Article Text

Abstract
Background Appreciative Inquiry is a motivational, organisational change intervention, which can be used to improve the quality and safety of healthcare. It encourages organisations to focus on the positive and investigate the best of ‘what is’ before thinking of ‘what might be’, deciding ‘what should be’ and experiencing ‘what can be’. Its effects in healthcare are poorly understood. This review seeks to evaluate whether Appreciative Inquiry can improve healthcare.
Methods Major electronic databases and grey literature were searched. Two authors identified reports of Appreciative Inquiry in clinical settings by screening study titles, abstracts and full texts. Data extraction, in duplicate, grouped outcomes into an adapted Kirkpatrick model: participant reaction, attitudes, knowledge/skills, behaviour change, organisational change and patient outcomes.
Results We included 33 studies. One randomised controlled trial, 9 controlled observational studies, 4 qualitative studies and 19 non-controlled observational reports. Study quality was generally poor, with most having significant risk of bias. Studies report that Appreciative Inquiry impacts outcomes at all Kirkpatrick levels. Participant reaction was positive in the 16 studies reporting it. Attitudes changed in the seventeen studies that reported them. Knowledge/skills changed in the 14 studies that reported it, although in one it was not universal. Behaviour change occurred in 12 of the 13 studies reporting it. Organisational change occurred in all 23 studies that reported it. Patient outcomes were reported in eight studies, six of which reported positive changes and two of which showed no change.
Conclusion There is minimal empirical evidence to support the effectiveness of Appreciative Inquiry in improving healthcare. However, the qualitative and observational evidence suggests that Appreciative Inquiry may have a positive impact on clinical care, leading to improved patient and organisational outcomes. It is, therefore, worthy of consideration when trying to deliver improvements in care. However, high-quality studies are needed to prove its effects.
PROSPERO registration number CRD42015014485.
- Quality improvement
- Organizational Culture
- Quality improvement methodologies
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Appreciative Inquiry has been successfully used for organisational change outside of a healthcare setting for three decades.
Changes in healthcare environments as a result of Appreciative Inquiry have been reported, for example, changing processes, defining services and improving the working environment.
What this study adds?
We draw on a global evidence base to systematically consider the outcomes reported in Appreciative Inquiry studies to evaluate its effectiveness.
