Article Text

Abstract
Background Surgery is recommended within 48 hours of hip fractures for better perioperative outcomes. Yet, such targets still commonly remain a challenge. Our institution is no exception.
As part of a hospital-wide initiative, our anaesthesia department focused on improving perioperative processes with aims to reduce the time to first anaesthesia consult and surgery for hip fracture patients. Acknowledging multiple causes for surgical delay, we decided first to address anaesthesia-specific factors—(a) first anaesthetist contact usually happens after surgery is offered which leaves a short runway for preoptimisation, (b) this is compounded by varying degrees of anaesthetist involvement for follow-up thereafter. (c) There is a need to calibrate our perioperative care standards and (d) enforce more consistent auditing in quality assurance. This project was conducted in a 1000-bed hospital serving eastern Singapore.
Intervention We created an integrated anaesthesia consultant-led outreach service for hip fracture patients, based on a perioperative workflow system to provide proactive anaesthetist consults within 24 hours of admission in advance of surgical decision. This was streamlined with a coordinated follow-up system for preoptimisation until surgery.
Methods Our quality improvement project applied the iterative Plan-Do-Study-Act model from pilot to sustainability stage. We collected data at baseline followed by 6-monthly audits from electronic databases.
Primary outcomes measured were time to first anaesthesia consult and surgery. Secondary outcomes included rate of critical care reviews and admission, mortality rate, length of stay and time to nerve blocks.
Results Post implementation, our service reviewed >600 hip fracture patients. Median time to anaesthesia consult reduced significantly from 35.3 hours (2019) to 21.5 hours (2021) (p=0.029). Median time to surgery was reduced from 61.5 hours (2019) to 50 hours (2021) (p=0.897) with a 13.6% increase in patients operated <48 hours. Critical care admissions, 6-monthly and 12-monthly mortality rates and time to nerve block were reduced with a greater percentage of patients discharged within 10 days.
Conclusion Our project focused on improving anaesthesia perioperative processes to address surgical delays in hip fracture patients. Our consultant-led anaesthesia service ensured that proactive anaesthesia care was delivered to provide sufficient time for preoptimisation with greater standardisation to follow-up, better communication and quality assurance.
- anaesthesia
- PDSA
- surgery
- quality improvement
- audit and feedback
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Despite a lot of literature discussing the clinical care of hip fracture patients, there is a shortage of reports focusing on the practicalities of delivering such care especially from an anaesthetist’s perspective.
WHAT THIS STUDY ADDS
This study is the first of its kind to discuss the rationale, evolution and challenges faced while setting up an anaesthesia consultant-led outreach service to expedite hip fracture patients safely from presentation to surgery.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We hope to encourage a change in mindset that anaesthetists can play an impactful role in upstream perioperative care of hip fracture patients beyond just the operating theatre. This study design can be upscaled and applied to other patient groups facing similar perioperative constraints.
Introduction
With an ageing population, hip fractures will continue to rise.1 Such patients are often elderly, frail with multiple comorbidities. Challenges in optimisation are often balanced against the need to expedite surgery.
Changi General Hospital admits approximately 500 hip fracture patients a year. Over the past 3 years, >90% of such patients underwent operative treatment. With a strong focus on longitudinal care and collaboration among several disciplines, our integrated hip fracture pathway has significantly streamlined the care of hip fracture patients since 2014.2
Problem description
Nonetheless, we still face delays in hip fracture surgery—a pervasive problem across institutions.3 Our median time to surgery was 61.5 hours in 2019. Reasons for delays included lack of operating lists, patients who were deemed medically unfit, and those who were undecided as to surgery or were awaiting investigations such as laboratory results, COVID-19 screens and echocardiography for cardiac clearance.
Trends from 2018 to 2019 found increased delays, short-term and long-term mortality and critical care reviews (CCRs) and intensive care unit (ICU) admissions over time (table 1). In 2019, 53.5% of patients were discharged within 10 days. Despite recommendations for early nerve blocks,4 fewer patients were receiving them preoperatively with a median time of 41–46 hours from presentation.
