Article Text

Abstract
ICU readmission is associated with increased mortality, resource utilisation and hospital expenditure. In the general population, respiratory-related event is one of the most common causes of unexpected ICU readmission. Patients with neurological deficits faced an increased risks of ICU readmissions due to impaired mentation, protective reflexes and other factors. A retrospective review revealed that the leading cause of unexpected ICU readmissions in adult neurovascular patients admitted to our hospital was respiratory related. A respiratory therapists-driven assessment-and-treat protocol was developed for proactively assessing and treating adult neurovascular patients. On-duty respiratory therapists assessed all neurovascular patients on admission, assigned a respiratory severity score to each patient and then recommended interventions based on a standardised algorithm.
Our quality improvement initiative had no effect on the rate of unexpected ICU readmissions in adult neurovascular patients. When compared with the baseline population, patients enrolled in the intervention group were significantly older ((79, 68–85 years) vs (71, 56–81 years)), but they spent comparable amount of time in the ICU (4.5 vs 4 days, p=0.42). When the respiratory severity score was trended in the intervention group, patients demonstrated significant improvement in their respiratory function, with a greater proportion of patients scoring in the minimal and mild categories and smaller proportion in the moderate category (p<0.01).
- Critical care
- Quality improvement
- Implementation science
- Patient-centred care
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Respiratory-related events are one of the most common reasons for ICU readmission in the USA.1 To gain a thorough understanding of this issue in our hospital, a retrospective review was conducted on all adult neurovascular patients who received rapid responses and/or were readmitted to Medical-Neuro ICU at the University of Pittsburgh Medical Center Mercy Hospital (UPMC Mercy) between 1 January and 30 September 2019. The review discovered that respiratory-related event was the major cause of unexpected ICU readmissions and that patients received respiratory assessment and/or intervention only when they experienced respiratory-related events, indicating a potential area for improvement.
UPMC Mercy is located within Pittsburgh’s downtown and is one of the UPMC system’s three quaternary flagship hospitals, serving a large catchment area of western Pennsylvania and neighbouring states. The amount of adult neurovascular patients admitted annually frequently exceed 1000, creating a busy and high turnover working environment. While our project team recognised that the environment and some staffing concerns might become the obstacles to implement this quality improvement (QI) project, it was believed that by putting respiratory therapists (RTs) in charge of the process could streamline the protocol implementation and provide benefits to this patient group. The project’s objective was to provide proactive respiratory assessment and interventions according to a predefined algorithm to every adult neurovascular patient on their admission day. Our aim is that by implementing this protocol, we will be able to reduce the rate of unexpected ICU readmissions due to respiratory-related events.
Background
Respiratory-related events were reported to be the leading cause for unexpected ICU readmissions.1 2 This is also true in patients who are neurologically critically ill.3 Additionally, ICU readmissions were also associated with increased mortality, longer length of stay in the ICU and hospital, and greater hospital operating cost.3–5 Numerous risk factors for unexpected ICU readmissions have been identified, including advanced age, the need for mechanical ventilation, vasopressor use, premorbid conditions, the presence of healthcare trainees, dysphagia at the discharge from ICU and the severity of the illness.1 6–8 Moreover, additional efforts were made to construct predictive models based on previously identified risk factors, yet the overall applicability of the models remained low.9 Lastly, increased clinical experience did not improve physicians’ ability to predict ICU readmissions.10 Additional research is warranted to advance this area, which is full of unanswered mysteries.
Protocols led by RTs have been shown to decrease the occurrence of unnecessary care, the length of ICU stay and hospital stay, medication consumption and total hospital operating cost.11–13 Successful implementation of these protocols has been shown to significantly improve departmental and hospital care performance and quality indices.8 14 After the retrospective review of all adult neurovascular admissions, we identified that the leading cause for unexpected ICU readmissions in our hospital was respiratory related. Additionally, respiratory assessment and care were provided as ‘rescue’ after a respiratory-related event. As a result, an idea sprouted that developing a standardised protocol to provide proactive respiratory care to reduce the rates of unexpected ICU readmissions in adult neurovascular patients.