We show that while the empirical effectiveness of Appreciative Inquiry is unclear, the qualitative and observational data suggest that Appreciative Inquiry could be a positive organisational change technique.
How this study might affect research, practice or policy?
We would like to encourage those interested in healthcare improvement to consider Appreciative Inquiry approaches for their organisational change initiatives.
We present the myriad ways that Appreciative Inquiry can have impact within a healthcare environment and encourage implementers/evaluators to use this framework to systematically consider all of these areas to document and report their Appreciative Inquiry studies/projects.
Introduction
Healthcare organisations are under pressure to improve the quality and safety of their services.1 One action cycle method for improving quality and safety is Appreciative Inquiry .1 2 Outside of healthcare, the benefits of Appreciative Inquiry have been widely described and include increased profits, reduced absenteeism and improved customer service.3 Appreciative Inquiry in the healthcare setting has been less well documented2 although its popularity is growing.1 4
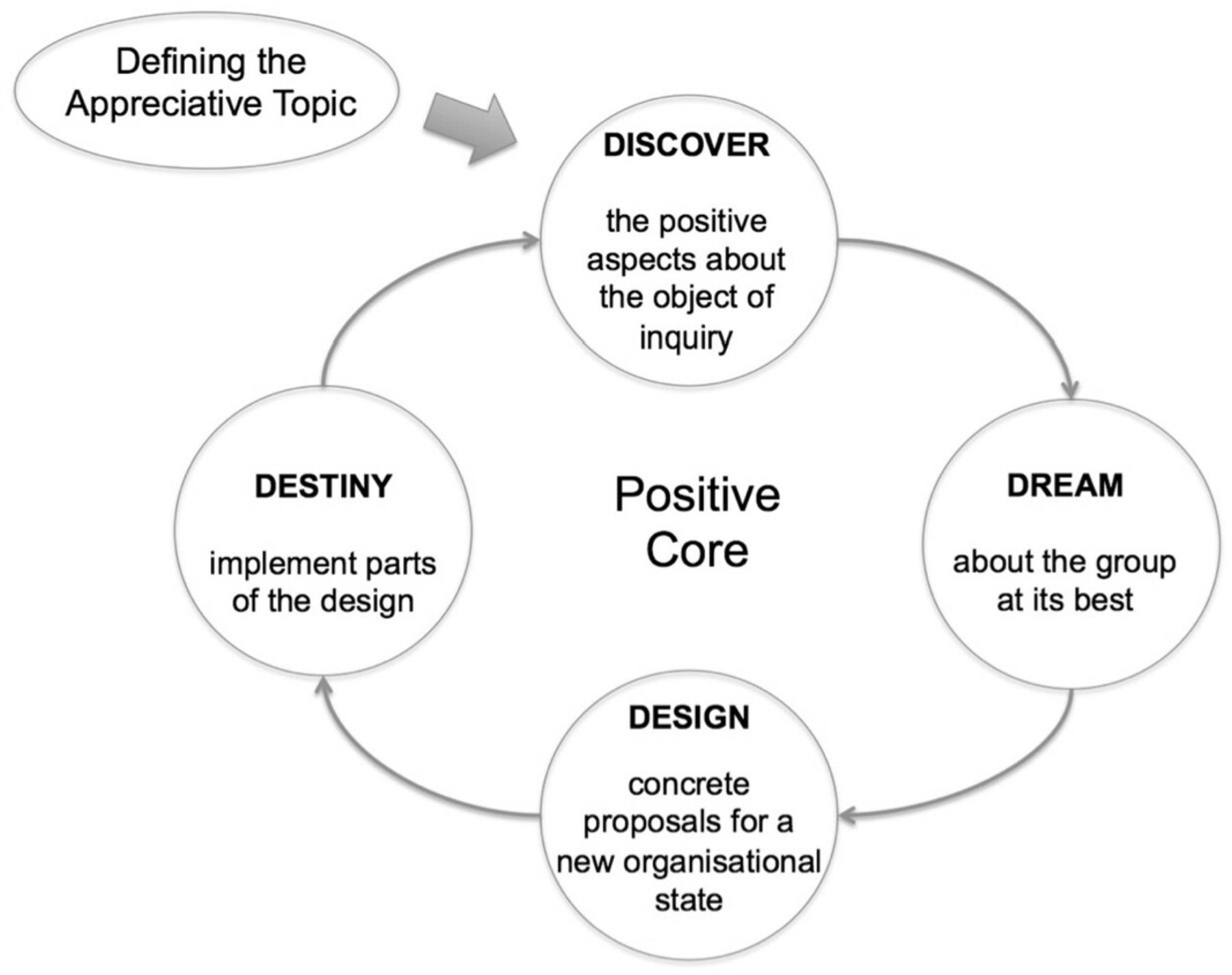
Appreciative Inquiry is a philosophical approach that seeks to harness the unique creativity of organisations, focusing on strengths, rather than becoming defensive and problem focused.5 6 It encourages new thinking, improvisation and aims to achieve transformational change.7 Appreciative Inquiry investigates the best of ‘what is’ before thinking of ‘what might be’, deciding ‘what should be’ and finally experiencing ‘what can be’.5 There is no ‘fixed’ method, Appreciative Inquiry is grounded in some ‘principles’. However the ‘4D cycle’ has emerged as the leading framework (figure 1).5

The Appreciative Inquiry Cycle.
A practical example of the use of Appreciative Inquiry in a healthcare context can be taken from an Indian study.8 9 Using the 4D cycle, in the ‘Discovery’ phase, they arranged meetings with hospital staff, where experiences of saving lives in childbirth were shared and celebrated. Staff then interviewed each other. Following feedback, the ‘Dream’ phase facilitated staff to develop aspirations. The overarching one was to be ‘the best hospital for infection control’. In the ‘design’ phase, they developed measurable and achievable action plans. In the ‘destiny’ phase, they discussed ways to sustain their plans and continue the good work.8
A systematic review2 of Appreciative Inquiry in healthcare showed a breadth of issues being addressed but did not fully evaluate the effects. A more recent review of Appreciative Inquiry in nursing practice concluded that Appreciative Inquiry was often implemented without attention to its pivotal components, but instead a ‘sanitised’ version of the 4D cycle was used.4 This review will focus on whether Appreciative Inquiry is able to improve healthcare.
