Article Text

Abstract
Background Driveline infections (DLIs) are a common adverse event in patients on ventricular assist devices (VADs) with incidence ranging from 14% to 59%. DLIs have an impact on patients and the healthcare system with efforts to prevent DLIs being essential. Prior to our intervention, our program had no standard driveline management presurgery and postsurgery. The purpose of this Quality Improvement (QI) initiative was to reduce DLIs and related admissions among patients with VAD within the first year post implant.
Methods In anticipation of the QI project, we undertook a review of the programs’ current driveline management procedures and completed a survey with patients with VAD to identify current barriers to proper driveline management. Retrospective data were collected for a pre-QI intervention baseline comparison group, which included adult patients implanted with a durable VAD between 1 January 2017 and 31 July 2018. A three-pronged care pathway (CP) was initiated among patients implanted during August 2018 to July 2019. The CP included standardised intraoperative, postoperative and predischarge teaching initiatives and tracking. Using statistical process control methods, DLIs and readmissions in the first year post implant were compared between patients in the CP group and non-CP patients. P-charts were used to detect special cause variation.
Results A higher proportion of CP group patients developed a DLI in the first year after implant (52% vs 32%). None developed a DLI during the index admission, which differed from the non-CP group and met criteria for special cause variation. There was a downward trend in cumulative DLI-related readmissions among CP group patients (55% vs 67%). There was no association between CP compliance and development of DLIs within 1 year post implant.
Conclusion The CP did not lead to a reduction in the incidence of DLIs but there was a decrease in the proportion of patients with DLIs during their index admission and those readmitted for DLIs within 1 year post implant. This suggests that the CP played a role in decreasing the impact of DLIs in this patient population. However, given the short time period of follow-up longer follow-up will be required to look for sustained effects.
- Quality improvement
- Statistical process control
- Performance measures
- Healthcare quality improvement
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Driveline infections (DLIs) in durable patients with ventricular assist device (VAD) are costly adverse events for the healthcare system and the patient. Despite this, to date, only one recently published protocol on driveline management exists.
What this study adds?
Targeted Quality Improvement initiatives can help to reduce the burden of DLIs among patients supported on durable VADs.
How this study might affect research, practice or policy?
Management of the driveline requires a multidisciplinary effort that begins intraoperatively and continues postoperatively with ongoing patient management and education.
Introduction
In North America, diseases of the heart and heart failure are one of the leading causes of death.1 Transplantation is the gold standard of care for patients with advanced heart failure. However, the availability of donor organs is not sufficient to meet demand and certain comorbidities preclude some patients from transplant candidacy. To circumvent this, ventricular assist devices (VADs) can serve as a bridge to transplantation (BTT) or as destination therapy in this patient population.2–5 Yet, VAD support is not without its complications, with driveline infections (DLIs) being among the most commonly reported adverse event.6–11
Various studies have found that the incidence of DLIs in patients with VAD ranges from 14% to 59%, while other studies have reported that up to 60% of unplanned hospital readmissions among patients with VAD are due to DLIs.6 7 9 10 12–16 Risk factors associated with development of DLIs have been highly variable and at times inconsistent. Some studies have reported that obesity exists as a predictor of DLIs17 18 while other studies have not replicated this finding.19 Other reported risk factors include younger age,13 older age,20 diabetes,20 depression,8 renal failure8 and driveline and device characteristics.21–23 DLIs often occur early after implantation suggesting that the index hospital admission may play an important role in the development of infections.24 When aiming to reduce or eliminate the risk of DLI in patients with VAD, the variability in identified risk factors serves as a challenge for singular interventions.
