Article Text

Statistics from Altmetric.com
Background
Patients undergoing autologous haematopoietic stem cell transplants (ASCT) lose their acquired immunity against various pathogens due to reset and weakening of the immune system.1 As such, Ontario Health guidelines recommend reimmunising these patients against vaccine-preventable diseases beginning 4–6 months post-transplant.2 London Health Sciences Centre (LHSC) performs approximately 80–90 ASCT procedures annually for haematological malignancies such as multiple myeloma, non-Hodgkin’s lymphoma and Hodgkin’s lymphoma. The LHSC ASCT team routinely disseminates recommendations for revaccination, but prior to this project local data regarding adherence to these recommendations was not available. As such, this quality improvement project aimed to assess compliance with post-ASCT vaccinations at LHSC, and to explore ways to improve this compliance.
Methods
In December 2020, 60 patients who received ASCT procedures at LHSC at least 6 months previously were identified by LHSC ASCT staff. Out of the transplanted patients, 53 were able to be contacted via telephone by a team of medical students (5 were not reachable by phone and 2 were deceased). Patients were asked to self-report their revaccination compliance, and those who were not fully compliant were asked to identify barriers to revaccination (see attachment online supplemental questionnaire script).
Supplemental material
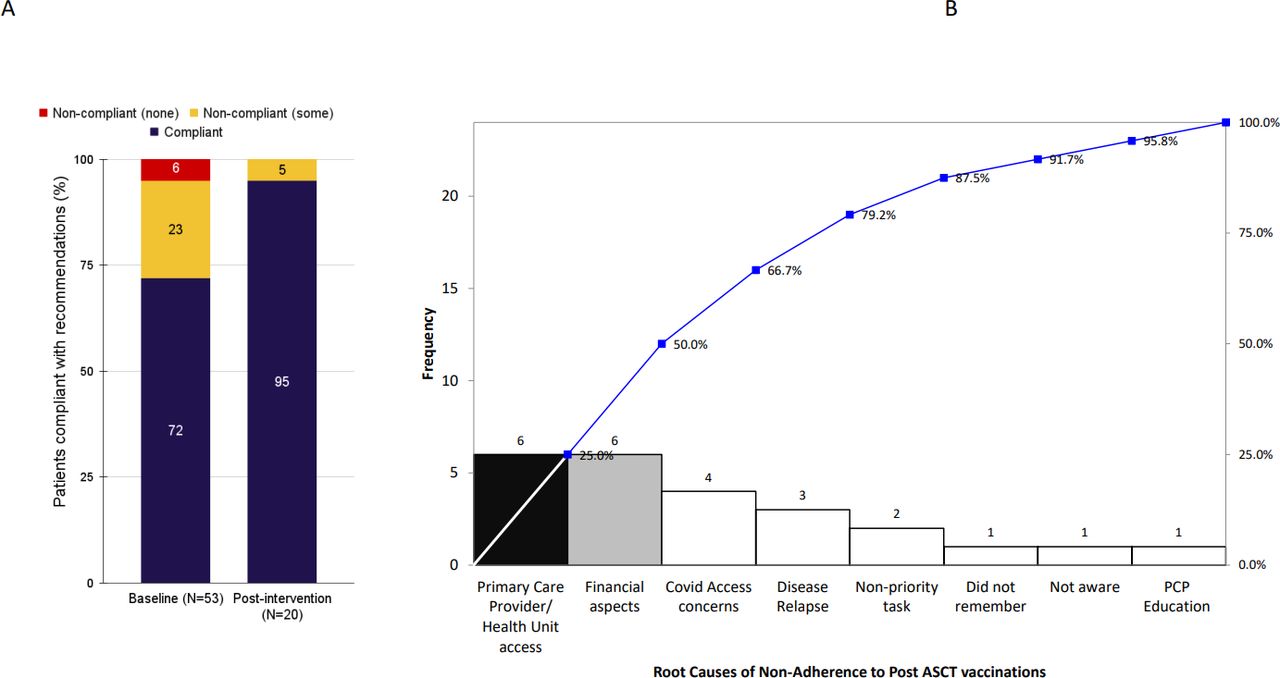
A root cause analysis was done to elucidate the major barriers to revaccination based on the December 2020 cohort (figure 1B). As the most commonly identified barriers were related to how to access and fund vaccines, a personalised information packet on these topics was designed (see attachment online supplemental information packet). Certain details were able to be individualised to each patient, including contact information for the nearest places they could access vaccination.
