Article Text

Abstract
Background For the design of a robust quality system for hospital-based physiotherapy, it is important to know what key stakeholders consider quality to be.
Objective To explore key stakeholders’ views on quality of hospital-based physiotherapy.
Methods We conducted 53 semi-structured interviews with 62 representatives of five key stakeholder groups of hospital-based physiotherapy: medical specialists, hospital managers, boards of directors, multidisciplinary colleagues and patients. Audio recordings of these interviews were transcribed verbatim and analysed with thematic analysis.
Results According to the interviewees, quality of hospital-based physiotherapy is characterised by: (1) a human approach, (2) context-specific and up-to-date applicable knowledge and expertise, (3) providing the right care in the right place at the right time, (4) a proactive departmental policy in which added value for the hospital is transparent, (5) professional development and innovation based on a vision on science and developments in healthcare, (6) easy access and awareness of one’s own and others’ position within the interdisciplinary cooperation and (7) ensuring a continuum of care with the inclusion of preclinical and postclinical care of patients.
Conclusions Important quality aspects in the perspective of all stakeholders were an expertise that matches the specific pathology of the patient, the hospital-based physiotherapist being a part of the care team, and the support and supervision of all patients concerning physical functioning during the hospitalisation period. Whereas patients mainly mentioned the personal qualities of the physiotherapist, the other stakeholders mainly focused on professional and organisational factors. The results of this study offer opportunities for hospital-based physiotherapy to improve the quality of provided care seen from the perspective of key stakeholders.
- healthcare quality improvement
- qualitative research
- hospital medicine
Data availability statement
Data are available upon reasonable request. The raw data of this study are available from the first author at request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
To our knowledge, this is the first study on quality aspects of hospital-based physiotherapy according to its main stakeholders (outside-in perspective).
What this study adds
Seven quality themes emerged from the data analysis, which characterises the quality of hospital-based physiotherapy from the perspective of key stakeholders.
How this study might affect research, practice or policy
The results of this study offer opportunities for hospital-based physiotherapy to improve the quality of provided care. With a better understanding of what key stakeholders expect, a quality policy can be worked on more effectively and efficiently, which strengthens the positioning of a hospital-based physiotherapy department within the hospital organisation.
Introduction
In the organisational structure of a hospital, the position of a hospital-based physiotherapy department can be seen as that of a service-providing or cost centre. A department within an organisation that does not directly add to profit but costs the organisation money to operate. The department delivers a service to a target group.1 To develop a high-quality standard of service, a target group centred strategy is needed. Such a strategy begins with defining the target group and its needs and wants.1 2 The key to delivering high-quality service is to balance stakeholders’ expectations and perceptions and to close the gap between these two aspects.3 Once the goals and perspectives of the stakeholders are understood, potential gaps in meeting their expectations can be explored and solved to ensure providing the required quality.4
Stakeholders can be seen as individuals, groups or organisations who have an interest (stake) and the potential to influence the actions and aims of an organisation, project or policy direction.5 6 Stakeholder analysis has been developed as a multipurpose tool in the fields of policy, management and project implementation. Its usefulness lies in its ability to highlight the importance of actors and interest groups in the policymaking process.7 Growing evidence indicates that stakeholder engagement in healthcare research contributes to increased relevance of outcomes for patients and stakeholders.8
In previous research into quality of hospital-based physiotherapy, we identified a set of 56 quality indicators, condensed into 7 quality themes, to describe and assess the quality of hospital-based physiotherapy from the perspective of hospital-based physiotherapists and their managers.9 However, it is also important to know what the main stakeholders of hospital-based physiotherapy consider quality to be. By identifying key stakeholders of hospital-based physiotherapy within the hospital, and including their views and opinions on quality of hospital-based physiotherapy, the quality policy of a physiotherapy department can be better targeted.
Whether the practice of care provided by hospital-based physiotherapists meets the criteria of desirable care and stimulates continuous quality improvement, an understanding of quality enriched with the views of key stakeholders within the hospital is required. The quality of the provided hospital-based physiotherapy care can be assessed with a quality system, and the alignment between performance, strategy, vision and desired outcomes can be established.10 Therefore, this study aims to explore key stakeholders’ views and opinions on quality of departments of hospital-based physiotherapy.