DLIs decrease quality of life as they are a significant source of morbidity and mortality.6 7 9 Furthermore, hospital readmissions due to DLIs negatively affect the healthcare system as they require intensive management, diagnostic testing, further medical interventions and increase healthcare costs.14 15 25 A recent study identified the median direct hospital cost corresponding with a DLI-related readmission as 11 506 US$.26 Not surprisingly, DLIs are an expensive and undesired outcome not only for patients and care teams, but also for the healthcare system itself.26
Guidelines for the care of drivelines has been lacking with the first published protocol coming out in 2020.27 Our programme had no comphrensive standard approach to driveline care and over a 5-year period (2013–2018), there were 278 readmissions among 79 patients with VAD. Of these readmissions, 51% (n=141) were for VAD-related reasons, with the most common being DLIs (37%) with 52 DLI-related readmissions recorded during this time period. The median length of stay (LOS) for a DLI was 9 days (IQR 7 to 12) with a range from 2 to 88 days. Based on the average daily cost of a hospital admission during this time period and using the median duration of a DLI-related readmission LOS, we inferred that DLI readmissions cost our healthcare system ~$1 million to $3.4 million (CDN) depending on the location of readmission and stay (ie, ward vs cardiovascular intensive care unit (CVICU)).
As the causes of DLIs are multifactorial, we aimed to address this issue through a collaborative and preventative approach. We carried out a Quality Improvement (QI) project that sought to develop and implement a standardised three-pronged care pathway (CP) with the goal of reducing DLI-related readmissions in the first year post-VAD implant.
Methods
Setting
The adult Artificial Heart Programme at the Mazankowski Alberta Heart Institute, University of Alberta Hospital (Edmonton, Alberta, Canada) has been implanting durable VADs with a driveline since 2009 and serves as a referral centre for other provinces in western Canada. From June 2009 through July 2019, 164 patients received a durable VAD that had a driveline. The programme consists of a multidisciplinary team of stakeholders: cardiac surgeons, anaesthetists, VAD coordinators, CVICU and ward nurses, CVICU intensivists, social workers, dietitians, as well as patient and family caregivers.
Study design
Our QI project focused on reducing DLI infections and related admissions among adult patients on durable VAD support. Formulation of the QI project began in January 2018. In anticipation of the project, we undertook several preintervention analyses: (1) a review of the programme’s current driveline management procedures; (2) a survey with patients with VAD to identify barriers to proper driveline management and (3) a retrospective chart review to determine the baseline incidence of DLIs in patients implanted with a VAD. Based on the data from the preintervention analyses, we developed a three-pronged CP that was practice-based, with initiatives and education centred on the medical management of the driveline following VAD implantation. The QI project included adult patients undergoing VAD implantation between 1 August 2018 and 31 July 2019 (CP group) with patients followed for 1 year after implantation. At the end of the QI project, we conducted chart abstraction of patients involved in the CP to determine the incidence of DLIs and related hospital readmissions. Results from the CP group were compared with the retrospective cohort (non-CP group) to determine if the CP led to an overall reduction in incidence of DLIs and related hospital readmissions.
Preintervention review of driveline management procedures
Prior to the initiation of this QI project, there was no standard intraoperative procedure for driveline securing or velour positioning and there was variability in antibiotic prophylaxis at the time of VAD implant. Postoperatively, daily dressing changes occurred for the first 10 days followed then by dressing changes Monday/Wednesday/Friday dressing with patients and family receiving didactic teaching about driveline care and being observed performing the dressing change before patient discharge.
Preintervention patient survey
A convenience sample of patients was surveyed to identify common barriers that patients and families experience with caring for the driveline. Seven patients provided answers to the four-question survey and the consistent theme identified was that the cost of the dressing kit and supplies was a major barrier to proper driveline dressing management, with some patients indicating that they used alternatives to the recommended supplies in order to reduce the cost. Based on this feedback, the VAD programme developed a new, more cost effective driveline dressing kit. The cost of the new kit was $13CDN compared with the previous cost of $30CDN per kit.
Preintervention retrospective chart review
To serve as a baseline comparison, retrospective data were collected for a pre-CP intervention group, which included adult patients implanted with a durable VAD between 1 January 2017 and 31 July 2018 (non-CP group).