Number and percentage of operated hip fracture patients requiring CCRs and ICU admission over time
Greater involvement, quality control and standardisation of perioperative care by the anaesthetist for hip fracture patients is widely recommended.5–7 Yet, internal analysis of our anaesthesia department’s practices revealed the following issues specific to hip fracture care:
The race against time to provide early and proactive anaesthesia involvement
The hip fracture patient was reviewed by multiple disciplines on admission, with the exception of anaesthesia. Occasional reviews requested earlier were seen by the duty anaesthetist during their emergency shift. Otherwise, the usual practice was to decide for surgery, schedule and then await an anaesthesia preoperative assessment the afternoon before. This was routinely done by a pool of junior anaesthetists. Only if required, the senior primary anaesthetist was consulted. This resulted in a short runway for optimal preoptimisation and potentially postponement of cases.
The need for standardised follow-up
During the perioperative journey, a patient may encounter different anaesthetists at various time points during preoperative assessment, regional nerve blocks, intraoperative care and potentially CCR if the patient deteriorates. It would be helpful to have one system to oversee this process longitudinally; this may encourage ownership, safe handover and direct focus more on medically unfit patients who had their surgeries postponed or critically unwell patients who may need CCR postoperatively.
Variations in perioperative standards
Within our department, we noticed different anaesthetists with varying thresholds for preoperative optimisation. Notwithstanding existing guidelines for preoperative echocardiography and cardiology referrals, members of the team may pre-emptively request for them to reduce delays downstream. These requests may sometimes be superfluous in impacting overall management and indirectly delay surgery.
The absence of an anaesthesia-focused auditing procedure for quality assurance
It is recommended that anaesthetists partake in standardised perioperative data collection for hip fracture care.6 Although quality assurance has long been integral in the hospital-wide approach for hip fracture management, we realised the need for anaesthesia to take a more focused and proactive lead in auditing anaesthesia-specific issues.
Aims of this quality improvement project
To reduce time to first anaesthesia consult with a 10% target increase in patients reviewed within 24 hours.
To reduce time to surgery with a 10% target increase in patients undergoing surgery within 48 hours.
These aims were specific for hip fracture patients eligible for surgery and targeted to be achieved over 18 months.
Aims of this report
This report discusses the rationale, steps and challenges behind an anaesthesia-specific quality improvement (QI) initiative. It is written according to the Standards for Quality Improvement Reporting Excellence 2.0 guidelines.8
Rationale
Our rationale was based on the need to target internal issues first which were anaesthesia-specific and modifiable within our control. We acknowledge this as part of the labyrinth of hospital-wide factors but do recognise how changes in the microsystem impact the macrosystem.
Methods
Context
Our anaesthesia department has 30 consultants covering several subspecialties—critical care, regional, pain and perioperative services. Hip fracture surgery is performed electively in a dedicated orthopaedic theatre or as an emergency by different orthopaedic teams.
REDCap (Research Electronic Data Capture) is a web-based software platform designed to support data capture. By 2019, multiple services within our hospital have adopted this platform. Prior to our project, there was no electronic interface to help with notification, follow-up or coordination of anaesthesia care for hip fracture.
Intervention
The intervention was the formation of a perioperative anaesthesia outreach service for hip fracture patients based on four main principles:
For more proactive anaesthesia input, we formed a consultant-led outreach team, following a standardised workflow to see eligible patients within 24 hours of admission. Compared with pre-existing practices, our input may at times be way in advance of surgical decision.
For better communication and coordination, we developed a one-stop database to facilitate continuity of perioperative optimisation until surgery was successfully performed.
For better quality of care and consistency, we collaborated with multiple disciplines to provide more up-to-date evidence-based guidelines and recommendations specific to our local cohort.
For continual quality assurance, we conducted regular audits based on iterative Plan-Do-Study-Act cycles.
Outreach team
On weekdays from 09:00 to 17:00, the service was run by a dedicated team of six anaesthesia consultants with strong interests in perioperative medicine, acute and chronic pain, regional anaesthesia and intensive care.
Patient selection
The inclusion criteria was all hip fracture pathway patients eligible for surgery who had neck of femur, intertrochanteric or subtrochanteric fractures.
The exclusion criteria was patients who already had surgery on selection, those who were conservatively managed or who were self-discharged from the hospital.
Standardised workflow
Early notification
Ideally, we aimed to see patients within 24 hours of selection. The case managers were pivotal in informing the team every weekday morning. This triggered an automatic cascade of reviews by anaesthetists.
Our preoperative clinical assessment aimed to be holistic, yet focused on the following:
Early decision for surgery based on fitness for surgery. If surgery was delayed for pending issues, targets were explicitly outlined with timelines for rescheduling surgery.
Early optimisation of conditions. Expediting only necessary investigations and referrals critical in making decisions for surgery and anaesthesia.
