, compared with 4% of commercially insured individuals.15 Finally, the majority of individuals insured by Medicaid were discharged to home without further support, with 20% receiving a home care referral, compared with 31% of adults insured by Medicare and fewer accessing specialty care.27 Results of our single site study were consistent with others showing higher postdischarge utilisation and difficulty accessing postdischarge care among Medicaid insured individuals.4 28
Aware of these disparate outcomes and other challenges following hospitalisation, our interdisciplinary team of clinicians, researchers and community members formed a Working Group with the goal of codeveloping a solution. Using a participatory approach and Human-Centred Design thinking, we codeveloped an intervention to support transitions for low income individuals with multiple chronic conditions.22 29 Participatory activities described, extensively elsewhere, were conducted over the course of 6 months, and included over 80 hours of clinical interviews, 30 inpatient and outpatient observations and 44 stakeholder informal interviews and observations covering eight units in the hospital.22 The culmination of this process resulted in the development of the THRIVE clinical pathway. THRIVE provides 30-day wrap-around transitional care services for individuals with three or more chronic conditions, Medicaid insurance and a Philadelphia zip code.22 27 The goals of the THRIVE clinical pathway are to focus on the physical, social and emotional needs of Medicaid-insured individuals with multiple chronic conditions by providing intensive case management, care coordination, continuity of care and communication across acute and community settings.
Although experts have established evidence-based standards for care transitions, discharge planning and care coordination,30 31 the application of these practices vary across settings and there is limited research on how to tailor discharge support for individuals insured by Medicaid.11 32 The Transitional Care Mode (TCM), for example, emphasises the continuity of care across settings and between providers throughout episodes of acute illness (eg, hospital to home).33 In randomised trials, the TCM has demonstrated reductions in readmission and cost.31 34 However, TCM focuses on older adults and requires additional trained healthcare providers (Advanced Practice Nurses) to coordinate care. Similarly, community health workers (CHWs) have increasingly extended support to individuals following hospitalisation. At least one randomised trial evaluating the use of CHWs demonstrated a reduction in readmissions for individuals with significant social needs. Despite facilitating important links to social services, CHW’s are unable to address clinical needs for medically complex patients in real time.35–37 Similarly, additional studies, by Jackson et al,38 Liss et al39 and Balaban et al,40 describe interventions to address medical and social needs among economically disadvantaged adults. While two of the three interventions appeared to decrease rehospitalisations over the course of 6 months to a year,38 39 none yielded reductions in readmissions and ED use in the critical period of 30 days.
In the current paper, we describe the outcomes of THRIVE participants during the first year including using plan-do-study act (PDSA) cycles. We also report differences in frequency of 30-day readmission and ED utilisation for individuals participating in the THRIVE clinical pathway compared with those that did not. We also describe frequency of referrals to community-based clinical and social services (ie, home care, primary care, specialty care, social workers and CHWs).
Design: THRIVE program description
With THRIVE, individuals are identified by Nurse Case Managers during hospitalisation using a predictive algorithm developed by our team.27 Within 48 hours after discharge, THRIVE enrollees receive a visit from a home care nurse. During home care visits, nurses serve as health coaches and spend time reviewing medications, and discharge orders, completing medication reconciliation and developing person-centred goals of care. THRIVE enrollees receive other clinical care services as warranted, including occupational therapy, physical therapy and social workers during the immediate days following a hospital discharge. THRIVE participants are assessed for social needs and referred to a CHW, as needed, who provides an additional layer of community-based support (figure 1).