Methods
Appreciative Inquiry is a complex intervention; therefore, heterogeneity between studies in terms of the intervention, study design and outcomes was expected. Narrative synthesis was selected10 to flexibly identify, include and synthesise diverse studies.11
Data sources
A search of major electronic databases (Medline, Embase, Cochrane collaboration, PsychINFO, Sociological Abstracts, Allied and Complimentary Medicine Database, British Nursing Index, Health Management Information Consortium, Health Business Elite and CINAHL) from 1987, until 8 December 2020, was undertaken. Grey literature was identified using Eldis, UK Data Service and websites of quality improvement and development organisations. Experts were contacted and reference lists of included studies and review papers were screened. Search terms were ‘appreciative’, ‘4D cycle’, ‘transformational’ and ‘non-punitive’ in titles and abstracts. This approach was inclusive, and though would generate a large number of records, would ensure that relevant studies were not missed.
Study selection
Included studies were of any design, but the intervention must have been described or referenced. We included studies of all quality to provide the fullest picture of the real-world implementation of Appreciative Inquiry. We report the study quality and draw conclusions in line with the quality of available evidence. There were no limits on language or country/region studied. Participants included healthcare/allied healthcare staff, delivering direct clinical care. The Appreciative Inquiry interventions could also include healthcare administrators, managers, patients and students.
Studies were not eligible for inclusion if Appreciative Inquiry was being targeted solely at participants not involved in clinical care or if there was no description of the intervention or any of the outcomes of interest.
Data extraction
Two authors screened studies, a third was consulted in cases of disagreement. A data extraction proforma captured the outcomes and study methodology (online supplemental file 1). Two authors extracted data and any discrepancies were resolved by consensus. The contribution of each study to the synthesis was discussed by two review authors who also agreed the quality of the study using a ‘weight of evidence’ assessment tool12 supplemented by the guidelines from the EQUATOR Network (http://www.equator-network.org/). A study was considered high quality if only two to three items on the relevant EQUATOR criteria checklist were dropped. Risk of bias assessment was performed for RCTs using the Cochrane risk of bias tool and the Newcastle Ottawa scale for observational studies.
Supplemental material
Analysis
A preliminary synthesis used tables and a short textual description of each study. This allowed common themes to be developed and outcomes grouped.
The Kirkpatrick framework was used to group the outcomes of Appreciative Inquiry. It was originally developed to categorise outcomes in educational interventions. The version used here provides greater detail than the original version to enable a better understanding the effectiveness of interventions. The elements include reaction of participants; modification of attitudes/perceptions; acquisition of knowledge or skills; behavioural change; change in organisational practice; benefits to patients/clients.13 These categories are used to discuss the available evidence for whether Appreciative Inquiry works.