Methods
Design and setting
This qualitative study was conducted from October 2020 to June 2021 in three large Dutch hospitals, one academic and two teaching hospitals.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research. The results of the study will be disseminated to all participants and members of the NVZF (Dutch Association for Physiotherapy in Hospitals) during their annual congress.
Preliminary research
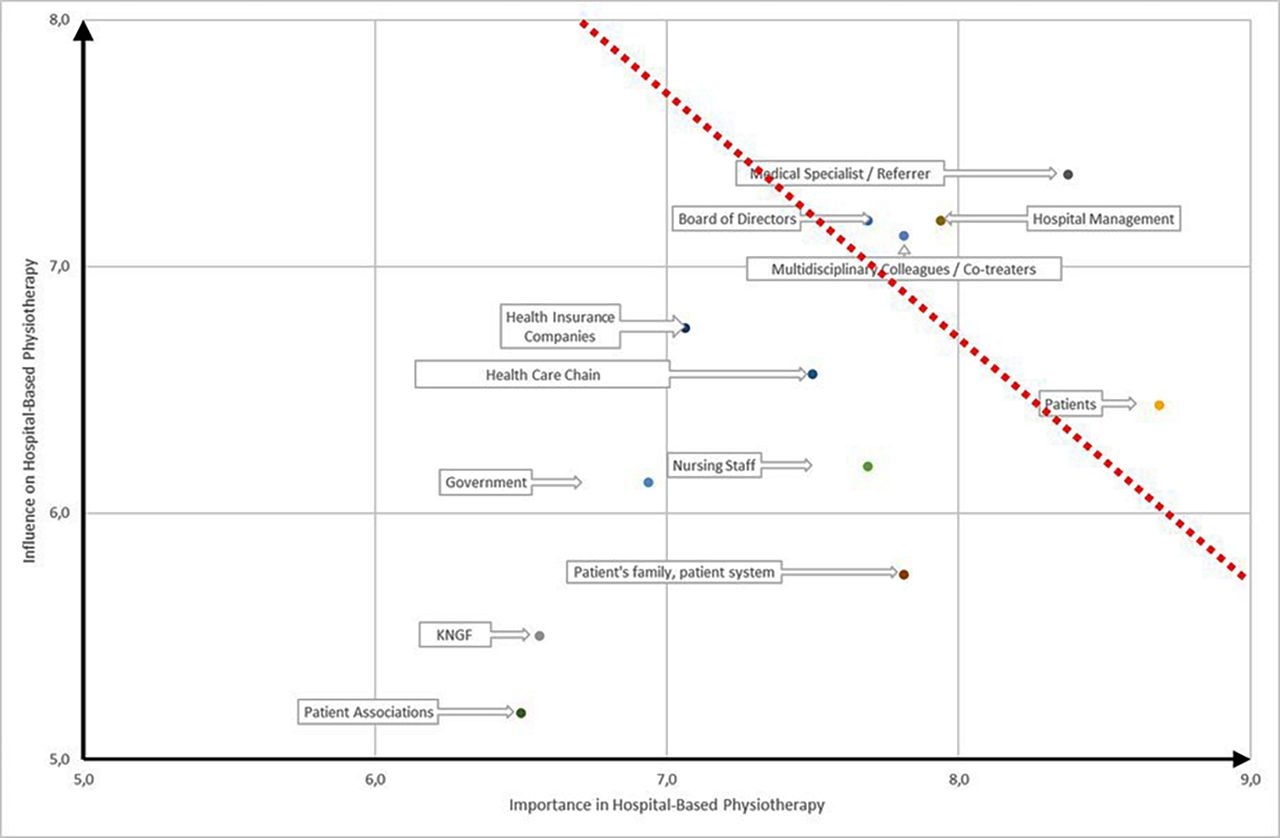
During our previous study,9 hospital-based physiotherapists and their managers were asked to list all stakeholders of hospital-based physiotherapy they considered important. Subsequently, they rated their importance in and influence on hospital-based physiotherapy, on a scale from 1 (minimal) to 9 (maximal). The average scores on the dimensions of importance and influence were plotted on the x-axis and y-axis in a stakeholder matrix (figure 1). Stakeholders from the quadrants with the highest scores on both axes were considered key stakeholders within the hospital. These included medical specialists (referrers), hospital managers, boards of directors, allied health colleagues and patients.