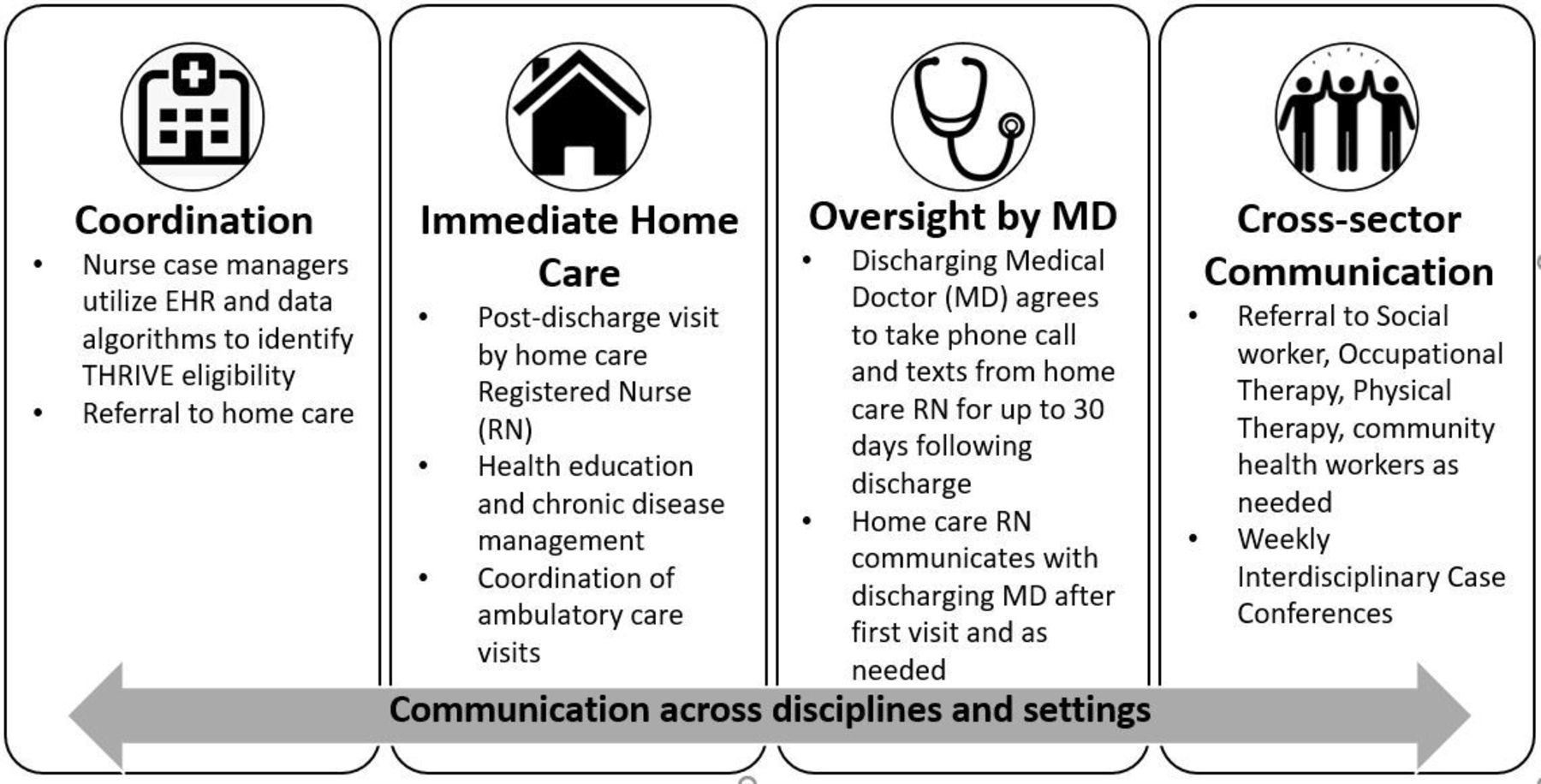
The THRIVE clinical pathway. EHR, electronic health record.
Another important aspect of the THRIVE clinical pathway includes the extension of support from the hospital-based discharging physician to patients following discharge. Clinical support from discharging physicians is provided through telephone and electronic health record (EHR) contact with home care nurses at the completion of the first home visit through calls or direct messaging. Nurses raise questions about medications (eg, medications found at home that are not documented in the discharge instructions), request additional medical equipment, clarify discharge orders and address emerging symptoms in real time with the provider who most recently oversaw the individual’s care. Our partnership with discharging physicians in this way is novel and actively works to address acute clinical needs attributed to the recent hospitalisation or to destabilisation of a co-occurring chronic condition in the days following discharge.
Following discharge, the THRIVE teams hosts virtual case conferences with the interdisciplinary team where each THRIVE participant is discussed weekly for 1 month after discharge. A home care Nurse Manager helps to facilitate weekly case conferences by serving as a clinical liaison to the THRIVE team and bringing to the team social and medical concerns that were noted during home care engagement. The THRIVE team is fully empowered to provide a holistic and integrated approach to care by being responsive to our clients’ needs (physical, social and emotional). By centring the health-related social needs of Medicaid patients, we directly address many of the factors that drive health inequities (ie, transportation, housing and food insecurity) by facilitating referrals to community-based resources including CHWs, or assistance with applications to low-cost housing.
Methods
We describe changes in monthly referral during the first year of the launch of the THRIVE clinical pathway. We also describe connections made by our team to clinical and social supports (ie, home care, primary care, specialty care, social workers and CHWs). We then compared individuals enrolled in THRIVE (April 2019–March 2020) to Medicaid-insured individuals not enrolled in THRIVE to evaluate differences in postacute care utilisation (ie, rehospitalisation, ED use). Comparison group data were provided by the health system’s data store, and included deidentified data derived from the EHR that included demographic (eg, age, race/ethnicity, sex) and service utilisation data (eg, rehospitalisation, ED use). The Squire for quality improvement (QI) reporting was used to detail the results of the QI initiative.25
Outcome measures
Monthly referrals to THRIVE were calculated and all other utilisation outcome measures were assessed within 30 days of discharge from the hospital. These additional outcome measures included clinical (ie, home care, primary care, specialty care) and social support linkage (ie, social workers and CHWs) and postacute utilisation measures (ie, readmission and ED utilisation).