This study protocol is registered with PROSPERO and this study is reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Only the effectiveness of Appreciative Inquiry is reported in this paper. Patients and public were not directly involved in this review.
Results
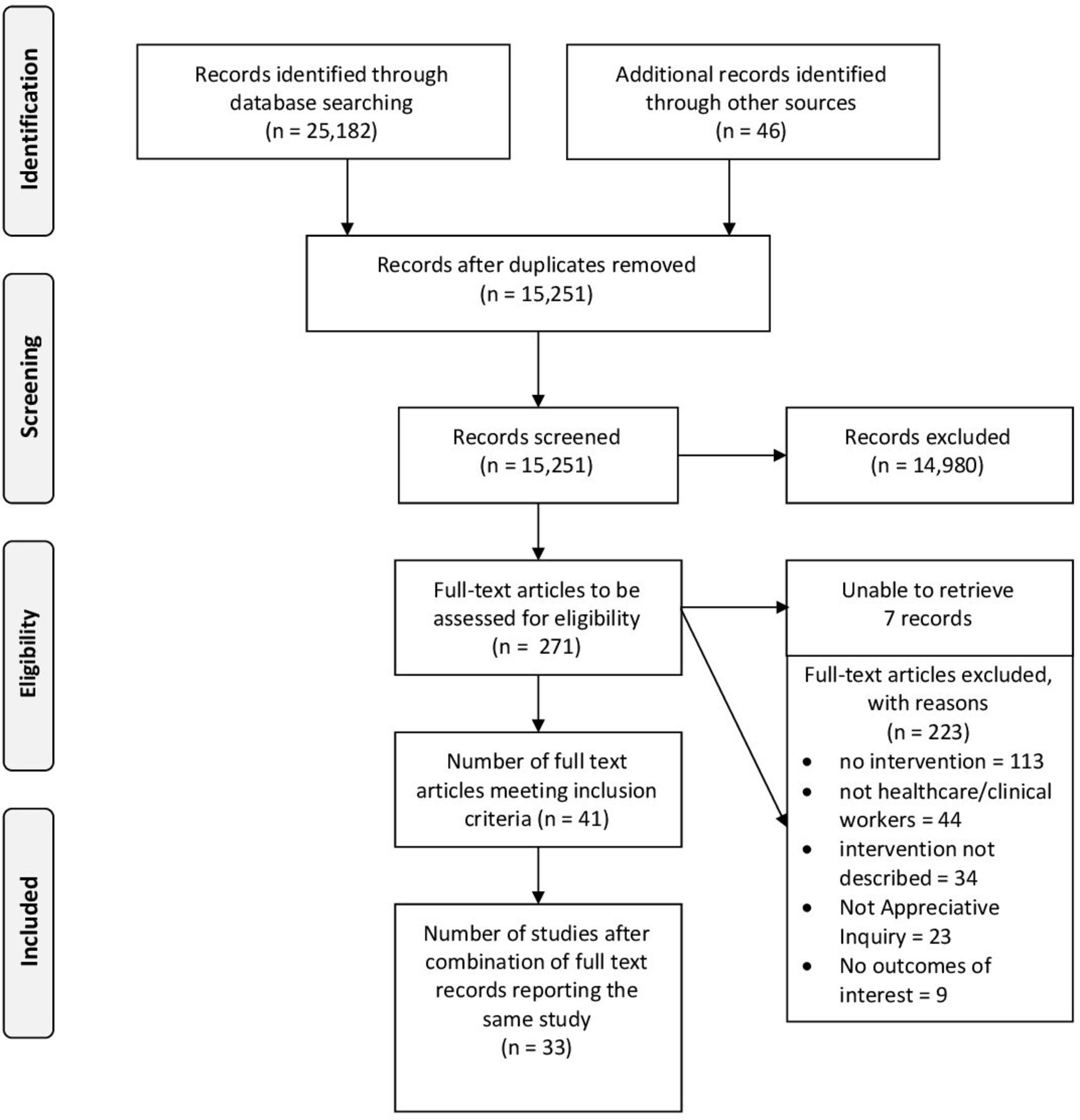
From 25 182 citations, there were 15 215 titles after deduplication. Following screening 41 papers were eligible for inclusion which report 33 studies. The process and reasons for exclusion are shown in the PRISMA diagram (figure 2). For those not reaching full-text screening, reasons for exclusion were mainly because studies were not about Appreciative Inquiry or healthcare. Online supplemental file 2 summarises each study and shows which records are related to each study. Throughout the Results section, all records of studies discussed will be referenced; therefore, where there is more than one record, both of these references will appear.
Supplemental material
{kind=link}
{kind=link}
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The weight of evidence attributed to each study is presented in online supplemental file 2. There are no high-quality randomised controlled trials of this intervention nor are there any other high-quality quantitative studies. There are, two well-conducted qualitative studies.14–16 Despite this, the included studies are highly relevant to the review.
A summary of results is presented in table 1. Due to the number of studies, it is not possible to give detailed examples from each; therefore, an exemplar of the evidence for each of the Kirkpatrick areas will be discussed.
A summary of the results containing examples of evidence according to Kirkpatrick areas
How do healthcare workers react to Appreciative Inquiry?
Sixteen studies report a largely positive reaction to Appreciative Inquiry.14–33 Staff found it enjoyable, refreshing and lively. When looking at the higher quality studies,14–16 18–21 these positive experiences are also reported. One high-quality study raises the issue that attending Appreciative Inquiry sessions is challenging.20 21 Three lower quality studies also contribute accounts, which are not wholly positive.25 32 33 However, all studies report that staff engaged with the process. Appreciative Inquiry allowed staff to reflect on their role, in one study a nurse reported that ‘I now remember why I became a nurse’.22
The four studies that reported negative reactions discussed how staff found it difficult to maintain attendance20 21 or to make time for Appreciative Inquiry activities.25 One study observes that Appreciative Inquiry does not work all of the time,32 and this is reflected in another study where they are unsure whether Appreciative Inquiry is effecting change.33
Despite some conflicting reactions, the available evidence suggests a positive participant reaction to Appreciative Inquiry, although due to the quality of these studies, the strength of this evidence is weak.