QI care pathway interventions
The QI technique used was a Total Quality Management Approach where emphasis is on a team-based approach for quality improvement.28 A DLI QI team was created that included VAD physicians, surgeons, coordinators, a social worker and a dietician who worked towards standardising driveline care and management.
As one of our primary drivers of change in this QI project, our goal was to develop and implement a three-pronged CP that was practice-based, with initiatives and education centred on the medical management of the driveline following VAD implantation.
Initiatives within the CP targeted cardiac surgeons, multidisciplinary team members (eg, dietitians, social workers, nurses), as well as patients and caregivers. The focus of the CP was on standardising driveline management at three time-points: intraoperative, postoperative and predischarge. We developed the CP after a number of meetings among the DLI QI team, review of the literature6 29–37 and feedback from stakeholders. Prior to implementation of the CP, the QI initiative was presented to stakeholders involved in the project in order to orient them to the initiative and outline their roles.
Table 1 provides an overview of all time-points and initiatives included as part of the CP.
CP Initiatives and Compliance Scoring Metric
One aspect of the CP was to foster education and awareness among the medical team and patients/caregivers about driveline management and infections. As a part of this, we developed a Driveline Dressing Video to use as an accessible educational resource. This video provided detailed footage of a driveline dressing change occurring from start to finish following the standardised protocol and aseptic technique. Further, we developed a digital Driveline Dressing Quiz that was to be used in conjunction with the video as an additional educational resource. The quiz was a direct reflection of the information presented in the video and was composed of 17 questions with a total score of 23 points. This quiz was tested on the VAD coordinators and other stakeholders (eg, social workers, dietitians) prior to its finalisation to assess difficulty, ease of completion and relativeness to the Driveline Dressing Video. The video and quiz were uploaded to a program-specific iPad for patient and/or caregivers to review prior to completing their own driveline dressing changes in hospital and prior to discharge. In addition, new paper-based infographics for patient use were developed that visually focused on the routine care of a driveline, proper positioning of the driveline to prevent any pull at the exit site, tips to prevent DLIs, signs and symptoms of DLIs and how to notify the VAD team if any signs or symptoms of infection were present.
Targeted specifically to the medical team, CVICU as well as ward nurses attended a 15 min in-service held by the VAD coordinators to review the new dressing change protocol and proper sterile technique for a VAD dressing change. For ease of access and as a source of ongoing reference among nursing staff, the Driveline Dressing Video was uploaded to CVICU and ward desktop workstations. Review of VAD driveline dressing changes and review of the video and quiz were included in the nurses’ annual VAD re-certification.
To track compliance with the CP, standardised Driveline Checklists encompassing 17 components of the initiative were created for use with VAD in-patients (table 1). Use of the newly developed low-cost dressing kit was not included in the compliance score. Missing documentation in a patient’s chart regarding completion of an initiative was interpreted as the initiative was not followed by a member of the team. Each patient received a compliance score out of 17 points, with good compliance to the CP protocol considered a score ≥80%.38
DLI data collection
Data collection for both groups (preintervention group (non-CP) and CP) included patient demographics, clinical and VAD characteristics, outcome at the end of follow-up, as well as DLI-related information up to 1 year post implant. DLIs were defined as per the Intermacs definitions which included clinical symptoms accompanied by a positive culture and initiation of antibiotic treatment.39 40
Measures
The outcome measures for the study included the incidence of first DLI, incidence of DLIs that occurred during the patient’s index admission and occurrence of DLI-related hospital readmissions within 1 year post implant. Our process measure included the overall compliance score as based on adherence to the intraoperative, postoperative and predischarge initiatives and standardised protocols by clinical professionals, patients and caregivers.
Data analysis
SPSS V.27.0 (IBM, USA) was used for descriptive statistical comparisons between the non-CP and CP groups. Descriptions for continuous variables are reported in terms of proportion, median, and the 25th, 75th IQR. To assess differences between study groups, the Mann-Whitney U (Wilcoxon rank-sum) test (two-tailed p value) was used to assess continuous variables whereas the Fisher’s exact test (one-tailed p value) was used to assess differences between categorical variables.