Ethical considerations
Our QI pilot project received approval from our institution’s Quality Improvement Institutional Review Board prior to beginning this work.
Strategy
We used PDSA cycles to implement the THRIVE clinical pathway. Our PDSAs were grouped into three main strategies.
PDSA Cycle 1: The THRIVE pathway was launched officially in April 2019 as a QI project. Hospital-based cased managers manually identified THRIVE eligible patients by insurance status. We began with two discharging physicians and home care referrals to patients discharged to four zip codes. Home care nurses provided care to THRIVE referred patients as a part of their normal case load.
PDSA Cycle 2: In months 4–5 we expanded the zip codes of THRIVE referrals from 4 to 20 and all discharging physicians on the Medicine service were able to make THRIVE referrals.
PDSA Cycle 3: In month 6 of the pilot, we initiated an EHR Flag to help automate the identification of THRIVE eligible patients while on the inpatient unit based on a predictive algorithm developed by our team. The EHR ‘flag’ draws on principles of behavioural economics to provide a visual cue in the medical record to ‘nudge’ Case Managers to activate a THRIVE referral.
Analysis
Data on THRIVE participants were derived from the EHR then imported into the REDCap database and appended to the comparison group dataset in STATA. An indicator variable was created to designate THRIVE participation. Descriptive statistics were performed for demographic, clinical and social support linkage (ie, home care, primary care, specialty care, social workers and CHWs), postacute utilisation measures (ie, readmission and ED utilisation) using means for continuous and counts and percentages for categorical data. Clinical and social support data were unavailable for the comparison group; therefore, service linkage data was only evaluated for THRIVE participants. All analyses were completed with STATA V.15.0.
Results
THRIVE was officially launched as a pilot in April 2019 and during the first 12 months, Case Managers identified and referred 75 individuals to the clinical pathway; of which 42 went on to receive the full range of THRIVE services. The most common reasons for enrollees not continuing in THRIVE included refusal of home care services, inaccurate postdischarge contact information, Medicare or commercially insured or the need for higher level care (ie, rehabilitation or skilled nursing facility placement).
Average monthly referrals increased in the first year from an average monthly referral of four in cycle 1 to seven in cycle 3. We began with two discharging physicians providing posthospitalisation supervision and consultation with home health nurses in cycle 1 and ended with 26 physicians at the end of year 1. During these calls, nurses and physicians addressed issues regarding medication reconciliation such as the initiation of new medications and making the physician aware of other medications the patients were taking in the home. They also provided clarification of orders and discharge instructions. On average physicians received one call per month.
THRIVE enrollees were on average 58 years old, 59% male, 95% Black/African American, 67% insured by Medicaid only and 33% dually enrolled in Medicaid and Medicare (table 1). The comparison sample included 437 individuals discharged from medicine services at our hospital. All individuals in the comparison sample were insured by Medicaid (65%) or dually enrolled in Medicare and Medicaid (35%) and discharged to home. They were on average 51 years old, 45% male and 85% were Black/African American.
Patient characteristics of individuals participating in the THRIVE clinical pathway and comparison group and their community-based service utilisation within 30 days of discharge
All THRIVE participants (100%) received nursing home care services within 48 hours of discharge, 68% had a primary care visit and 67% had a specialty care visit within 30 days of discharge. THRIVE enrollees received referrals to a range of other in-home and community-based services such as social workers (50%), physical therapists (50%) or CHWs (40.5%). Over the course of the first year, we have addressed clinical and social needs across our THRIVE participants including, assistance with housing, securing transportation, obtaining affordable medications, ordering durable medical equipment and making connections with mental health and substance abuse services. THRIVE enrollees experienced fewer 30-day ED visits (14.3%; n=6) compared with patients not enrolled (28.4%; n=124, p<0.05). Similarly, THRIVE enrollees experienced fewer 30-day readmissions (14.3%; n=6) compared with patients not enrolled (28.8%; n=126, p=0.05; figure 2).

{kind=link}
{kind=link}
Rates of readmissions and emergency department visits within 30 days of discharge for THRIVE (n=42) versus comparison group (n=437). ED, emergency department.