Supplemental material
{kind=link}
A. Re-vaccination compliance post ASCT at Baseline and after planned intervention. B. Pareto chart showing major root causes. ASCT, autologous haematopoietic stem cell transplant; PCP, Primary Care Provider.
In March 2021, 20 new patients who received ASCT procedures at LHSC at least 6 months previously were identified, and information packets were personalised and mailed to them. In April 2021, these 20 patients were contacted via telephone and asked to self-report their revaccination compliance. They were also asked whether they found the information packet to be accessible and helpful.
No patients or members of the public were involved in the design, conduct, reporting or dissemination plans of the research.
Results
At baseline, 72% of patients were compliant with post-ASCT revaccination (N=53 patients contacted in December 2020, who had received ASCT at least 6 months previously). Incompletely compliant patients identified vaccine cost and access to healthcare providers as major barriers (figure 1).
Among patients who received personalised information packets on how to access and fund vaccinations, 95% were compliant with revaccination (N=20 patients contacted in March 2021, who had received ASCT at least 6 months previously). The majority of patients described the intervention as accessible and helpful via descriptive patient surveys. There were negligible costs involved, primarily related to LHSC staff time and postage.
Discussion
This study estimated the baseline rate of post-ASCT revaccination compliance at LHSC to be 72%. It is likely that revaccination rates are suboptimal across many institutions that perform ASCT. Indeed, revaccination compliance post stem cell transplant has been estimated at 76% at Yale New Haven Hospital in Connecticut, and 67% at the Karmanos Cancer Center Bone Marrow Transplant Center in Michigan.3 4 It is not known how the ongoing COVID-19 pandemic might influence compliance rates. However, with increasing access to COVID-19 vaccines and decreasing provincial restrictions, it is likely these barriers will not persist long term.
This study identified vaccine cost and access to healthcare providers as major barriers to vaccine compliance among post-ASCT patients. This study suggests that mailing personalised information packets on how to access and fund vaccinations may be an effective low-cost strategy to improve post-ASCT revaccination compliance. In other institutions, increased efforts to educate patients and tailored follow ups have been identified as solutions to improve revaccination programmes.5 In another study examining reasons for declined revaccinations, some cited reasons included time out from transplant, immunosuppressive therapy and prior adverse reactions.6
A key limitation of this study is its reliance on patient self-report of vaccination status, which may have led to an over-estimation of vaccine compliance (eg, if patients were unwilling to admit to non-compliance, or unsure of their compliance and unwilling to check their records). Further studies could consider using alternate methods to assess patient vaccination status (eg, accessing electronic medical records or asking for proof of vaccination). Further limitations include the lack of a control group that was not sent the information packets but was contacted simultaneously with the March 2021 group, and the lack of statistical analysis. This project also did not formally assess the long-term sustainability of mailing information packets, though the low costs incurred suggest this may be feasible. A questionnaire is planned in coming months to assess the sustainability of this intervention. To further lower financial, environmental and time costs, other institutions could consider options such as not personalising the information packets, emailing the information to patients rather than traditional mailing, or offering the information as a pamphlet during in-person appointments rather than mailing it.
In conclusion, a timely, patient centric, efficient and effective intervention described above is able to make a desired impact on improving revaccination rates in post-ASCT population at our centre. This low cost intervention can be replicated in other transplant centres to achieved the goal of high immunisation rates.
Ethics statements
Patient consent for publication
Ethics approval
Because this study was identified as having low risk for participants by the ARECCI screening tool (A pRoject Ethics Community Consensus Initiative), no formal ethics review was completed.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at Cellular Therapy and Transplant Canada annual conference 2022 and Institute of HealthCare Improvement Scientific Symposium 2021
Contributors CD and AJK: Survey design, data collection, manuscript preparation. AS, CR, HC and ZK: Survey design, data collection. AF, SN and DS: Project design, letter design and mailing, administrative support. UD: Project design, project coordination, manuscript preparation and corresponding author.
Funding Funded by the Blood and Marrow Transplant Program, London Health Sciences Centre, London, ON, Canada. No specific grant/award.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.