Early communication and coordination with multiple disciplines including anaesthesia.
Early pain control and decision for nerve block as part of a multi-modal analgesic regime.
Early risk assessment and risk counselling for shared decision-making.
Early planning for acute postoperative care.
Follow-up system
After the first anaesthesia consult, patients with pending issues were flagged for follow-up on REDCap as a safety net in addition to a verbal handover. Issues include medical optimisation, investigations, referrals or decision for surgery.
If there were no issues highlighted, the team still screened all unoperated patients until surgery, to ensure no unforeseen clinical deteriorations were missed.
Termination criteria
We discharged patients from the service when they were successfully operated on or conservatively managed.
Documentation and charging
We used electronic documentation for all anaesthesia consults based on a standardised template document created on Citrix, Sunrise Clinical Manager SCM.
Each patient was charged once on first consult regardless of the number of follow-ups required.
Patient and public involvement
Neither the patient nor the public were directly involved in this QI project.
Measures
Primary outcome
Access to anaesthesia
Time to first anaesthesia consult was measured by median time (hours) from emergency department (ED) registration to the first anaesthesia consult documentation.
The capture rate of patients was measured by the percentage of patients who had their first anaesthesia consult within 24 hours, 48 hours and 72 hours of ED registration.
The number of patients missed was measured by the number of patients who fit project selection criteria but referred to anaesthesia via other means instead.
The 2020 cohort was measured from March when the service was initiated.
Access to surgery
Time to surgery was measured by median time (hours) from ED registration to start of surgery and was expressed as a percentage of patients having surgery within 48 hours.
Secondary outcomes
Access to nerve block
The percentage of hip fracture patients receiving a preoperative nerve block over time.
Time to nerve block was measured in median time (hours) from ED registration to procedure start time.
CCR and ICU admission
Measured as the number of patients who required CCR and ICU admission over time. (Surrogate for clinical deterioration requiring critical care resources.)
A standard charge code was used to trend CCR outside of the ICU, regardless if reviewed preoperatively, postoperatively, electively or as an emergency.
An admission code was used to trend patients eventually requiring ICU admission.
Mortality rates
Inpatient, 6-month and 12-month mortality rates for operated patients over time.
Length of stay (LOS)
Median LOS from inpatient admission date to inpatient discharge date.
The percentage of patients discharged within 10 days of admission.
Data collection
Data were collected from the department of informatics.
The platforms include:
REDCap databases.
Citrix SCM.
Operating theatre management.
SAP Systems Applications and Products in Data Processing.
CCR patient documentation.
Data collection and analysis were performed by the ValueCare hip fracture programme facilitator and perioperative anaesthetists.
Missing data were validated from the source system to determine the data were indeed missing or due to incomplete documentation. If documentation was the issue, missing data were manually retrieved from other sources. As the majority of CCR paper documentation from 2018 to 2019 was missing, we resorted to using electronic data by charge and admission codes instead. The REDCap database for the service was only available after July 2020, so information before this was obtained mainly from SCM.