Does Appreciative Inquiry change the attitudes of staff?
Seventeen studies reported a positive change in staff attitudes.6 7 17 18 21 23–25 27 29–41 Over half focus on healthcare practitioners understanding each other better, team working and creating common ground.6 7 17 18 23 32–34 36 37 39 41 The higher quality studies support these results. There is discussion of improved self-esteem9 and developing a shared purpose.34 One medium-quality study describes a powerful image of a ‘pathbreaking experience’ for the cleaning staff, who sat on the floor at an equal level with their superiors, which was a ‘highlight of their service’.18 19
Other outcomes include desire to gain knowledge and provide consistent care36; desire to embrace change22 39; feeling empowered and enthusiastic25 and increasing motivation and professional self-confidence.30–32
The studies report positive changes in attitude; however. the strength of evidence for this is weak.
Does Appreciative Inquiry improve the knowledge and skills of healthcare workers?
Fourteen studies report6 7 13–16 19 20 23 32 38 40–47 improvements in knowledge and skills, but this was not universal. There were two studies with quantitative measures of knowledge, one of which was high quality. Both showed an increase in knowledge scores following the implementation of Appreciative Inquiry.17 20 21 However, one element of the low-quality study,17 the group learning, was poorly implemented, and knowledge scores for this element did not increase.
A common theme was understanding of the needs of patients and families.16 42–45 48 In one study, parents in a neonatal unit shared how they wanted to be treated, including being seen as important, being involved in their baby’s ‘firsts’ and fathers being more involved.16 Healthcare practitioners developed a better understanding of the system and how it works.14 15 24 33 Other studies reported new knowledge around performing good handovers47 and understanding what factors contributed to nursing longevity.46
The quantitative evidence for Appreciative Inquiry improving knowledge and skills is equivocal, based on two studies one of which is poor quality. The remaining evidence, although weak, suggests that knowledge and skills can improve using Appreciative Inquiry.
Does Appreciative Inquiry facilitate behaviour change?
Thirteen studies reported behaviour change of staff,4 8 9 20 21 23 24 28 32 34 36–38 41 43 44 49 50 including three in a quantitative way.20 21 23 41 The highest quality study was a controlled study, which showed no change in pain score of the patients.20 21 The other two studies were lower quality. One used a survey to ask about whether staff changed their behaviour in terms of discussing clinical risk: 70% felt it had improved.23 In the final study, a teamwork survey showed that the teams were performing well; however, there was no pre-intervention or discriminatory questions about the change in behaviour.41
The remaining 10 studies reported behaviour change qualitatively.6 7 23 31 33 35–37 42–44 48 49 In the highest quality study, improved teamwork resulted in better allocation of work, clear responsibilities and changes in individual practice. The medium-quality study reported how a team developed action steps.34 Other studies contributing evidence were of low quality. One reported 92% of commitments to change were implemented.36 Five studies observed that staff changed their interactions with patients.24 36 43–45 49 50 Examples of this include nurses increasing the frequency and consistency of oral care in a rehabilitation hospital36 and nurses doing hourly rounding to ensure patient’s needs (eg, toileting and comfort) are met.49 Communication also featured. One study reported improved communication and appreciation of staff37 38 and another discussing altered interactions with human resources.28 One study reported that nurses took more initiative and that cleaners worked harder to keep surroundings clean.32
While there is no high-quality evidence for Appreciative Inquiry resulting in behaviour change, the evidence that is available suggests that change does occur, although it is weak.
Does Appreciative Inquiry lead to organisational change?
