Article Text

Abstract
Background This systematic review used qualitative methodologies to examine the role of quality improvement collaboratives (QICs) in general practice. The aim was to inform implementers and participants about the utility of using or participating in QICs in general practice.
Methods Included studies were published in English, used a QIC intervention, reported primary research, used qualitative or mixed methods, and were conducted in general practice.
A Medline search between January 1995 and February 2020 was developed and extended to include Embase, CINAHL and PsycInfo databases. Articles were sought through chaining of references and grey literature searches.
Qualitative outcome data were extracted using a framework analysis. Data were analysed using thematic synthesis. Articles were assessed for quality using a threshold approach based on the criteria described by Dixon-Woods.
Results 15 qualitative and 18 mixed-methods studies of QICs in general practice were included. Data were grouped into four analytical themes which describe the role of a collaborative in general practice: improving the target topic, developing practices and providers, developing the health system and building quality improvement capacity.
Discussion General practice collaboratives are reported to be useful for improving target topics. They can also develop knowledge and motivation in providers, build systems and team work in local practice organisations, and improve support at a system level. Collaboratives can build quality improvement capacity in the primary care system. These roles suggest that QICs are well matched to the improvement needs of general practice.
General practice participants in collaboratives reported positive effects from effective peer interaction, high-quality local support, real engagement with data and well-designed training in quality improvement.
Strengths of this study were an inclusive search and explicit qualitative methodology. It is possible some studies were missed. Qualitative studies of collaboratives may be affected by selection bias and confirmation bias.
PROSPERO registration number CRD4202017512.
- Collaborative, breakthrough groups
- General practice
- Healthcare quality improvement
- Primary care
- Quality improvement methodologies
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Collaborative, breakthrough groups
- General practice
- Healthcare quality improvement
- Primary care
- Quality improvement methodologies
What is already known on this topic
Repeated systematic reviews of quality improvement collaboratives have found they can have positive effects on target topics. This qualitative systematic review is the first to focus on their role in the unique and strategic context of general practice.
What this study adds
Collaboratives can be useful in general practice for improving target topics, developing practices and providers, developing the health system and building quality improvement capacity. Collaboratives appear to provide outcomes strategic for improving general practice, which is important for efficient, effective health systems.
How this study affects practice
Future implementations should be cognisant of their potential impact beyond target topics and consider how to optimise impact in all four areas.
Introduction
Quality improvement collaboratives (QICs) are multifaceted interventions in which teams from multiple sites come together to make improvements around a common goal (box 1). They have been widely used in a broad range of healthcare settings. The dominant model is the Breakthrough Series developed by the Institute for Healthcare Improvement.1
What is a quality improvement collaborative (QIC)?2
A QIC is a multifaceted approach to quality improvement that involves five essential features:
A target topic, most often a subject with large variations in care or gaps between best and current practice, for example, glycated haemoglobin levels (diabetes) and central line infection rate.
Clinical experts and quality improvement experts who provide ideas and support for improvement. They identify, consolidate, clarify and share scientific knowledge, best practice and improvement knowledge.
Multiprofessional teams from multiple sites which are willing to improve care, share and participate.
A model for improvement which involves setting clear, measurable targets, collecting data and testing changes quickly on a small scale to advance reinvention and learning by doing.
A series of structured activities (learning workshops, activity periods, visiting facilitators) in a given time frame to advance improvement, exchange ideas and share the participating team’s experiences.
There is debate over the effectiveness and particularly the cost-effectiveness of QICs. Schouten et al, in their 2008 review,2 found that the evidence for QICs was positive but limited. The same group3 found that aspects of teamwork and participation in specific collaborative activities were associated with improvement success. Most studies included by Wells et al4 in their 2018 review reported improvements in targeted clinical processes and patient outcomes.
There are a number of activities within collaboratives which are associated with improved outcomes.5 6 Zamboni et al found that participation in a QIC could result in improvement of health professionals’ knowledge, problem-solving skills and attitudes, teamwork, shared leadership and improvement habits.6 Peer interactions could generate normative pressure, opportunities for capacity building and peer recognition. All major reviews noted that the literature was limited in quality.