Two sample t-test was used to test statistical significance for the two primary outcomes with the assumption data was normally distributed.
Results
Evolution of the intervention
Stage 1 (pilot)
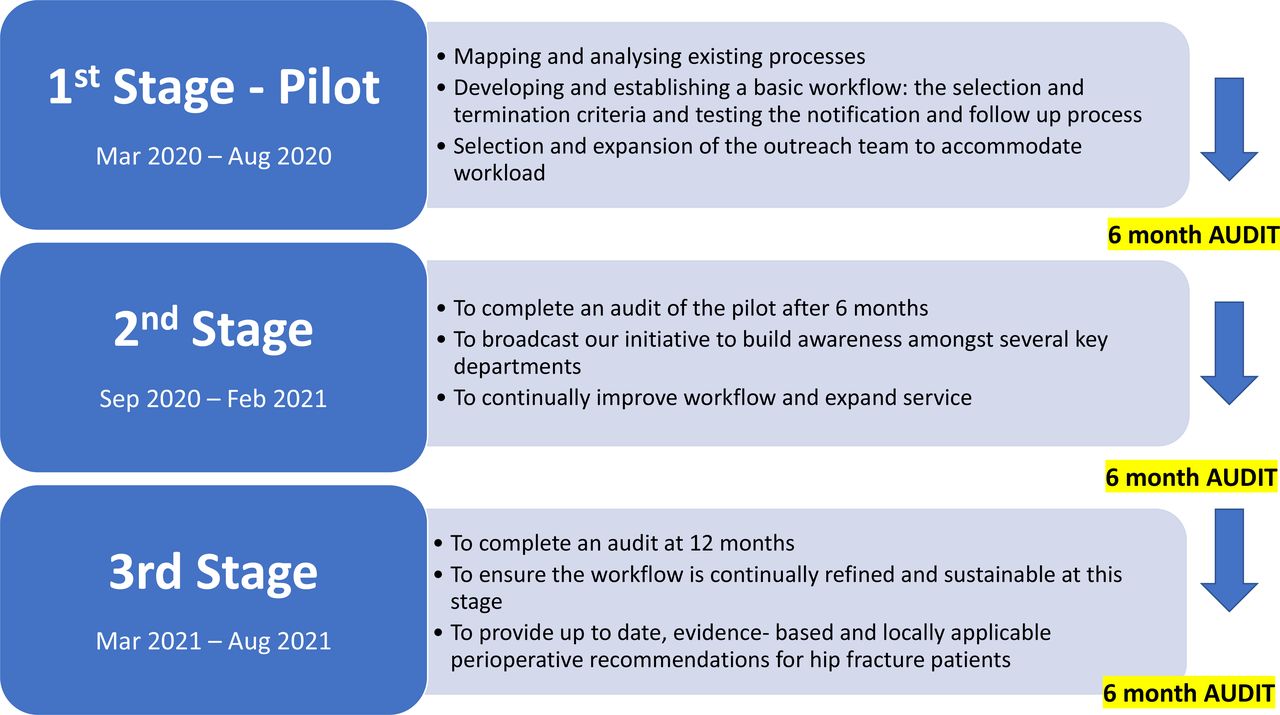
The actual ground work started with joining the orthogeriatric ward rounds. Through immersion, we understood the workflow better and forged new partnerships with key members. Existing processes were analysed with value stream mapping to identify bottlenecks to surgery and anaesthesia. With the use of root cause analysis and Pareto charting, we focused on the four most significant anaesthesia issues in need of improvement. Using change concepts with driver diagrams, we formed a basic workflow based on four principles (figure 1).

Stages of the quality improvement with main priorities and interventions over time. Figure created by the author with permission to use.
We selected only consultant anaesthetists with a special interest in perioperative medicine to participate in the project. Once the basic workflow was ironed out, we expanded from two to six consultants over time to cover the increasing workload.
Our priority was to redesign the current notification process while seamlessly integrating it into the pathway. We engaged a common point-of-contact to select and notify us of cases within 24 hours. This key role was played by the case manager who was already liaising closely with multiple disciplines. The original selection criteria was identical to that of the existing pathway to ensure consistency.
Our termination criteria evolved over time, originally it was based on fitness for surgery. However, this became rather unclear with dynamic changes to complex conditions. Often initially fit patients may deteriorate before surgery and be overlooked. For clarity and safety, we subsequently terminated on completion of surgery.
Our handover system also evolved with time. Initially, separate excel spreadsheets enumerating new and existing patients were created daily. This was laborious and time-consuming. A one-stop electronic platform to succinctly provide an up-to-date overview of all hip fracture patients was more ideal. This took several months to create on REDCap with multiple revisions before finalisation in July 2020. Now at a glance, patients are categorised into:
New patients.
Existing patients who are fit but still pending surgery or unfit with pending issues to optimise prior to surgery.
Patients terminated from the service (either has surgery or conservatively managed).
By the end of stage 1, an established workflow with key interventions was developed and implemented. As a team, we worked through challenges via regular feedback and made sure there was consensus among members.
Stage 2
Our first audit produced promising results. To increase awareness and support, we presented our workflow and pilot results to key stakeholders—the ValueCare team, case managers, anaesthesia, orthopaedics and orthogeriatrics departments.
Assured of the workflow and resources, we expanded our selection to encompass more patients regardless of:
Age: we included younger patients (<60 years). Such patients, although a small number, were not reviewed by orthogeriatrics due to an age cut-off but still suffered complex issues and uncontrolled pain.
Location: patients were initially reviewed by anaesthesia only after ward admission. This delayed our consults. To save time, we made our service more mobile by reaching out to patients regardless of location or admission status (eg, ED).
Subspecialty: delays were common in patients admitted under non-orthopaedic specialties; other competing medical issues obscuring a hip fracture could delay their presentation to the pathway.
As our selection criteria was more inclusive, we based our data on all operative hip fracture patients rather than patients strictly under the ValueCare hip fracture pathway.