Twenty-three studies describe organisational change8 9 14 15 18 19 22–24 26–29 34–39 41 43–51, six measured it.22 23 34 35 37 38 46 The medium-quality randomised controlled trial measured preventative service delivery score, in primary care practices. The study showed no change.34
The remaining studies were of low quality. One controlled study showed improved delivery of patient care through nutritional assessment by 11% and adherence to cardiac enzyme regimens increased by 9.2%. There was increased nursing satisfaction and teamwork.35 A non-controlled study identified that 30% of staff felt that clinical decision-making had improved.23
Retention and recruitment were discussed in three studies; in one of the controlled studies, turnover decreased from 10.35% to 8.42%, with vacancy rate decreasing form 6.2% to 4.1%.22 One of the non-controlled studies showed a decreased staff turnover by 3% and sickness by 2%; however, this could represent normal variation.37 38 Finally, the vacancy rate fell from 12.1% to 8.9% in another non-controlled study.46
Other studies made observations about changes that were implemented. The highest quality study discussed the introduction or improvement of regular staff meetings across the sites.8 9 The medium-quality studies report new staff activities, systems34 and improved surroundings.18 19
Some areas of change were described in multiple studies: altered patient care pathways or protocols26 34 35 47 50; new mechanisms for delivering care14 15 24 26 48; positive interactions with Human Resources22; staff meetings were initiated or altered8 9 23 24 26 36 51 and staff education or training was improved.29 39
The trial did not show quantitative evidence of organisational change. The controlled studies showed that Appreciative Inquiry can change organisational practice and qualitative studies and non-controlled studies, which report on organisational practice, reported positive changes. While the evidence is weak, it does suggest that Appreciative Inquiry has the potential to improve organisational practice.
Does Appreciative Inquiry lead to improved patient outcomes?
Of the eight studies reporting patient outcomes,8 9 18–21 29 35 49 50 52 four were high/medium-quality controlled studies8 9 18–21 and four were low-quality non-randomised studies.29 35 49 50
Of the higher quality studies, the controlled study in India, aiming to reduce puerperal infection rates, followed up 8124 women. It revealed decreased incidences of infection in the control (7.4% to 3.5%) and intervention (4.3% to 1.7%) groups; although the levels in the intervention group fell more, this was not statistically significant. However, this was on a background of a decreased infection rate in both groups and a larger percentage point decrease in the control group, and, therefore, firm conclusions are difficult to draw.8 9 Another controlled study which measured pain intensity scores in a paediatric ward showed no difference.20 21 A medium-quality study aimed to improve leprosy detection and false-positive rates. They saw a reduction in the false-positive rate of −9% (95% CI −20 to 1.3).52 This suggests that there is no strong evidence to support Appreciative Inquiry being effective.
Another higher quality study and the three lower quality ones report on patient satisfaction scores. A controlled study from India found that 89% of patients were satisfied with the care pre-intervention and 96% after. They also saw a 28% improvement in patient-reported attentiveness of staff and a 20% improvement in patients feeling that staff had treated them well. The control group remained stable.18 19
One lower quality controlled study measured patient satisfaction in a US hospital with a focus on cardiac patients. Patient satisfaction with care improved by 10.2%.35 Another that reported improved satisfaction was a case study of a health system in the USA. Their scores improved by 37%.29 The final study reported that more patients would ‘definitely’ recommend the hospital to a friend after the study (74.4%) compared with before (68.9%).49 These studies did not report on measures of spread.
One low-quality study reported the impact of the intervention on carers.50 89% felt involved in care planning post-intervention compared with 66% before, and carers felt consulted about decisions in 100% of cases post-intervention compared with 92% before, although no confidence intervals are provided.50
In summary, five studies, one medium-quality and three low-quality showed improvements in patient satisfaction, and one showed improved involvement in decision-making. The three higher quality studies showed no significant changes. The evidence contributing to this is not persuasive as it is neither of high quality nor consistent. The lower quality studies do suggest that there may be a trend towards improvement in patient care following Appreciative Inquiry; however, the evidence for any improvement is weak.
Discussion
We identified 33 studies using Appreciative Inquiry to change clinical care. The majority were small change initiatives, lacking methodological rigour. Appreciative Inquiry as an approach to improve the quality of healthcare and patient safety is in its infancy but, despite weak evidence of its effectiveness due to the low-quality of studies, the positive reports suggest it warrants more rigorous evaluation.
An important consideration is the philosophy of Appreciative Inquiry,5 with the idea that the world is open to constant revision, which is not immediately congruent with positivist methods of evaluation such as randomised controlled trials. Consistent with this incongruence, we only identified one trial that met the inclusion criteria for this review,34 and one further healthcare trial that did not.53 It is more likely that action research approaches would favour evaluation methodologies rather than clinical trials, and this may be one reason for the small number of controlled studies.