Time series data were analysed using statistical process control methods using P-Charts and run charts. These types of charts were used to compare DLIs and readmissions over time in the first year post implant between the non-CP group and CP group. Specifically, P-Charts, graphing proportion values over time, were used to detect special cause variation attributable to the implementation of the CP. Benneyan et al define special cause variation as ‘unnatural variation due to events, changes or circumstances that have not previously been typical or inherent in the regular process’ (p.59).41 This type of variation, as opposed to common cause variation, would indicate if the variations in our outcome measures were attributable to the implementation of the CP or occurred inherently and predictably.41 42 P-charts were analysed using standard criteria for probability established for assessing data points and their behaviours.41 The upper and lower limits were set at three SD from the mean. Run charts were used to examine variation over time for compliance scores with the median score determined and plotted as the centerline and probability rules used to determine special cause variation.
Patient and public involvement
The development of the research question and quality improvement project was designed to reduce the occurrence of DLIs and related hospital admissions in patients implanted with durable VADs. Patients and the public were not involved in any aspect of the research study (eg, design, recruitment, conduct). Dissemination of results is intended through open access publication.
Results
Demographic and clinical characteristics
A total of 55 patients were included in the project (non-CP (n=34) and CP (n=21) group)). Online supplemental table 1 shows baseline, clinical and DLI characteristics for all patients with a comparison of the non-CP and CP groups separately. The median age was 56 years (IQR 45 to 61) with the majority (87%) of the cohort male. The majority (87%) of patients had a diagnosis of cardiomyopathy, with idiopathic cardiomyopathy identified as the most common (45%) aetiology. Among all patients, the most common therapeutic intent for VAD use was as a BTT (86%). Overall, most patients (78%) were implanted with the HeartMate III (HM3) (Abbott, Abbott Park, Illinois, USA) and the median duration of support was 601 days (IQR 405 to 825). There was no significant difference in demographics and clinical characteristics between the two groups (online supplemental table 1). Just under half (47%) of the patients were still on VAD support when the last patient in the CP group reached the 1-year follow-up time-point.
Supplemental material
DLIs during follow-up period
As shown in online supplemental table 1, a higher proportion of patients in the CP versus non-CP group developed a DLI within the first year post-VAD implant (52% vs 32%, p=0.12). The median time to first DLI post implant was longer in the CP group (147 days; IQR 97 to 280) than in the non-CP group (88 days; IQR 53 to 202), although not statically significant (p=0.19) (online supplemental table 1). In addition, a smaller proportion of patients in the CP group (55%) were readmitted to hospital within the first year post implant with a DLI than those in the non-CP group (67%) (p=0.47).