Improving general practice is of pressing interest because there is strong evidence that it is key to effective, efficient and equitable health systems.7–10 The challenges of ageing populations, rising chronic disease rates, increasing costs and stretched hospitals make improving primary care a high priority. In the past, the sector has been characterised by episodic, reactive care provided in face-to-face consultations. Typically, the provider was a physician, often in a solo practice, who may be relatively professionally isolated.10 The Organisation for Economic Cooperation and Development10 and the WHO11 have called for transformation from a reactive, episodic model to more person-centred, integrated, multidisciplinary care which is population based.11 12 Increased use of digital technologies, such as electronic health records and virtual care, has been identified as a key enabler.7 11 The collaborative, data-driven, evidence-based aspects of QICs appear to align well with these reforms in general practice.
The importance of context is well described in the implementation literature.13 Interventions that are effective in one context may be ineffective in another. General practice presents important and unique contextual challenges. Organisations tend to be relatively small. They may be poorly integrated with the wider health system. Primary care in many countries is relatively under-resourced.10 These factors reduce capacity for change, making improvement more challenging. To date, no systematic reviews have focused specifically on the role of QICs in the general practice context.
This systematic review explores the role of QICs in improving general practice. In contrast to previous general reviews of QICs, it uses qualitative methodologies to synthesise qualitative literature. Qualitative methods have been selected to develop a nuanced understanding of the views of participants. The purpose is to inform implementers and participants about the utility of using or participating in QICs in general practice.
Methods
A team of researchers with experience in general practice, quality improvement (QI) and systematic reviews determined the design and conduct of the study. A protocol is available at the PROSPERO international register of systematic reviews (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=175129).
The research team elected to focus on qualitative studies and qualitative components of mixed-methods studies. This strategy was selected to yield rich descriptions of the experience of front-line informants of the roles of QICs in the general practice context.
Search strategy
A Medline search using the OVID platform, between January 1995 and February 2020, was developed. QICs were identified using a search string developed by Schouten et al and used in subsequent reviews by Hulscher et al, Nadeem et al and Wells et al2–5 (online supplemental appendix 1). Articles addressing general practice were identified using search terms developed by the Australian Primary Health Care Research Institute (online supplemental appendix 1).14 The search string was translated for use with Embase, CINAHL and PsycInfo databases. The reference lists of the five general reviews2–6 of QICs were examined for articles based in general practice. These reviews were also forward chained to identify general practice-based articles which cited them.
Supplemental material
Grey literature was sought using a Google search on the terms “Quality Improvement Collaborative” and “General Practice”. The first 10 pages were analysed. The evidence-based medicine resource, the ‘TRIP database’,15 was searched for the same terms and the first 10 search pages examined for potentially eligible reports.
Article selection
After removal of duplicates, a title and abstract review of 20% (620 articles) of the sample was completed by one of the authors (AWK) and a research assistant using the online review tool Covidence.16 Both are experienced qualitative researchers. Differences were resolved through consensus and an agreed review process established. Due to limited resources, the agreed review process was applied to the remaining studies by one researcher (AWK). As a check, a random audit of a 10% sample of the excluded articles was completed by a second researcher (HS). No articles in the random sample were found to have been inappropriately excluded.
A full-text review was completed on the remaining articles by one researcher (AWK) according to the agreed inclusion criteria.
Inclusion criteria
Studies were included if they were: published in English; used a QIC intervention (see box 1); reported primary effect measures, healthcare processes or patient outcomes; used qualitative or mixed methods; and conducted in general practice. Studies were considered ‘conducted in general practice’ if general practitioners or the general practice setting was the target of the QIC. Included studies involved physicians described as ‘general practitioners’, ‘primary care physicians’, ‘family medicine specialists’ or the equivalent.
Data extraction
This review sought to identify views about QIC roles or outcomes in the broadest sense. A framework analysis17 was used to identify qualitative outcomes in the text of included studies. They included target outcomes and processes. They also included any other qualitative outcomes identified by participants. Texts were coded line by line using QSR NVivo V.12 software.18 Data were extracted by one experienced qualitative researcher (AWK) and discussed with another experienced qualitative researcher (CWMT).