Patient satisfaction is one area which Appreciative Inquiry could plausibly affect because it may foster changes at an interpersonal level. Analysis of Appreciative Inquiry in other settings has suggested that both the process (eg, the discovery phase) and the philosophy (the unconditional positive question) shape the relationships that are formed and through this discourse relationships can flourish.54 This is supported by our recently published study focusing on improving staff working lives using Appreciative Inquiry where relationships and patient experience improved.55
In terms of patient outcomes, there is some promising evidence for the use of Appreciative Inquiry from a study of infection control measures,8 9 although the study was underpowered, and from a leprosy study in India.52 The only other study on pain management in paediatrics looking at patient outcomes reported no change during the study.20 21 However, for patient outcomes, there are three key issues: whether the Appreciative Inquiry is aiming to affect change in this area, whether the intervention actually affects change, and if it can be accurately measured. Many studies did not attempt measurement. Sample sizes were too small to demonstrate or attribute change to the intervention, nor may it be possible to attribute change in patient outcomes to a complex intervention.56 Furthermore, for predefined patient outcomes to be measured, the focus of the Appreciative Inquiry needs to be predetermined. This could reduce its effectiveness, as participants may not be focusing on what is important to them, instead focusing on a more conventional change process. A broad analysis of Appreciative Inquiry methods has shown that when this happens, change due to Appreciative Inquiry is less likely to be transformational.57 Methods which were used in studies in this review to incorporate this included allowing the team to choose its own idea first34 and introducing best practice guidelines as part of the process.36
Finally, interventions need time to embed, so longer study durations may be required. When considering evidence from social work, interventions can take 2–4 years to implement.58 This is similarly modelled when considering the evidence-to-practice gap in healthcare.59 Considering Appreciative Inquiry specifically, we have shown on a small scale in our recent paper, how organisations take up interventions in different ways.55
There is no clear evidence to suggest that Appreciative Inquiry can change patient outcomes. However, it seems unlikely that it will cause harm to patients, and there is some promising, although poor-quality and inconclusive evidence for its use.
The evidence for Appreciative Inquiry changing the way organisations work is more convincing and plausible considering evidence from outside of healthcare.7 Changes included reduced staff turnover, sickness and altered protocol adherence. However, success was not universal. Many studies reported changes such as morale improvement activities, altered human resources policies and new patient care pathways. While these were not captured in a quantitative manner, their introduction impacts organisational practice and may go on to affect measurable outcomes.60
There is some evidence to suggest that behaviour change is possible with Appreciative Inquiry. Appreciative Inquiry seemed to produce positive outcomes for knowledge and skill development, with the two studies which measured this outcome quantitatively showing improved knowledge, with other qualitative reports of changed behaviour. Attitudes changed following Appreciative Inquiry, particularly teamwork, understanding each other and communication.
Appreciative Inquiry is reported in a largely positive light, with few negative findings. This may be because the ethos is to focus on the positive and authors are often synonymous with the implementation team. This reporting bias may result in overly positive accounts of Appreciative Inquiry. An additional weakness of the available literature is publication bias. It is unlikely that negative findings of Appreciative Inquiry interventions would be published outside of a rigorous evaluation, adding to the positive slant on the literature.
Another influence is that Appreciative Inquiry is often instigated for quality improvement rather research. Most of the studies capture qualitative data or are reports of real-life implementation, with few studies systematically collecting outcome data. While this may have positives, for example, the organisation being committed to change, it makes interpretation of the impact of Appreciative Inquiry difficult. Nonetheless, from the limited evidence available, Appreciative Inquiry does seem to bring about change within organisations and the Kirkpatrick model helps in illuminating this.
The Kirkpatrick framework was not designed for organisational change studies, and, therefore, it is not perfect. For example, it does not consider the implementation or context of the intervention.61 However, it was a useful framework to consider heterogenous outcomes.
The current evidence of the effectiveness of Appreciative Inquiry is not conclusive, with a lack of empirical evidence for process or clinical outcomes. The studies identified in this review suggest that Appreciative Inquiry has the potential to effect positive change for patients and organisations. It could, therefore, be particularly useful in the context of the needing to improve quality and safety of a service. However, to draw firm conclusions about the effectiveness of Appreciative Inquiry, high-quality studies are required.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @abimerriel
Contributors AMe conceived the study, AMe/JH/ML/ACoo refined the question and planned methodology, KB ran searches, AMe/AW/ED/MOD screened and extracted data, AMe performed initial analysis, ALL contributed to interpretation, AMe wrote the first draft of the paper, ALL critically contributed to the final draft. AMe is the guarantor for this study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.