{kind=link}
Stakeholder matrix of hospital-based physiotherapy. Key stakeholders at the top right. KNGF, Royal Dutch Society for Physiotherapy.
Interviews
We planned interviews with each of the five key stakeholder groups in the three participating hospitals. In each hospital, a contact person from the physiotherapy department was recruited who coordinated the selection of and appointments with stakeholders in their hospital. Each potential candidate for an interview received an information letter about the study and an informed consent form. Inclusion criteria for members of the Executive Board were that they had allied healthcare as a focus area in their portfolio, for managers and specialists that they were at least among the top 10 largest referrers to physiotherapy within their hospital, and for multidisciplinary colleagues that they collaborated substantially with hospital-based physiotherapists. Patients were included when they had received at least three physiotherapeutic treatment sessions during admission and their admission period was no longer than 1 week ago.
All participants were interviewed individually. Exceptions for a group interview were made if there were several interview candidates within a stakeholder group at the same time. For every type of stakeholder, a specific topic list with interview guide for the semi-structured interview was drawn up by the authors (online supplemental appendix 1). Each topic list was piloted several times in test interviews prior to use in this study. Each interview was moderated by the primary researcher (RS), assisted where possible by the contact person of the respective hospital. To ensure that all items on the topic list were covered in each interview, no time limit was set for the interviews. Interviews were audio-recorded and transcribed verbatim.
Supplemental material
Analysis
Transcripts of the interviews were checked against the field notes by the interviewer and the contact person of the respective hospital when present. A thematic approach was used to analyse the transcripts.11 Three researchers (RS, LvH-S and GD) independently studied and inductively coded the transcripts by open coding. Differences in coding were discussed, and a codebook as well as a set of the most meaningful quotations were created based on consensus between the three researchers before the next set of transcripts was analysed. Saturation was achieved from the moment that list coding, instead of open coding, could be fully used via the codebook. Analysis of transcripts was supported by ATLAS-ti V.8.4.12 In the last step of the analysis phase, codes were thematically ordered and the themes found were finally categorised according to three organisational levels at which a hospital physiotherapy department can be viewed (ie, the hospital-based physiotherapist, the hospital physiotherapy department and the hospital).
Trustworthiness
To enhance trustworthiness, the whole research team, all experienced hospital-based physiotherapists and researchers, reviewed and consented with the identified themes and results as found by the three primary researchers. A member check by participants was also carried out. Participants received the preliminary findings and could, when desired, provide feedback on the accuracy of the researchers’ interpretation of the data. No substantive comments were received.
Reflexivity
During the study, we were aware of our positions and maintained a reflexive approach from our perspectives as experienced hospital-based physiotherapists and researchers (RS, LvH-S and GD), as a teacher of physiotherapy and experienced researcher (MM) and as (associate) professors in allied health and medical care and experienced researchers (TJH, PB and PvdW). We tried to obtain balanced and uniform data by having RS conduct all the interviews, supported by a local contact from the hospital in question. During data analysis we were always aware of conflicting codes, which we resolved in consensus. In correctly defining the codes and themes found, and in writing the manuscript, we carefully selected the appropriate language.
This study was reported following the Consolidated criteria for Reporting Qualitative research.13
Results
Sixty-two hospital employees and patients divided into five stakeholder groups were interviewed. Of the total of 53 interviews, 46 were individual and 7 were group interviews. Characteristics of the participants are presented in table 1.
Characteristics of participants
The most important quality aspects stakeholder groups reported are presented in table 2.
Important quality aspects per stakeholder group in rank order
The analysis of all interviews yielded a total of 129 quality aspects which could be classified under the following 7 quality themes (table 3).
Quality themes for hospital-based physiotherapy according to key stakeholders
Quality of hospital-based physiotherapy is characterised by a human approach
Mainly patients indicate that they expect a hospital-based physiotherapist with a human approach; a professional who is engaged and empathic, with respect for the needs and demands of the patient, stays calm and gives clear explanations and motivational instructions preoperatively and postoperatively. The care of the physiotherapist should be personalised and should provide safety and confidence according to patients and co-treating professionals.