Synthesis of results
Data were considered by two researchers (CWMT, AWK) and through thematic synthesis early descriptive themes proposed. The codes were grouped into higher descriptive themes through iterative discussion (CWMT, AWK) and presented to the wider research team for feedback. Through an iterative process with the research team, a higher analytical coding model was created and revised following discussion.
Quality assessment
Articles were assessed for quality using a threshold approach based on the criteria described by Dixon-Woods et al.19 A low threshold was adopted to be as inclusive as possible given the ongoing discussion of theoretical and practical challenges in quality assessment of qualitative articles. Studies were assessed based on five questions: Are the aims and objectives of the research clearly stated?; Is the research design clearly specified and appropriate for the aims and objectives of the research?; Do the researchers provide a clear account of the process by which their findings were reproduced?; Do the researchers display enough data to support their interpretations and conclusions?; Is the method of analysis appropriate and adequately explicated?19
Results
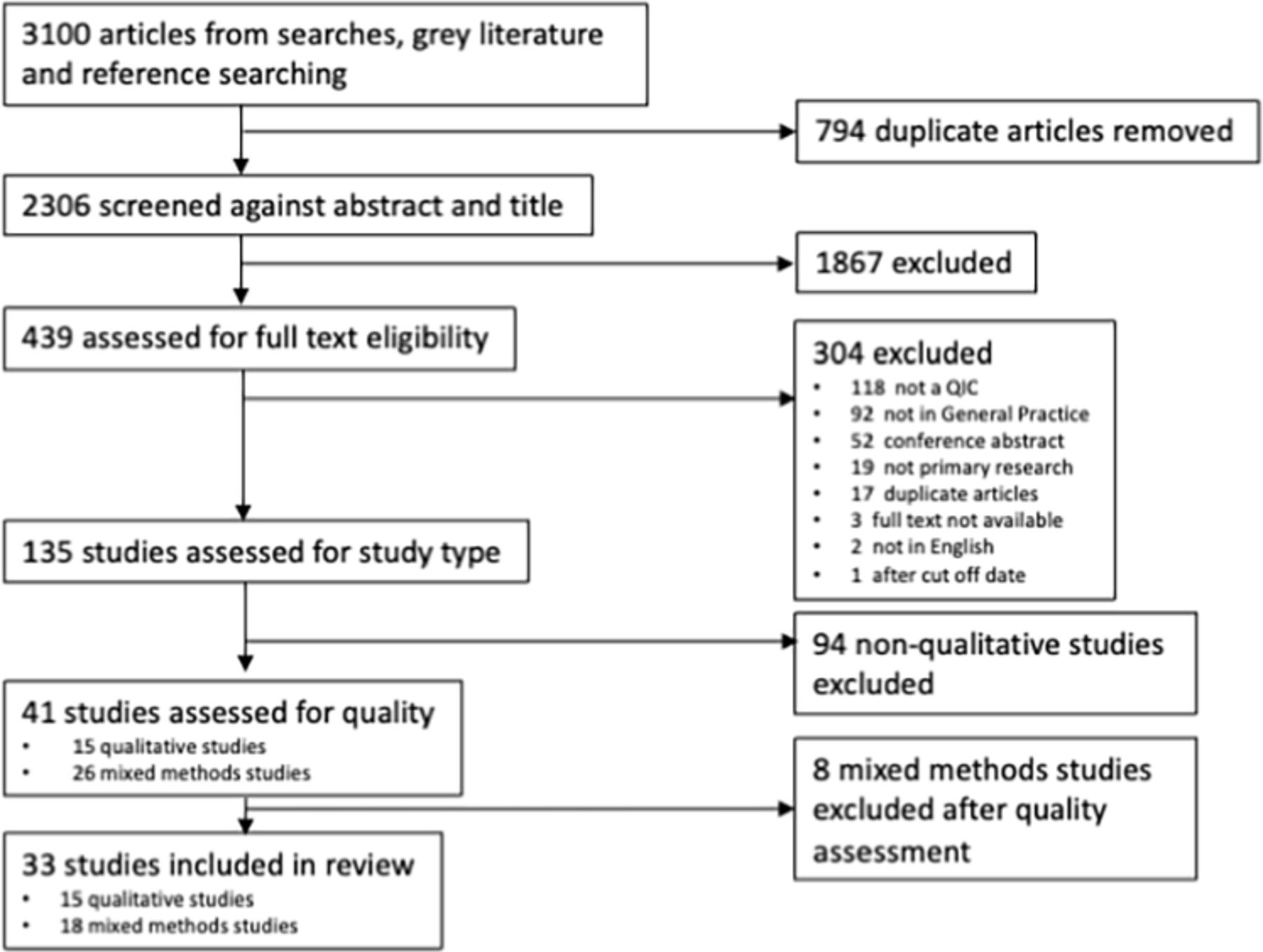
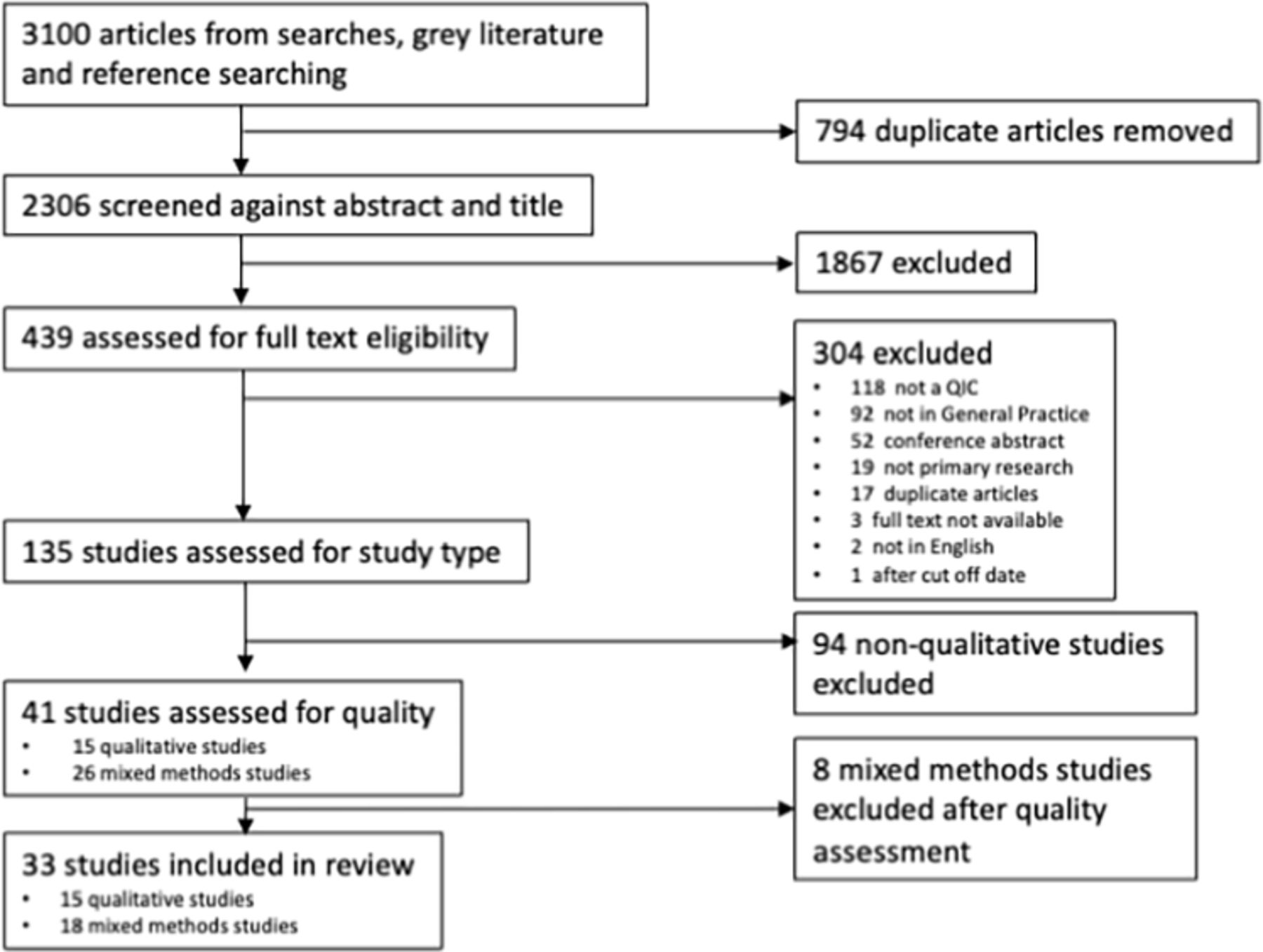
There were 3100 articles identified by the search strategies (figure 1). After screening and quality assessment, 33 articles, representing 26 projects, were included (online supplemental appendix 2). Quality assessment resulted in exclusion of eight mixed-methods studies which did not describe data collection, display data or describe analysis methods. Included articles met all five quality assessment criteria. Fifteen were qualitative and 18 used mixed-methods designs.