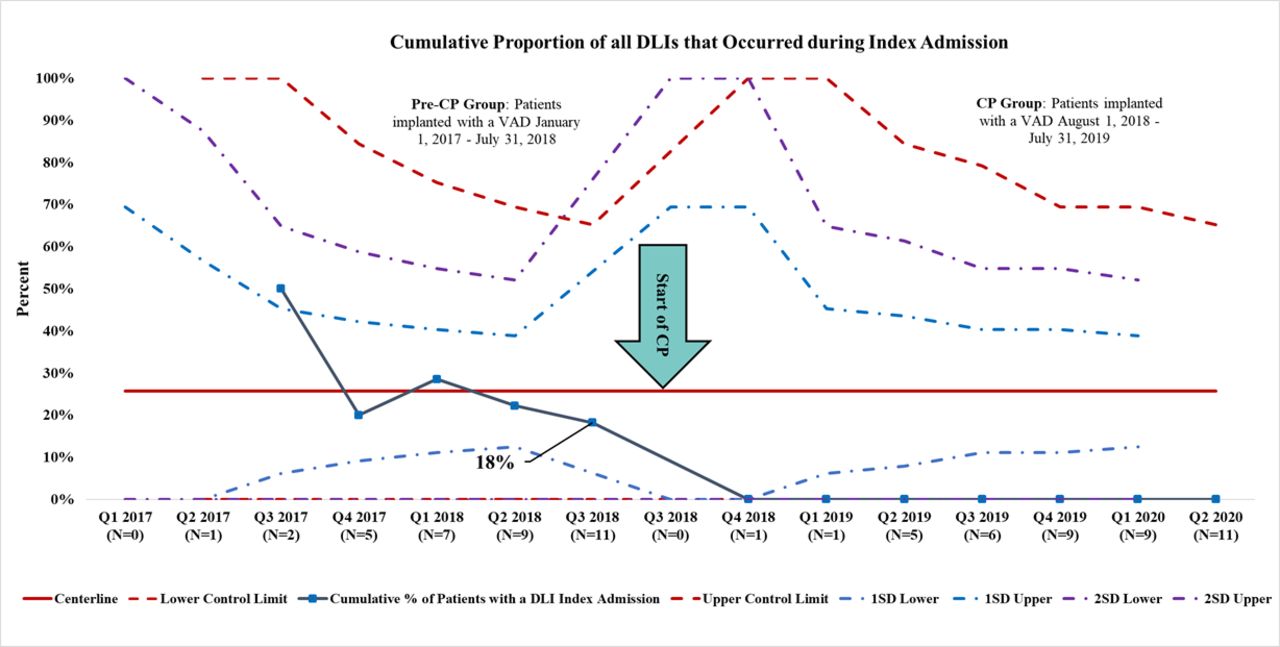
When examined using statistical process control methods, the P-Chart in figure 1 highlights an increasing trend for cumulative DLIs post-CP implementation. However, no DLIs developed during the index hospital stay among patients in the CP group (figure 2), which differed from the non-CP group and met criteria for special cause variation. Lastly, a downward shift in the cumulative DLI-related readmissions among patients in the CP group was noted (figure 3) but this shift did not meet the criteria for special cause variation.

Control chart displaying the cumulative proportion of implanted patients with a DLI, with n representing the cumulative number of implanted patients. Only first DLIs were included. The central red line represents the mean with upper and lower limits set at 3 SDs from the mean (dashed lines). CP. care pathway; DLI, driveline infection; VAD, ventricular assist device.

Control chart displaying the cumulative proportion of DLIs that occurred during index admission, with n representing the number of DLIs that occurred by the end of the quarter (Q). The central red line represents the mean with upper and lower limits set at 3 SDs from the mean (dashed lines). CP, care pathway; DLI, driveline infection; VAD, ventricular assist device.
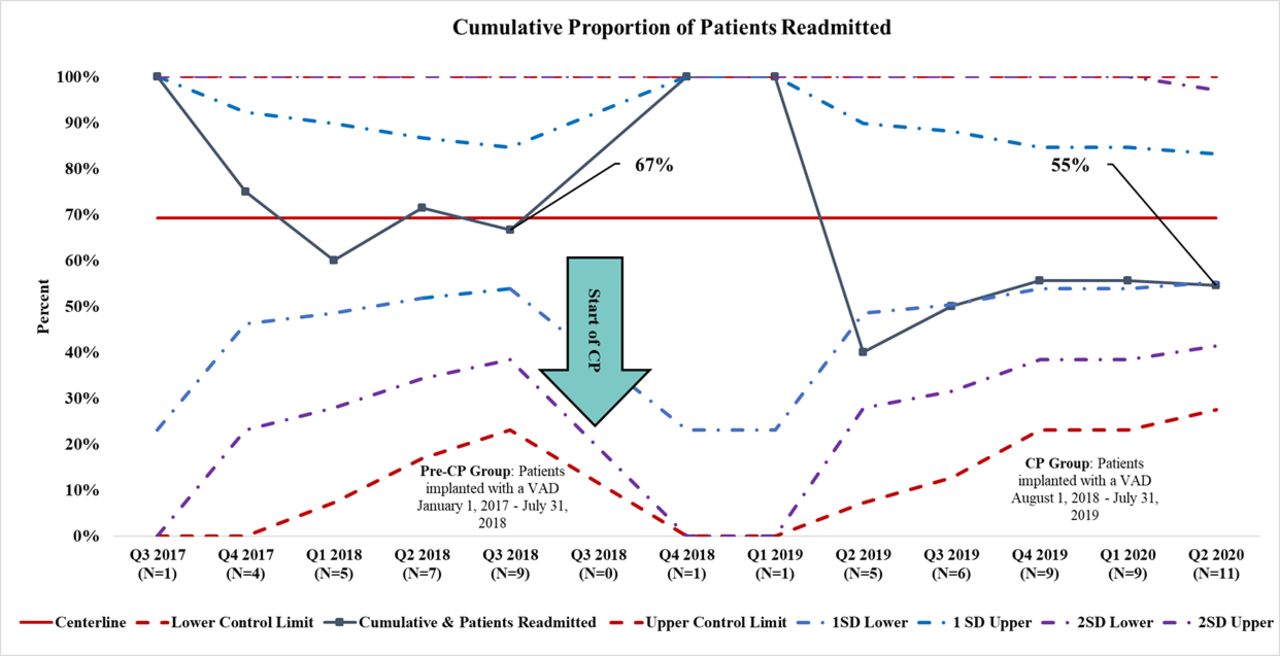
Control chart displaying the cumulative proportion of DLIs that required Hospital readmission, with n representing the number of readmissions in the quarter (Q). Each patient was censored following their first admission to hospital (excludes those DLIs occurring during index admission). CP, care pathway; DLI, driveline infection; VAD, ventricular assist device.
Protocol compliance
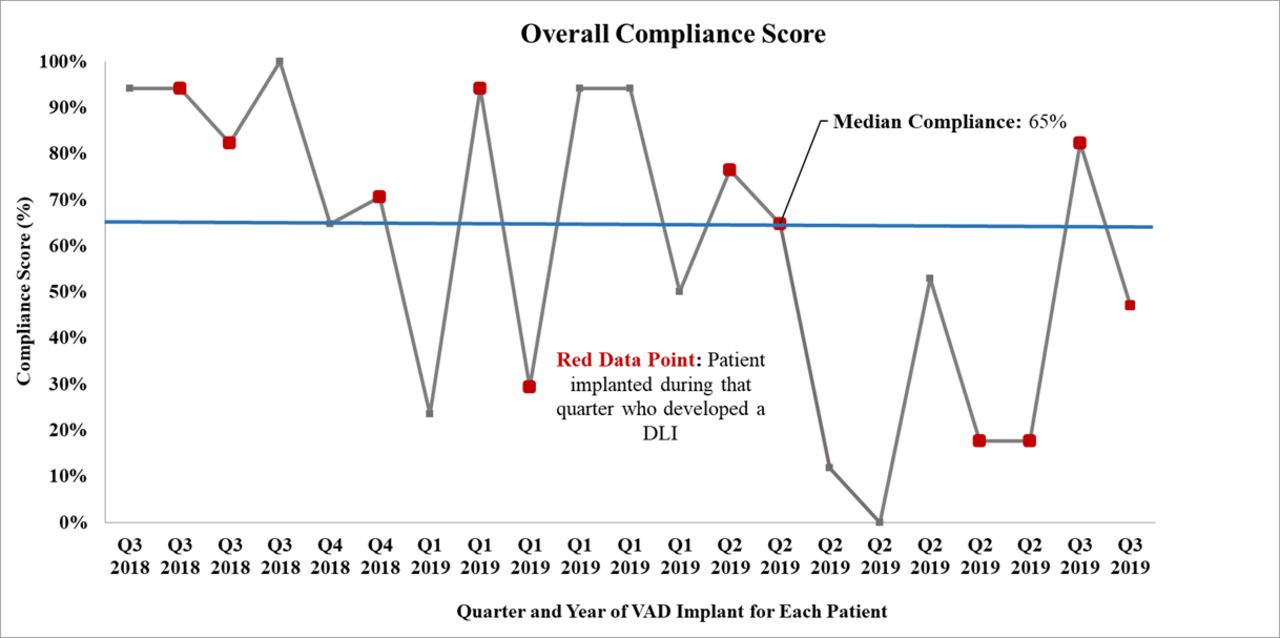