If, for example, you have to move from the bed to the chair, that they remain calm and clearly tell you that this is what is going to happen and you cannot fall out, and so on, that is very important. (Patient 02)
The pep talk, you know with walking and so on, that they say well done, you are doing well, or you know, it is going fantastic, you know. Then you feel a bit of euphoria of, oh yes, well you know then it is going well, so then I think oh well I am doing my best and they see it. (Patient 03)
Quality of hospital-based physiotherapy is characterised by context specific and up-to-date applicable knowledge and expertise
According to patients, although they cannot verify this directly, the physiotherapist is expected to have professional knowledge and expertise. Medical specialists and hospital management, who are able to call on this knowledge and expertise directly, add that this expertise should match the specific pathology of the patient, providing more additional in-depth diagnostics. In this way, the physiotherapist can become an important sparring partner for the medical specialist in determining and implementing treatment policy. Or even take over parts of the medical work independently.
A good physiotherapist also has a signalling function, so he can also tell us: if this is what you have in mind, then I need this and that. Or that’s not feasible in this patient’s case. Or I see that it won’t work in the long run. So, to put it bluntly, a physiotherapist must not only blindly carry out what we prescribe. (Medical Specialist 03)
In some places, the physiotherapist takes over the role of the doctor, for example pelvic floor problems. Or the physiotherapist who participates in the hand centre. There, they are so specialised and differentiated that, based on their knowledge of functional movement, they take over a role from a doctor who only predominantly looks at it from a medical perspective. (Hospital Manager 01)
Quality of hospital-based physiotherapy is characterised by providing the right care in the right place at the right time
Availability of the right physiotherapist at the right moment was mainly mentioned by medical specialists and co-treating professionals, as well as having short communication lines with these colleagues. This is particularly to avoid unnecessarily prolonging the patient’s stay, often indicating that this could also mean continuing treatment in the evening hours or at the weekend. Hospital management adds the issue of whether a physiotherapist should be embedded in the allied health service or care department, to have more control on this process.
The availability or unavailability of the physiotherapist should not lead to longer hospitalisation times or longer recovery times for the patient. In other words, the patient should not have to stay in hospital longer because Pete or Jeff or Karen really cannot make it that day. (Medical Specialist 09)
Look, I can still see some disadvantages in the process, but that eh, look the hospital is a 24/7 company in principle. And, you often see that we are not always set up that way, so also the physiotherapy. There is physiotherapy at the weekend, but it is of a different intensity and that one physiotherapist has to treat more patients in a shorter time than during the week. Yes, I don’t think that’s continuity. (Hospital Manager 14)
Quality of hospital-based physiotherapy is characterised by a proactive departmental policy in which the added value for the hospital is transparent
Hospital management and medical specialists are looking for proactive physiotherapists, both at request and spontaneously, primarily ensuring that the hospitalisation period of patients is shortened. Physiotherapists contributing to the multidisciplinary care pathway, and delivering added value in projects and innovations, were also mentioned. The executive board likes to see the physiotherapist being a specialist in issues concerning physical functioning which affect the whole hospital, and a physiotherapy policy that dares to make result-oriented agreements with the organisation.
Then I expect a proactive attitude from the um, from the club physiotherapists. That there are sometimes requested, and sometimes unrequested modifications of the consultation. (Hospital Manager 05)
Physiotherapy is part of the treatment team that helps patients. The difference lies in the expert role regarding functional movement that is taken up by this team. In practice with patients, and also in the active participation in treatment policy, and daring to make outcome agreements concerning interventions within certain patient categories. (Executive Board 01)
Quality of hospital-based physiotherapy is characterised by professional development and innovation based on a vision on science and developments in care
From the perspective of what is best for their patients, medical specialists expect physiotherapy to adhere to the most recent guidelines and, where necessary, to conduct and to lead their own scientific research. Boards of directors and hospital management also expect this, but more from the perspective of business economics and patient satisfaction, by balancing scientific evidence and actual healthcare needs.