Supplemental material
{kind=link}
PRISMA diagram.49 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses).
Initial reading of codes suggested a simple grouping of the data into descriptive themes of patient, provider, clinic and system-level outcomes. Further descriptive analysis identified cross-cutting themes within the data. Through an iterative process among the research group, a coding model was abstracted which described the role of QICs in general practice in four broad analytical themes: improving target topics, developing practices and providers, developing the health system and building QI capacity (table 1).
Analytical themes
Improving target topics
Target topics are those chosen as the focus of a collaborative. Target topics may be clinical outcomes, such as diabetes management or process outcomes, such as implementing models of care or interventions. Most included studies described positive changes in target topics.
Clinical outcome improvements reported included parameters such as glycated haemoglobin and cardiovascular risk factors.
Impressive improvements in Australian general practices participating in the Collaboratives include a 50% increase in the mean percentage of patients at target for glycaemic control and similar improvements in blood pressure and cholesterol targets. (Brown et al20)
Improvements were also reported in care processes such as daily weighing,21 colorectal cancer screening,22 immunisation23 and depression screening.24 Evidence of sustained change because of QIC involvement was provided by some studies.
During follow-up we found that most improvement changes were sustained more than 2 years after the last learning session. (Nease et al24)
However, some reported variability in making and sustaining change in practice culture and systems.
A similar proportion of the practices made no improvement or only transient improvement, whereas 20% demonstrated slow progress. (Donahue et al25)
Developing practices and providers
As described below, impacts were reported beyond the target topics, relating to practice organisations and their staff. Important impacts were reported in patient inclusion, administrative systems, patient care and teamwork. Provider impact appeared to be greatest on the small improvement teams delegated to attend the activities of the QIC. Outcomes included building skills and knowledge, and changes to motivation. Spillover to other members of the practice was described.26
Including patients in care
Improvements in patient education were reported in areas such as immunisation,23 diabetes,27 chronic kidney disease,28 medication management,21 depression29 and colorectal cancer screening.22 Activities included education sessions and the production of information resources. Increased patient self-management was reported.
Participants explained how increasing patient involvement and supporting self-management seemed to improve patient knowledge, adherence to treatment, and skills in self-management. (Harris et al27)
Reported patient experience outcomes were often related to improved access to care. Some described improved relationships with care teams.
Family satisfaction appeared to stem from better access, care, and safety, and having a strong relationship with their health care team. (McAllister et al30)
Improved care coordination was reported to result in saved time, reduction in unnecessary appointments and improved satisfaction.
We saved that family unnecessary visits and tests—that was a result of having a coordinator to help right the ship a little bit. (physician champion, practice 4) (McAllister et al30)
Some reported that teams had become more patient-centred through changes such as joint goal setting with patients and providing patients with more choices.