We adjusted our workflow to adapt to various constraints posed by the COVID-19 pandemic.
At the beginning of the pandemic, due to uncertainties of the disease, we only reviewed patients after COVID-19 was excluded. Waiting for swabs became a significant reason for delaying an anaesthesia consult.
With improving knowledge of COVID-19 and more established workflows to address it, we eased our restrictions and reviewed all patients before swabs. Nonetheless, providers used personal protective equipment.
Our results highlighted two vulnerable groups at risk of uncontrolled prolonged pain with uncoordinated access to nerve blocks:
Nerve blocks were performed in the operating theatre by anaesthetists but only after admission from the ED. Delays were common due to bed shortages. In collaboration with the ED and pain service, we have since created a protocol that expedites the block by cutting out admission as a criteria.
Conservatively managed patients who were terminated from our service may still have uncontrolled pain. They were found to have markedly delayed nerve blocks compared with operative patients. Collaborating with the pain service and orthogeriatrics, we worked out a referral system on discharge to ensure such patients had their pain control followed up. We subsequently found improved time to nerve blocks for this cohort.
Stage 3
Using the 12-month audit results, we ensured our workflow was continually refined and sustainable by this stage.
In parallel, we individually reviewed cases requiring critical care, inpatient mortalities, cancellations and prolonged duration before surgery. We also reviewed cases with significant conditions (eg, acute stroke, embolism, myocardial infarction and anaemia). In collaboration with multiple disciplines, we worked to provide up-to-date, evidence-based and locally applicable perioperative recommendations for hip fracture patients for these conditions. These topics were regularly discussed and presented during multidisciplinary meetings.
Quantitative and qualitative outcome measures
Access to anaesthesia consult
Since January 2020, 695 patients were admitted to Changi General Hospital with a hip fracture, of which >90% of patients underwent surgery. Since implementation in March 2020, our service saw approximately 80% of operated patients who underwent surgery.
The median time to anaesthesia consult decreased significantly from 35.3 hours in 2019 to 21.5 hours in 2021 (p<0.029). The percentage of anaesthesia consults <24 hours increased significantly from 39% in 2019 to 67% in 2021 (p<0.003). The percentage of patients seen within 48 hours and 72 hours also increased.
Nine patients were missed initially but subsequently added to the service when the anaesthetist was notified via other means (eg, separate referral or by case managers later).
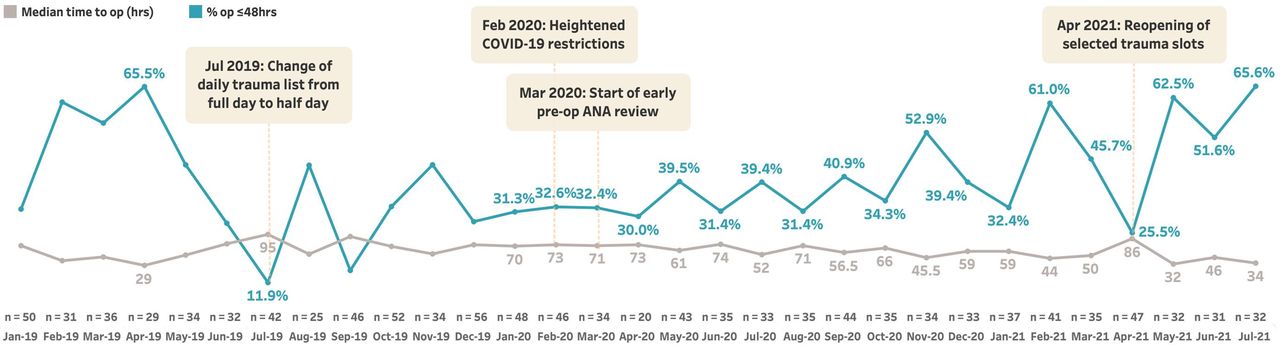
Access to surgery
Post implementation, time to surgery generally improved compared with previous years (figure 2). Median time to surgery was reduced from 61.5 hours in 2019 to 46 hours in 2021 (p=0.897). The percentage of patients having an operation within 48 hours increased from 38% in 2019 to 51.6% in 2021 (p=0.904). This was despite longer wait times for admission.