When analysing compliance scores, 62% of the patients had a compliance score of ≥80%. The median compliance score was 65% (IQR 27 to 94) (figure 4). No association was seen between good compliance (score ≥80%) and development of a DLI within 1 year post implant (p=0.60) or readmission (p=0.25). As figure 4 highlights, there was a noticeable decrease in compliance over time, with the last two quarters of the project having the worst compliance scores and the majority of DLIs in the CP group (66%). The shift in compliance scores below the median almost satisfies the criteria for special cause variation, with the exception of one outlier in Quarter 3 of 2019.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Run chart displaying compliance scores with the CP protocol for each patient with median displayed in blue. Red dots represent patients implanted in that quarter (Q) that developed a DLI within a year of VAD implant. CP, care pathway; DLI, driveline infection; VAD, ventricular assist device.
Discussion
This QI project standardised driveline management for patients with VAD at three interdisciplinary time-points, in addition to initiating standard and enhanced patient and provider education, as well as documentation tools within this programme. Although there was an increase in DLIs among patients involved with the CP, there was a reduction in DLI-related readmissions over the first year post implant. Furthermore, there also was a significant decrease in DLIs during the index admission among patients in the CP group. Thus, indicating that the implementation of the CP did in fact play a role in reducing the impact of DLIs in this patient population within our programme. Additionally, the increased time to infection may suggest that the multiprong interdisciplinary initiatives were effective initially in addition to standard of care but that the impact diminished over time as patient management occurred in the outpatient setting. Lastly, it is possible that