Baseline measurement
To conduct this project, a representational sample of adult neurovascular patients who had rapid responses called on and/or unexpected ICU readmissions during their stay at UPMC Mercy was reviewed. It was decided that capturing all adult neurovascular patients admitted between 1 January and 30 September 2019, would provide a data sample capable of detailed analysis. This would allow for the identification of baseline pattern of respiratory care and the establishment of an accurate estimate of the actual number of unexpected ICU readmissions over this period.
Because respiratory care was traditionally used to ‘rescue’ patients after a respiratory-related event, we identified those patients who received rapid responses during this 9 month period. Baseline data revealed that 94 out of 655 adult neurovascular admissions satisfied the established criteria. We analysed demographic data, ICU readmission status and causes, admission diagnosis and discharge status. Unplanned ICU readmissions occurred in 36 patients, 22 of which were due to respiratory-related causes.
Design
It became evident that we need a quick and reliable standardised protocol for evaluating patients’ respiratory function and initiating appropriate interventions. While most RTs were receptive to the change, increased workload was a major concern. A QI team consisting of key stakeholders was formed, including two attending physician champions, two nursing champions and four RT champions. With the collaboration of all key stakeholders, an RT-driven assess-and-treat (RTDAT) protocol (online supplemental table 1) was created.
Supplemental material
As per the protocol, when the adult neurovascular patients were admitted to the Medical-Neuro ICU or neurology ward, bedside nurses would notify the on-duty RT once patients were roomed and ready. On-duty RTs evaluated patients’ respiratory function and assigned them a respiratory severity score based on the protocol. They then recorded it on the data collection sheet and provided recommended interventions and frequency according to the proposed algorithm (online supplemental figure 1). The on-duty resident physician ordered the requested medication and/or devices in the electronic medical records (EMR). At the end of RTs’ shifts, they would submit the data collection sheets to the RT champions’ office and give formal sign-outs to the next shift.
Supplemental material
The QI team met approximately every 4 weeks during the cycles to monitor the implementation and complication of project. Additionally, all RTs, resident physicians and nurses were educated on the RTDAT protocol, questions regarding the clinical flow were addressed. New staff received orientation from nurse and RT champions were also invited to the monthly meetings.
Strategy
PDSA cycle 1
The initial core QI team consisted of two attending physicians, two nursing unit directors and four RTs. The leading causes of unexpected ICU readmissions were identified via the retrospective review. According to the review, respiratory-related cause was the leading reason for unexpected Intensive Care Unit (ICU) readmission in adult neurovascular patients. The team then corroborated to develop the standardised assessment tool and intervention algorithm. We began by identifying two adult neurovascular patients admitted to the Medical-Neuro ICU, providing proactive respiratory assessment and intervention according to the protocol, and monitoring them throughout their stay on the Neurology ward. Although the initial results were promising, we encountered challenges of keep track of everything as the number of patients enrolled increased. We contacted the UPMC Mercy information technology department for assistance in generating a respiratory report, however, they were unable to assist due to all resources being redirected towards the preparation of COVID-19 pandemic.
PDSA cycle 2
A fellow physician and three resident physician champions joined the QI team to assist with project coordination, data collecting and chart review. To facilitate protocol implementation, we conducted formal training sessions on all Medical-Neuro ICU nurses and RTs, which were led by nurse champions and RT champions, respectively, in coordination with the physicians. The learners were informed about the aims of our initiative, their role in ensuring its success, and their concerns were addressed, incorporated into, and reflected in the protocol. All educational materials were also distributed to other resident physicians within the Department of Internal Medicine. Right after the intense educational phase, the first wave of COVID-19 struck, halting all research and QI activities.