Discussion
The THRIVE clinical pathway sought to improve postacute care outcomes by intensifying transitional care support, increasing linkages to postacute community-based services (ie, home care, primary care, specialty care and social services) and decreasing the frequency of 30-day readmissions and ED utilisation for Medicaid-insured individuals transitioning from hospital to home. Using a multicomponent innovation, we demonstrated clinically meaningful reductions in readmissions, ED visits and increases in postacute connections to primary and specialty care as well as social services. In addition, our team has intensified our attention to the social determinants of health and health-related social needs of THRIVE participants by assisting with challenges related to housing insecurity, substance use and difficulty accessing medication or durable medical equipment.
Multicomponent process innovations like THRIVE, which focus specifically on Medicaid-insured individuals, provide important and necessary services to a population that is generally younger, yet coping with significant chronic illness. The average age of THRIVE participants is 58 and diagnosed with on average 14 chronic conditions and numerous compounding social needs. The majority of THRIVE participants are members of a racially minoritised community (95% Black/African American) and are additionally subject to cumulative disadvantage because of ongoing systemic racism and structural inequality. With THRIVE, we intentionally allocate resources to support low-income minorities who need intensive health and social resources.
Our findings of reductions in readmissions and ED utilisation are clinically meaningful and may be linked to our intentional focus of connecting THRIVE participants to primary and specialty care within the first month posthospitalisation. More importantly through both home care services and continued clinical oversight by hospital-based physicians, we are able to intensify the services provided in the aftermath of an acute hospitalisation. The days and weeks following hospitalisation can be wrought with new treatment regiments, medication changes and the need for additional specialty intervention. Navigating the complexities of these additional expectations is made even more difficult when coping with limited social or material resources. Our team focuses on the holistic health needs of THRIVE participants throughout the clinical pathway and purposefully uncovers and addresses concerns that may have otherwise gone unmet.
Our experience with THRIVE demonstrates the ability of multisector collaborators working in partnership to address the needs of individuals insured by Medicaid with multiple chronic conditions. This project also provided an opportunity to gain insights about feasibility of the THRIVE pathway and to learn quickly from our failures. Our early experiences have prompted the team to think more critically about our selected clinical outcomes. While reductions in ED visits and readmission are key quality indicators and are aligned with our health system’s goals of containing costs and delivering value-based care, they may not fully reflect relevant patient-reported outcomes that are key to understanding the effects of innovations that address inequities as well as clinical and social needs.41 Subsequent studies of THRIVE will include a combination of quantitative and qualitative approaches that capture patient experiences alongside how and why the intervention works and what contextual elements, adaptations and implementation strategies are necessary for success.42
Limitations
We acknowledge several limitations with this project. We were unable to access data regarding postacute community-based service linkages of the comparison group for home care, primary care and specialty care services. Our sample is from a single institution, which along with our sample size, limits generalisability. We did not evaluate the cost implementing the THRIVE clinical pathway, though we developed THRIVE with an intent not to require the addition of health personnel and instead leveraged the expertise of providers currently working for the health system or in the community. Nonetheless, shifting the workflow of providers may influence cost in unintended ways that may prohibit expansion to other settings. Our early findings suggesting reductions in readmission and ED utilisation should be viewed with caution as we do not account for other factors, including differences between clinical presentation, language barrier or patient preferences that may differ between THRIVE and the comparison group. Future studies with larger sample sizes will allow us to conduct analyses with more robust risk adjustment. Despite these limitations, findings from the THRIVE pilot offer promising preliminary data from which to launch future efficacy focused trials.
Conclusion
The THRIVE clinical pathway addresses gaps in care delivery that are linked to health inequities for Medicaid-insured individuals by focusing their physical, social and emotional and emphasising intensive case management, care coordination, continuity of care and communication across acute and community settings. Early results from the THRIVE clinical pathway suggest the value of interdisciplinary and community-based collaborations and healthcare innovations that target healthcare delivery and system processes.
Data availability statement
No data are available. Our health system EHR data is not accessible.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but The University of Pennsylvania Institutional Review Board determined that our project qualified as Quality Improvement and did not require further IRB approval. No reference or ID number was provided. (date 27 February 19) exempted this study. Consent was not required because this project was deemed to be a QI study as the procedures of our study were not experimental or untested (ie, receipt of home care services).
References
Footnotes
Contributors JMBC and HB developed the original manuscript. JMBC oversaw the analysis and HB conducted the analysis. JMBC, HB, RF, MD, MG-M, JB, KR, EP and PC contributed to the data curation, conceptualisation, drafting and editing of this manuscript. Guarantor - JMBC.
Funding Funding for this project was provided by the Leonard Davis Institute of Health Economics (Brooks Carthon, Co-PI; Williams, Co-PI), the Center for Healthcare Economics and the Office of Nursing Research, University of Pennsylvania School of Nursing. There are no award/grant numbers for these funding sources.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.