And now the physiotherapist as part of allied health care, supports the medical field, so to speak. And I think that in the future, it should be the other way round, with much more focus on healthy exercise, physical activity and nutrition. And then to consider what the medical specialist can still do for you. (Medical Specialist 12)
If you talk about academic physiotherapy, you have to emphasise the renewal and innovation of your training, but also the innovation of your professional field, and research is necessary for this. And also to look at what is evidence for and what is not. (Executive Board 03)
Quality of hospital-based physiotherapy is characterised by easy access and awareness of one’s own and others’ position within the interdisciplinary cooperation
Being an inherent part of the care team, giving support and supervision to all patients’ physical functioning during the hospitalisation period and supporting early mobilisation, was mentioned by medical specialists. Hospital management and the executive board expect an expertise regarding physical functioning in relation to daily practice of the patient. Interdisciplinary collaboration was mentioned by co-treating professionals, as well as the ability to identify one another based on an expertise within the care team, leading to a joint treatment plan for the patient.
Well, because at the moment the doctor is certainly not going to do all the exercises with the patient, and neither will the nurses. So, who is going to do it? So no, I think the physiotherapist is really an inherent part of running your department. (Medical Specialist 11)
Movement and mobility, how incredibly important that is for mental and physical recovery. And I think physiotherapists, because of their expertise, but also because of their practical attitude, are very, um, approachable for most of our patients and they can more easily make the link to daily practice. (Medical Board 02)
Quality of hospital-based physiotherapy is characterised by ensuring a continuum of care with the inclusion of preclinical and postclinical care of patients
Being visible as an integral part of the care team and the care pathway within the network of preoperative and postoperative care around the hospital, was seen as a key quality aspect by the board of directors, hospital management and medical specialists. This ensures a continuum of care, which extends beyond the admission. Important issues here are how to link with external physiotherapists, and how to ensure a proper transfer to other healthcare professionals.
I think continuity is important—and that is both preoperative and postoperative. What I think is important here, what I’m noticing now, is that you have to determine how you function in the network, so that you, how do you link up with peripheral or, indeed, external physiotherapists? I think that eventually, people leave the hospital, of course, and then you just don’t fall under hospital-based physiotherapy any more, so if there is a good transfer of this and also the other way round, I think that is an important factor. (Medical Specialist 07)
I think a huge added value for us is that the transition to primary care or to a rehabilitation centre or other institutions is seamless. That we simply deliver people well, so to speak. (Hospital Manager 06)
Discussion
Major findings
This study aimed to record views and opinions of key stakeholders within the hospital on the quality of hospital-based physiotherapy. Overall, seven quality themes emerged from the data analysis, reflecting that the quality of hospital-based physiotherapy is characterised by: (1) a human approach, (2) context-specific and up-to-date applicable knowledge and expertise, (3) providing the right care in the right place at the right time, (4) a proactive departmental policy in which added value for the hospital is transparent, (5) professional development and innovation based on a vision on science and developments in care, (6) easy access and awareness of one’s own and others’ position within the interdisciplinary cooperation and (7) ensuring a continuum of care with the inclusion of preclinical and postclinical care of patients. Across all seven themes, three aspects stood out that were mentioned most often by all stakeholders: an expertise that matches the specific pathology of the patient, the hospital-based physiotherapist being a part of the care team and support and supervision of all patients’ physical functioning during the hospitalisation period.
Whereas patients mainly mentioned the personal qualities of the physiotherapist, the other stakeholders mainly focused on professional and organisational factors. Patients prefer physiotherapists who show empathy and engagement with their health problem, whereas hospital management would like them to be proactive. Medical specialists focus on expertise that matches the specific pathology of the patient, executive boards on an expert role regarding functional movement within the treatment team. Co-treating professionals emphasise the importance of interdisciplinary collaboration with the hospital-based physiotherapist.