We have now become more patient-centric… depending on what the patients are wishing to do and how we can help them. (Harris et al27)
Administrative systems
Participants cited improvement in systems within their practice as a major benefit to participation. (Brown et al20)
Reported changes to financial systems included improved billing practices and growth in billing relative to costs. Some reported participation provided data which was used to approach insurance companies and external funders for increased funding.31
Better data management by practices leads to financial gains, because patients are better managed, and additional Medicare item numbers can be claimed. Improvements in staff and resource management have allowed for better patient access and improved finance. (Brown et al20)
Patient care
The use of disease registries was cited as a foundational improvement. This enabled the identification of populations of interest and clinical variation including patients not attending for care.
Central to the design was a patient registry and guideline-based work flow sheet that enabled physicians to track whether they are actually ‘doing’ what they ‘know’ as best care for their chronic disease patients. (Green et al32)
Some studies recorded a paradigm shift from reactive, episodic care to more active population management. Through systematic approaches, practices could become aware of patients with poor clinical measures or patients who were failing to attend for care.
Teams developed various strategies to systematically follow-up and track patients by developing diabetes registries, flow sheets and reminder systems in EMRs [electronic medical records], fostering a sense of improved care by ensuring appropriate and timely follow-up. (Harris et al22)
Other clinical process improvements reported included use of care coordination, care bundles, guidelines, care plans, patient tracking and care templates.
…programme participation had enabled them to identify suboptimal care in these areas and take action such as: clean up-related patient registers and improve identification of patients with LVSD [left ventricular systolic dysfunction]; optimise heart failure management through specialist clinics leading to reported improvements in, for example, New York Heart Association [NYHA], recording and increased pneumococcal vaccinations; implement more robust monitoring of medications and improved patient contacts and care education. (Bowie et al21)
Electronic medical records, while challenging to implement,22 were a key innovation credited with facilitating population management and seen as pivotal to achieving outcomes.
With this EMR, it’s so much easier to track patients that have been missed out of the system… (Taliani et al33)
Models of care such as the Chronic Care Model and the Patient Centred Medical Home were used in some studies to inform changes to care processes.
The unique combination of two evidence-based models, the expanded chronic care model, and the IHI [Institute for Healthcare Improvement] break-through series resulted in the critical integration of quality improvement and education to realize change in chronic disease care. (Green et al32)
Some noted little change as a result of the QIC.22 34
Improving teamwork
The inclusion of patients in the practice team was reported by some as an important outcome which could motivate the whole team. Though motivating, it required considerable effort to include consumers in care team processes.
…these new points of contact gave staff opportunities to glean insights or make contributions to patient care that might not otherwise happen. Practice staff observed that, for personal, social, or cultural reasons, patients sometimes preferred to disclose critical information to nonphysician members of the team. (Kyle et al35)
Physician champions found this parental involvement motivating but acknowledged that the recruitment, orientation, and engagement of parent partners were difficult. (McAllister et al30)
Improvements in practice team communication were also reported with particular reference to increased regular practice meetings and off-site meetings.
Some practices cited more effective communication channels within their practices, incorporating regular team meetings, as a positive outcome of the [Australian Primary Care Collaboratives] program.
GP007. “Previously, we had one, between one and four (meetings) a year, after Collaboratives we had more. Since last year we have them fortnightly”. (Brown et al20)
A common narrative was that QIC participation helped team members to get to know each other. Better understanding of each other’s roles led to increased trust. This empowered different members, including non-clinical staff, to work to their scope, develop as leaders and take on redistributed tasks.
Understanding each other’s role emerged as an important component of team building, and participants described experiencing more trust and respect among team members and fewer professional silos within their teams. (Harris et al22)
This task-shifting relieved some of the burden on physicians and felt rewarding to nonphysicians, contributing to a culture of mutual regard and respect, which in turn reinforced confidence in, and reduced discomfort with, the redistribution of tasks and responsibilities. (Kyle et al35)
Improved team functioning was reported to underpin improved patient care.
Team formation and continuous improvement efforts built on each other to help practices achieve effective team-based care. (Kyle et al35)
Building skills and knowledge
Participants described how the program gave them the knowledge, skills, and confidence to change how they deliver care. (Harris et al27)
Knowledge was reportedly gained in tools for care (eg, care plans, guidelines), clinical conditions (eg, chronic kidney disease, diabetes, screening), and local resources and services.