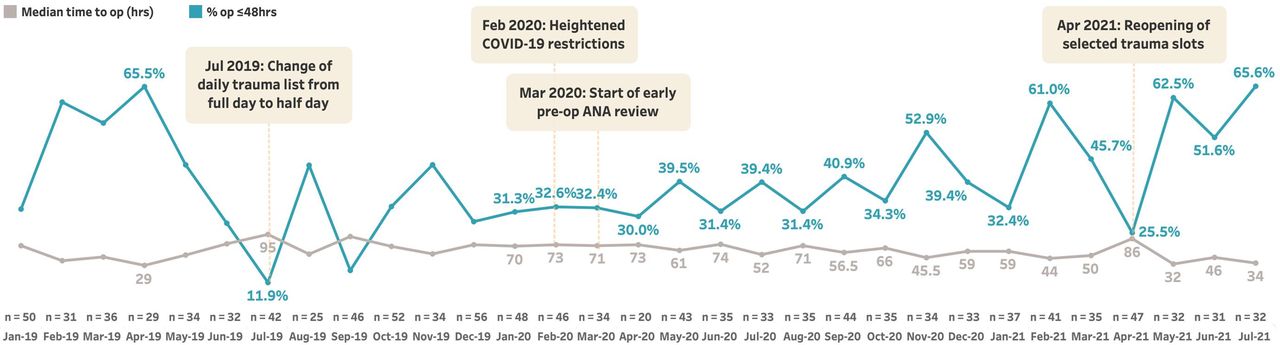
Time to surgery from January 2019 to July 2021 by month. Median time to op (hrs), operation in hours, in grey. % op≤48 hours, percentage of patients operated within or equal 48 hours, in blue. Figure created by coauthor with permission to use.
Since the pandemic, competing interests with heightened COVID-19 restrictions could have impacted access to surgery. A transient delay in surgery coincided with the temporary reopening of selected trauma lists from March to April 2021.
Access to nerve block
The percentage of all hip fracture patients who had a preoperative nerve block increased from 8.9% in 2019 to 15.3% in 2020. With faster access to surgery, this dropped to 9.8% in 2021. The median time to nerve block for operated patients improved from 41 hours (2019) to 28 hours (2020) to 22 hours (2021) (figure 3).

Time from emergency department registration to administration of nerve block for operated hip fracture patients over the years 2018, 2019, 2020 to July 2021. Median time in orange. Average time in green. Figure created by co-author with permission to use.
CCR and ICU admission
The critical care outreach team conducts CCR of patients in the wards as an elective follow-up after ICU discharge or as an emergency due to clinical deterioration preoperatively or postoperatively. A fraction of these patients may eventually need ICU admission. The percentage of patients requiring ICU admission was reduced from 2019 to 2021 while the percentage of patients requiring CCR increased (table 1). This may be attributed to greater vigilance for hip fracture patients perioperatively and collaboration between surgical and critical care teams, resulting in a lower threshold to refer and follow-up for safety reasons. A smaller denominator for total cohort in 2020 and 2021 compared with the earlier years may also result in a higher percentage.
Mortality rates of hip fracture patients
Comparing 2019–2020, three fewer patients died within 10 days of operation, inpatient mortality rate was reduced from 1.9% to 1.8% and 6-month and 12-month mortality dropped by 2.6% and 4%, respectively (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Depicts inpatient, 6-monthly and 12-monthly mortality rates of operated hip fracture patients. Figure created by coauthor with permission to use.
In early 2021, we noticed a slight increase in the inpatient mortality rate. Appreciating baseline variations, we considered how data may be skewed with a smaller denominator earlier in the year. An audit of mortalities in 2021 found most cases were American Society of Anaesthesiologist ASA class 4, dying sometime after surgery, from multifactorial or unpreventable causes. Most patients turned to palliative care halfway through their postoperative for comfort measures. Perhaps we should consider the changing thresholds we are adopting to operate on riskier patients earlier.
Length of stay
From 2019 to 2021, while the median LOS was maintained within the target 10 days, the percentage of operated patients discharged within 10 days increased from 53.5% in 2019 to 59.5% in 2021.
Discussion
Summary
A collaboration among a diverse mix of key stakeholders has always been paramount in ensuring safe and timely surgery for hip fracture patients. Beyond just assuming an intraoperative presence, the anaesthetist should have a greater role in the perioperative frontline alongside other disciplines. Armed with a practical overview and direct engagement in the perioperative process, anaesthesia can be a key facilitator between surgical and non-surgical specialties in expediting patients safely through the acute perioperative phases.