Relation to similar studies
To our knowledge, this is the first study on quality aspects of hospital-based physiotherapy according to its main stakeholders (outside-in perspective). A recent systematic review of quality of care indicators for hospital-based physiotherapy emphasises once more that in this field more research is necessary to provide proven, evidence-based quality measures to fill this gap and determine how indicators can be implemented in everyday practice.14
However, part of our findings touches on the conclusion of earlier research into the changing role of the physical therapist in hospitals: an increased emphasis on higher-level skills in patient care and professional interaction and the continuing importance of professionalism.15 16
In general, information from a stakeholder analysis can be used to develop strategies for managing these stakeholders, to facilitate the implementation of specific decisions or organisational objectives or to understand the policy context and assess the feasibility of future policy directions.7 8 Within healthcare, this can lead to surprising insights, for example, by allowing the target group to have more influence on the therapy offered,17 18 or to discard a strategy that initially seemed the right one.19 When stakeholder insights are used to measure quality, it is important that stakeholders also collaborate in measurement development and selection.20 Regardless of which methodology for quality improvement is used (eg, Lean or Six Sigma), the most important aspect of successful quality improvement is to achieve stakeholder buy-in.21
Meaning and relevance of the findings
The results of this study offer opportunities for hospital-based physiotherapy to improve the quality of provided care seen from the perspective of key stakeholders. This applies to the individual hospital-based physiotherapist, the physiotherapy department and the entire hospital. In this way, with a better understanding of what key stakeholders expect, a quality policy can be worked on more effectively and efficiently, which strengthens the positioning of a hospital-based physiotherapy department within the hospital organisation. And when this process is combined with the results we found in a previous study in which we asked hospital-based physiotherapists and their managers what they thought were important quality aspects,9 a quality system for hospital-based physiotherapy can be established. This system can provide the local basis for a solid quality cycle, and when applied by more hospitals the possibility may arise to generalise data to nationwide quality indicators for hospital-based physiotherapy that enable benchmarking. Consistently high quality physiotherapy care can only occur when there is general commitment to understanding all the constructs of the physiotherapy quality package.22
Strengths and limitations
The design and analysis of this qualitative study was rigorous and robust. The large number of interviews with experienced professionals and patients, spread across three large Dutch hospitals, also contributes to the generalisability of the findings. It should be noted, however, that smaller district hospitals were not represented in this study. Another limitation is that only stakeholders in the hospital, and no external stakeholders were interviewed.
A key limitation is the extent to which the results of this qualitative study can be generalised or transferred to other contexts.23–25 Checklists to assess transferability of qualitative research do not exist.26 27
Seen from the perspective of our design and analysis, extrapolation of our results to the Dutch situation of hospital-based physiotherapy should be possible. From an international perspective, this is more complex because our data apply to the Dutch system and are difficult to translate to other countries due to differences in the healthcare system. The positioning of hospital-based physiotherapy may vary, depending on this amount of difference.
Suggestions for further research
To obtain a complete understanding of quality expectations of hospital-based physiotherapy, stakeholders outside the hospital qualified as less important in the preliminary research of this study, like health insurance companies, professional and patient associations and general practitioners, could be investigated additionally. Also, to support the findings of this study, additional research could be done in other settings and countries.
Conclusion
According to key stakeholders of hospital-based physiotherapy, important quality aspects were (1) an expertise that matches the specific pathology of the patient, (2) the hospital-based physiotherapist being a part of the care team and (3) the support and supervision of all patients concerning physical functioning during the hospitalisation period. Seven quality themes emerged from the data analysis of these stakeholders groups by which quality of hospital-based physiotherapy is furthermore characterised. Whereas patients mainly mentioned the personal qualities of the physiotherapist, the other stakeholders mainly focused on organisational factors. The results of this study offer opportunities for hospital-based physiotherapy to improve the quality of provided care seen from the perspective of key stakeholders.
Data availability statement
Data are available upon reasonable request. The raw data of this study are available from the first author at request.
Ethics statements
Patient consent for publication
Ethics approval
The Research Ethics Committee of the Radboud University Medical Centre, reference number: 2020-6288, exempted this study. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank Lara Bold and James Keogh, lecturers at Saxion University of Applied Sciences, for their contribution to translating quotes from the qualitative research from Dutch into authentic English, and their linguistic advices.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RS designed the work, collected, analysed and interpreted the data, wrote the draft of the manuscript, and is as first author responsible for the overall content as the guarantor. GD and LvH-S collected, analysed and interpreted the data, provided critical feedback on drafts of the manuscript and finally approved this version to be published. TJH and MM contributed to the analysis of the write up of the study results, the development of the manuscript and finally approved this version to be published. PB and PvdW contributed to the design and methodology, provided critical feedback on drafts of the manuscript, supervised the study and finally approved this version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.