the increased incidence of DLIs among patients in the CP group was impacted by the change in implanted device during the duration of the QI project. Prior to the initiation of the CP, the predominant devices implanted were the HeartWare VAD (HVAD) (Medtronic, Minneapolis, Minnesota, USA) and the HeartMate II (HMII) (Abbott, Chicago, Illinois, USA) but around the time the CP was started, the programme had switched to implanting patients predominantly with the HM3. Compared with the HVAD and HMII, the HM3 has a driveline that is larger in diameter and is stiffer which may increase the risk of patients implanted with this type of device developing DLIs.22 27 43 This is relevant to our study given that all the patients in the CP group were implanted with the HM3 device and we saw an increased incidence of DLIs among patients in the CP group compared with the non-CP group where only 65% of patient were implanted with the HM3.
The improvements in terms of reducing DLIs during the index admission and DLI-related readmissions within the first year post implant among CP patients illustrate the effectiveness of addressing driveline management through an interdisciplinary approach. This aligns with a study conducted by Bernhardt et al in which a 10-step standard operating procedure (SOP) for driveline exit site (DLES) care (the DESTINE SOP) and wound staging was cultivated.27 Similar to our study, key aspects included standardising procedures for dressing changes, driveline immobilisation, patient training and re-evaluation. We agree with Bernhardt et al that an interdisciplinary approach to DLES management and awareness is needed to prevent DLIs as well as increase patient compliance and quality of life.27 While the above article had some similarities with respect to approach to driveline management, the study did not evaluate the impact of their QI initiative.