Our project aimed to reduce the time to anaesthesia consult and surgery by first targeting four key anaesthesia-modifiable factors. We successfully integrated a perioperative anaesthesia outreach service into the existing hip fracture pathway to deliver proactive anaesthesia consultation early, streamlined with a coordinated follow-up system thereafter. Key findings demonstrate significantly shorter anaesthesia consultation times upstream, with improved surgical and nerve block times downstream, in addition to fewer ICU admissions and long-term mortality without a deterioration in LOS.
Alongside optimal clinical care, the organisation and delivery of service matters as much. Despite an abundance of literature discussing the clinical management of hip fractures,5–7 9 there is a dearth of reports describing how to set up and audit an anaesthesia perioperative service for it. Without a substantial evidence base to guide implementation, we may be blind to how effective our perioperative care is, even when we know it is integral. Recent guidance is available on establishing enhanced perioperative care services to surgical patients at increased risk of adverse outcomes.10 Unlike building a service around a fixed location, we created a mobile outreach service which pragmatically addresses delays in admission or COVID-19 isolation. To our knowledge, our project is the first of its kind to be reported.
Strengths of our project:
It addresses a widespread and clinically relevant problem of surgical delays in hip fracture patients, uniquely from an anaesthetist perspective.
Our two primary outcomes were clinically relevant to our intervention, objective and easy-to-measure. With existing tools for data collection, it was easy to compare trends with baseline.
We focused on microsystems first by addressing problems locally within our department and emphasised on small-scale replicable changes that were effective timely and efficient.
Our workflow complemented existing processes to conserve costs and resources for example, REDCap was readily available and already used by the case managers. Our initial selection criteria mirrored that of the existing hip fracture pathway to ease implementation.
We strongly encouraged communication and engagement by learning what was important to each stakeholder to give ownership in the process. A carefully selected core team of anaesthetists represented our service to provide a consistent point of contact. Whenever there was the opportunity, geriatrics, surgeons, anaesthetists and case managers reviewed patients by the bedside to openly discuss crucial decisions forthwith. As collaborative technologies proliferate during the pandemic, we plan to use virtual platforms to remotely conduct multi-disciplinary discussions of complex cases.
We celebrated small wins and gave due acknowledgement to key stakeholders during regular departmental meetings. By broadcasting the positive results of our project, the culture in the department gradually changed to embrace the service. This helped to overcome the original inertia for change especially with varying degrees of enthusiasm towards perioperative care among anaesthetists.
Interpretation
Postintervention, anaesthesia consult timings improved significantly, likely due to multi-disciplinary collaboration, an emphasis on communication and a revised workflow designed to ensure standardised anaesthesia assessment on presentation of hip fracture rather than decision for surgery. Timings to surgery also showed an improvement generally; a lack of power may explain why it was not statistically significant. Instead its clinical importance is demonstrated by the reduction in 6-month and 12-month mortality and ICU admissions. In addition, nerve blocks to optimise pain were expedited with greater facilitation from our service. Hence, we hope to qualify how our service may improve care globally with respect to timeliness, effectiveness, efficiency and safety.
We would like to consider some points when discussing how early anaesthesia consult relate to timing of surgery: (a) there is an element of temporality with anaesthesia consult preceding surgery; (b) it is also a plausible concept that by triaging cases early, our service gives the ‘green light’ to surgeons to operate as soon as patients are ready; (c) bringing forth earlier anaesthesia reviews may help concentrate on issues for preoptimisation to expedite surgery; (d) with greater attention and an element of Hawthorne effect, parties were willing to proceed with high-risk cases being assured patients were already maximally optimised.
However, beyond just anaesthesia-related factors, surgical delays are multi-faceted with a diversity of contextual variables and confounders as explored below:
Human factor: despite standardised workflows and guidelines, it is unavoidable to have inter-individual variability of values and perspectives among the perioperative team guiding decisions for surgery especially for high-risk patients. We regularly encouraged the culture of open platform discussions to calibrate standards within the team to ensure consistent care was delivered.
COVID-19 pandemic: while our hip fracture caseload was fairly stable during the pandemic, the need for COVID-19 screening and isolation may be a factor in delaying surgery. This made up 8.5% of the delayed cases in 2020 at the start of the pandemic and reduced to 2.9% by mid-2021. While frequent changes in hospital infection control guidelines may have impacted access to surgery globally, restrictions on elective surgeries at the peak of the pandemic may have indirectly freed surgeons up to clear hip fracture surgeries instead.