PDSA cycle 3
We rescheduled the start of this QI initiative. Additional in-person and virtual training sessions were conducted to update all ICU nurses and the entire RT department. In response to the feedback, we simplified the data collection sheet and eliminated things that were difficult to obtain in the EMR, such as modified Rankin score. Following the repeated training phase, each adult neurovascular patient admitted to ICU was recognised, risk-stratified and cared according to the protocol, thanks to our enthusiastic nurses and RTs.
PDSA cycle 4
We broaden the scope of this QI initiative to include the Neurology ward. Additional training sessions were conducted for the floor nurses, and periodic review of the protocol was undertaken during the monthly staff meeting.
Results
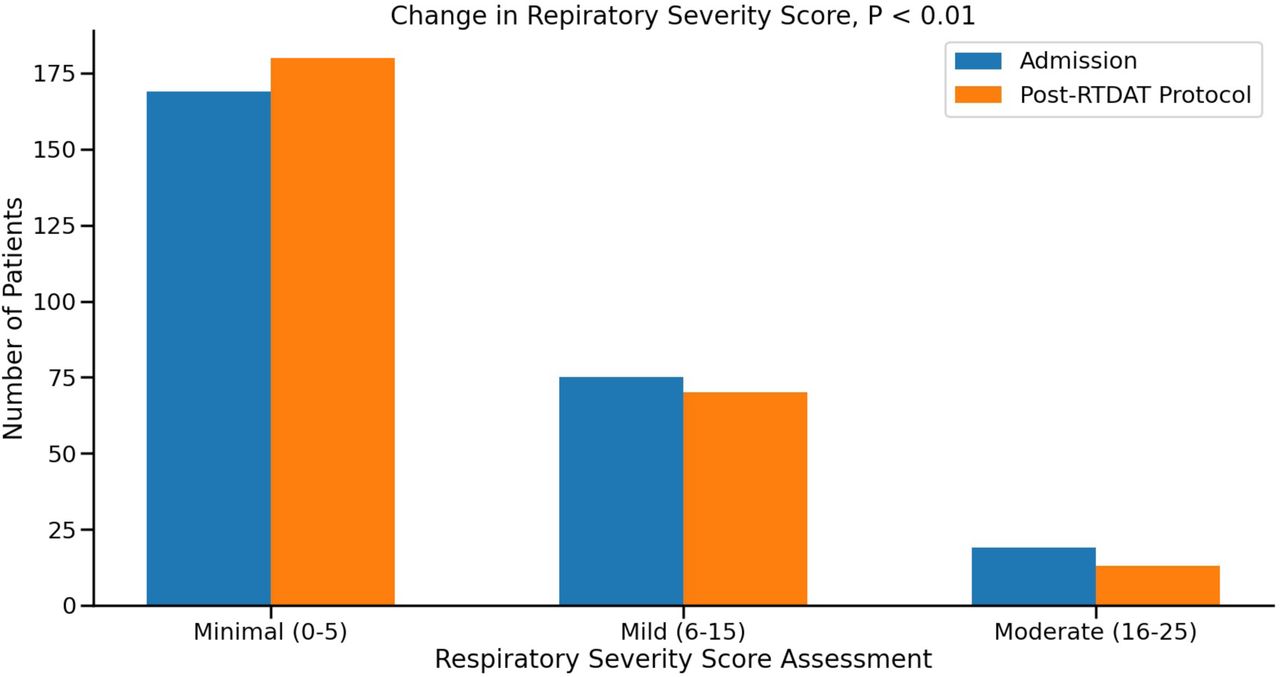
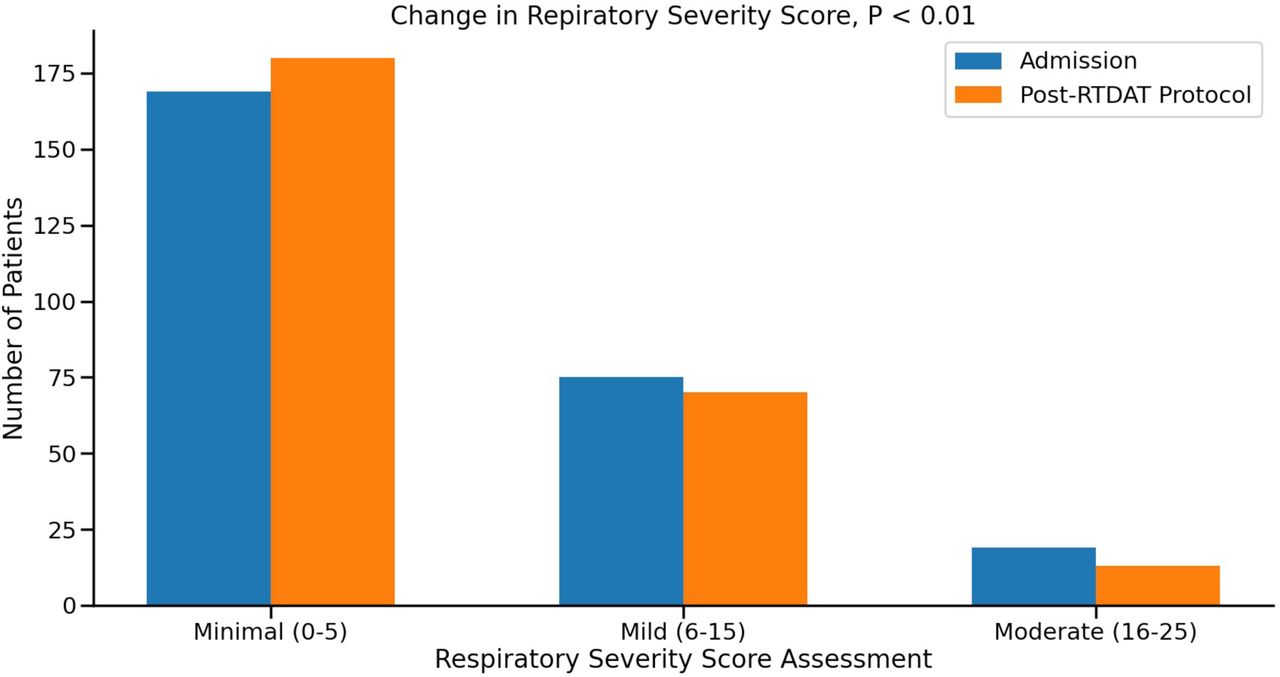
During our implementation phase, we provided proactive respiratory assessment and care to 263 patients; 17 patients suffered from unplanned ICU readmission. Fourteen were because of respiratory-related events. Our initiative did not reduce respiratory-related ICU readmissions in the adult neurovascular patients (table 1). Although patients in intervention group were significantly older (79, 68–85 years) than those in the baseline group (71, 56–81 years), both groups spent comparable amounts of time in the ICU (4.5 vs 4 days, p=0.42). When discharge destinations were classified as good or bad, intervention group had better discharge outcomes, which was defined as home and inpatient rehabilitation unit (p<0.01). Finally, patients in the intervention group demonstrated significant improvement in their respiratory severity score, with a greater proportion of patients scoring in the minimal and mild categories and a smaller proportion in the moderate category (p<0.01) (figure 1).
Subject characteristics
{kind=link}
Change in respiratory severity score after the implementation of RTDAT protocol. RTDAT, respiratory therapists-driven assess-and-treat.
Lessons and limitations
Inspired by previous work in the cardiothoracic ICU patient groups,8 our initiative aimed to decrease unexpected ICU readmission in the adult neurovascular patient population, with the particular emphasis on proactive respiratory assessment and intervention by the RTs. To accomplish this goal, a process must be developed with a standardised algorithm for the on-duty RTs to follow. A key lesson learnt during the process was the importance of identifying key stakeholders from diverse backgrounds (attending physician, nurse, RT, fellow physician and resident physician), who assisted in ensuring the protocol was activated and implemented effectively.