Another key finding was that compliance scores decreased over time and ultimately the worst scores coincided with the period in which the majority of DLIs in the CP group occurred. This phenomenon, where continued implementation of an initiative waivers over time, has been well described and is sometimes referred to as the ‘bathtub curve’, where the impact may decrease overtime for design or situational factors.38 In this case, situational factors such as changing team members and burnout over time may have played a role. Successful CP uptake and implementation is a complex process and requires careful consideration about facilitators and barriers in order to change behaviour.44 Facilitators and barriers to the uptake of our CP need to be further explored. Our patterns of compliance may indicate that further resources are needed at adapting implementation strategies over time based on feedback from CP stakeholders.
By taking a QI approach, this allowed us to not only assess the impact of DLIs and readmissions in the patient population but also actively implement initiatives intended to target aspects of care in the hopes of improving short-term and long-term outcomes. The QI approach required consideration of all stakeholders and interdisciplinary team members as our initiatives may directly affect them. Instead of simply collecting data on VAD-related readmissions, we dove deeper to assess how we could effectively improve our target population’s experience with DLIs and readmissions. Compared with traditional statistical methods where a measure of central tendency is compared before and after an intervention, QI methods look for trends over time, which may be missed by statistical tests. Run and control charts help us better understand the nature of the data and look for trends of improvement or worsening with interventions and if the impact is sustainable.4 45 46 This is clearly highlighted in this QI initiative where traditional statistical methods did not show any significant difference in outcomes pre-intervention and post interventions. However, by understanding the variance over time we were able to observe changes through the QI methods employed.
Limitations
There are a number of limitations inherent within the study design that may have affected the outcomes. CP development and implementation involves the utilisation of significant resources.43 Following completion of the first cycle, we began to focus on ways to improve the CP. However, despite some modifications to the CP, we were unable to proceed with a second cycle given the beginning of the COVID-19 pandemic, which resulted in decreased resources for the programme, a decrease in surgeries and redeployment of key staff. We felt that all these factors would likely have a major impact on the overall result of a second cycle.
Given the time span of the QI project, it was impossible to control for the change in VAD device used by our centre. With this, there is potentially an inherent selection bias that could not have been predicted at the start of this project as there was little information available about the HM3 and it was not known that this device would become the primary device implanted at our institution. There are limitations to the generalisability of the outcomes found in our study due to the small sample size. The small sample size also resulted in low statistical power, which not only limited inferential statistical assessment but also likely affected our results from the statistical process control methods, as there were less than the number recommended of data points post intervention. In addition, there were 12 patients that did not meet the 1-year follow-up point due to explant of the device, transplant or death and therefore may have resulted in bias to the sample. Lastly, the CP involved multiple components and it is not possible to tease out which components were the most useful and which components need further refinement. However, from the data, it appears that the CP was successful at preventing in-hospital DLIs during the index admission and at reducing DLI-related admissions although there were more patients with DLIs within the first year post implantation compared with the non-CP group. This highlights an area for the programme to focus on which is outpatient care of the driveline so that the initial improvements after surgery with respect to DLIs is sustained as the patient is followed postdischarge in the outpatient setting.
Conclusion
With the observed improvements, we speculate that the CP induced a cultural shift in awareness regarding the importance of effective and standardised techniques for driveline management, infection identification and prevention. This shift in awareness likely played an important role in reducing the impact of DLIs for this patient population but further work is required to maintain and improve compliance over time to ensure ongoing effectiveness.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but based on the criteria established by the Research Ethics Board at the University of Alberta (Edmonton, Alberta, Canada), this project met the criteria for Quality Improvement and as such was exempt from full ethical review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to the preparation of this manuscript. Material preparation and data collection were performed by JS, ND, LC and OZ. JS wrote the first draft of the manuscript with all other authors commenting on previous versions. All authors read and approved the final manuscript.
Funding Alberta Health Service Chief Medical Officer (CMO) Quality Innovation Fund.
Competing interests HB contributed to Consultant for Abbott. JC contributed to non-restricted education grant from Abbott; Medical Monitor for Pumpkin Trial. DHF contributed to Stock Owner for Tevosol.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.