The ‘weekend’ effect: cases admitted over the weekend had delayed preoptimisation and potentially poorer outcomes.11 In our institution, weekend admissions made up approximately 5% of delayed cases in 2020 and 2021. With our service limited to weekdays only, weekend admissions will only get seen by our service earliest on a Monday. Occasionally, cases could still proceed out-of-hours with the discretion of the emergency on-call team, although not a formal coverage of our service due to the variability of resources.
Access to OT space: a dedicated daily trauma list is recommended.12 However with constraints of theatre space, we were flexible in performing cases whenever the opportunity arose in elective or emergency theatres. Such adaptability played a main factor in expediting surgery, but was subject to manpower and resources.
Wait times for admission: the median wait times for admission fluctuated from 6 hours in 2019, dropping to 4 hours in 2020 and increasing to 7 hours by mid-2021. By 2021, we already evolved to be a mobile outreach team which addressed delays in review due to delays in admission.
The bottom line is while improving things locally within our department may have some impact, we still need to continue our holistic multidisciplinary approach in addressing the bigger picture.
Limitations
We cannot fully exclude biases in data collection, reporting and interpretation of results. Another challenge is ensuring accuracy of data within the limits of existing electronic databases. Prior to 2019 anaesthesia documentation was primarily from paper charts making data retrieval challenging.
Evaluating the contributions of various elements of perioperative care to surgical outcome is neither straightforward to measure nor exhaustive. As we evolve, we plan to study more patient-centred outcomes—patient satisfaction of care, prolonged fasting, complications (eg, delirium, thromboembolism, cardiac events) as patient-centred outcomes; surgical cancellation as a performance indicator; shortage of manpower for other anaesthesia services as a balance measure. Recommendations for Core Outcomes for Measures for Perioperative and Anaesthetic Care to guide outcome selection in future studies was recently published.13 It was not available when we first developed this project but will certainly look to it in the future.
Limits to generalisability: innate variables in health, race and socioeconomic circumstances may impact baseline risks and choice of surgery. Hip fracture pathway criteria varies in different hospitals. Case mix and patient numbers may change with time which impacts availability for theatre space. Differing manpower allocations and priorities exist so not all anaesthesia departments would put as much of an investment in perioperative care as we did. It took a great mindset to transition to a consultant-only led service when traditionally routine preoperative assessment was done mainly by junior staff. We decided to assess the patients upstream, way before the surgical consent was made at times, which breaks the convention of assessing the patient only after decision for surgery is finalised. Unlike other institutions, critical care, pain and regional services are shared among a common pool of anaesthetists in our hospital, streamlining communication and handover once a system was in place.
Conclusion
Our QI project sets out to address surgical delays by forming a consultant-led outreach anaesthesia service to provide proactive anaesthesia care in advance of surgical decision with emphasis on greater standardisation in workflows, communication and quality assurance. With our successful implementation, we have already scaled our model of perioperative care to other microsystems within our department and do intend to expand to others. For successful scalability, we endeavour to adopt a framework for spread that aligns with hospital-wide culture and priorities. Nonetheless, with the right people, process and support, we demonstrated our service is useful not just as a small fragment in a puzzle, but as a cogwheel driving big changes in perioperative outcomes downstream.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to acknowledge the following for their unwavering support and help: collaborative support from the ValueCare hip fracture pathway team (lead by Dr Adj Asst Professor Andy Yeo and Orthopaedic department), Orthogeriatrics (lead by Dr Goh Kiat Sern and team) and case managers (lead by Nurse Clinician Ms Wang Ping and team). The guidance and support from Chairman, Medical Board of Changi General Hospital, Adj Associate Professor Siau Chuin. The strong encouragement and combined team effort from the Department of Anaesthesia and Surgical Intensive Care, Changi General Hospital, which also includes critical care, regional and pain services. The Office of Improvement Science and Performance Excellence in Changi General Hospital. Last but not least, the rest of the perioperative anaesthesia team with their invaluable experience in multiple anaesthesia subspecialties, in which this service would not be possible without our collective spirit and investment. (In alphabetical order, Dr Avinash Gobindram, Dr Jessica Malanjum, Dr Lydia Li, Dr Ong Ee Teng, Dr Tham Huae Min and Dr Zhang Xin Yan.)
Footnotes
Contributors WSS and CLM contributed to the planning, conduct and reporting of the work described in the article and are both responsible for the overall content as guarantors. LT contributed to the collection of data, ensuring data is cleaned, analysed and up to date, and also drafted and reviewed the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.