The multidisciplinary collaboration established the groundwork for the improvement process; prior to developing our protocol, we successfully identified stakeholders from the diverse backgrounds. By including their advice during the protocol design and planning phases, the initiative become more viable and streamlined. By putting RTs in charge of the protocol implementation ensured the excellent compliance rate of the protocol.
While our RTDAT protocol did not result in less respiratory-related ICU readmission, the shift of operational paradigm could be a significant contributing factor. During our enrolment phase, UPMC Mercy transitioned to become the primary receiving centre within the UPMC system for adult neurovascular patients over the age of 75 as a result of another QI initiative to improve quality metrics in stroke patient population. As a result, patients in the intervention group were significantly older and more likely to have complex comorbidities which raised their risk of unexpected ICU readmissions. However, we were able to maintain a similar rate of unexpected ICU admissions in the intervention group with the RTDAT protocol, and the patients enrolled had considerably improved outcome. Notably, the respiratory severity scores of patients in the intervention group also improved significantly, further supporting the efficacy of our RTDAT protocol. Additionally, the RTDAT protocol may have some additional advantages. The Neuro-ICU is always short of beds due to the increasing number of interventional and neurosurgical cases. By minimising the unexpected ICU readmissions, our RTDAT protocol may help optimise patient flow and the availability of beds. Even though this QI initiative did not reduce respiratory-related ICU readmissions, our RTDAT protocol was adopted by the hospital and implemented regularly on every adult neurovascular patient admitted to UPMC Mercy.
Our project has the following limitations. We were limited in our data collection and analysis capabilities from our EMR. We were unable to validate all intervention modalities and frequencies provided by the RTs in the EMR. In retrospect, we should have mandated this being documented in daily progress note. Due to the observational nature of this project, it was also susceptible to biases and confounding variables. In our study, for example, patients in the intervention group were older than those in the baseline group. As we all know, age is highly correlated with ICU readmission, owing to the fact that older patients tend to have higher prevalence of comorbidities and lower reserve. Additionally, while we were unbale to verify all the interventions in the EMR, the assessment and interventions provided in the intervention group adhered strictly to the pre-established algorithm, whereas the respiratory assessments conducted in the review period were completely random. Additionally, we were unable to alter physicians’ discharge practice pattern. Borderline patients may have been prematurely discharged to the neurology ward due to ICU bed requests for incoming patients. During the review and implementation phase of this project, there was no physician turnover, however it remained unknown what effect physicians’ discharge practice pattern might have had on the outcomes. Finally, generalising our findings to other ICU patient populations may be challenging because our patient cohort was limited to adult neurovascular patients.
Conclusion
With a proactive RTDAT protocol, we were unable to reduce respiratory-related ICU readmissions in adult neurovascular patients. However, a shift in our hospital’s operational paradigm may have contributed significantly to this negative result. Our data suggested that RTDAT protocol might improve overall respiratory performance and discharge outcomes in adult neurovascular patients.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by UPMC Department of Critical Care Medicine quality improvement committee as a QI project with ID of 2460.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors FW: protocol execution, data acquisition and analyses, literature review, manuscript draft. AA: protocol execution, chart review and data acquisition. NP: protocol execution, chart review and data acquisition. KP: protocol execution, chart review and data acquisition. DS: protocol design and execution, respiratory therapist lead, data collection. AD: protocol design and execution, respiratory therapist lead. JB: protocol design and execution, respiratory therapist lead. JA: protocol design and execution, respiratory therapist lead. JM: protocol design and execution, respiratory therapist lead. ML: protocol design and execution, nursing education. SZ: protocol design and execution, nursing education. JB: study concept, protocol design, literature review. FA: study concept, protocol design, literature review, data analyses, manuscript revision, guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.