It has certainly increased my knowledge so hopefully we may have an increased knowledge I am delivering better patient care…[and]…made the doctors think a bit more on how they see their patients, how they read their patient’s records and what action they take. (practice nurse 2) (Bowie et al21)
Skills reported were in areas such as searching the electronic record21 and chronic disease care.36 For some, accrual of professional development ‘points’ was an important outcome promoting participation.
Interviewees….widely praised offering maintenance of certification (MOC) or continuing medical education (CME) credits—which provided ‘a big hook to bring in physicians,’ as one Idaho organizer put it. (Burton et al37)
Engagement or motivation
Increased motivation for change was attributed to numerous factors including the use of patient stories, the evidence-based nature of the collaborative interventions and evidence of better outcomes for patients. The most common and highly valued impact on motivation reported was from interaction with peers.
Far and away, the aspect of collaboratives that practices most frequently praised (in all 12 states) was learning from other practices, which typically occurred during in-person meetings, but sometimes also through practice-to-practice phone calls to troubleshoot issues or site visits to observe how another practice did. (Burton et al37)
It was the networking, the ability to get together with others who are passionate about improving health care and excited to work as a team towards making situations better for our patients. (PHC team) (Harris et al22)
Peer interaction provided moral support as well as access to new ideas. Sharing of successes, struggles and mistakes was highly valued. Some studies reported that participation had increased professional satisfaction28 30 38 39 and could empower individuals.
The coming together of multiple teams for off-site learning sessions (streams A and B) was described as the most effective activity because it facilitated interaction and created a sense of ‘togetherness’ that was enabling, energising, and motivating to tackle common challenges in QI. (Paquette-Warren et al40)
Hearing what other practices were doing motivated and invigorated practices and made change seem less daunting. (Burton et al37)
A common theme was the challenge of inspiring the rest of the practice to change.
…coming back to a busy practice back into all the time constraints and all the demands on your time to then try and pass on that energy is extremely difficult, that’s where a lot of it falters, it is actually very, very difficult to pass that on to the wider group. (Bowie et al21)
Participation in QICs was also reported to reduce motivation for change at times. Some factors cited included inadequate support, lack of remuneration, the lack of people to do improvement work, impact on personal time and competing priorities. Working in a team that did not know each other, or was resistant to change, discouraged some. Some studies reported concern about increased external oversight engendered by the sharing of practice data,20 competing priorities41 and loss of dedicated time.28
In teams where members did not know each other prior to the QIC, it was a very time-consuming process to reach a shared understanding of depression care and get clinicians engaged with the change process. (Franx et al42)
…practice members reported being overwhelmed with co-occurring events in the practice, such as electronic health record implementation or practice ownership changes. (Shaw et al41)
Developing the health system
System-level outcomes were identified beyond the borders of the participating practice organisations affecting the wider health system. Outcomes reported included improved regional practice support and the implementation of regional innovation.
Regional practice support
Local support is a key part of the QIC intervention. Respondents noted that for some practices, this commenced a relationship with a regional organisation for the first time.
For many practices this was their first WREN project, which meant that PBRN [Practice-based Research Networks] staff were facilitating the intervention at the same time they were building new relationships with staff. (Lipman and Aspy28)
Reported support included provision of customised data and feedback to practices, training in information technology skills, training in QI skills and development of change champions.
Interviewees considered [primary health care organisation] staff needed to play the role of coach and educator when facilitating QI work. When these roles were performed well, interviewees perceived this to result in better teamwork, more reliable data collection, and increased use of PDSA [plan, do, study, act]cycles, improved guideline use, development of change champions and sharing of success stories. (Hespe et al43)
This support role enabled regional organisations to understand general practice better including the management of chronic disease and reasons for variation in success in improvement.
The use of the breakthrough series approach provided significant insight into GPs’ [general practitioners] management of patients with a chronic disease. (Jones et al36)
Poor quality or inadequate support was reported to contribute to frustration, decreased engagement and disempowerment for some.
Finally, survey comments from a handful of sites conveyed frustration with a perceived lack of support and engagement from local leadership; respondents from these sites felt that frontline staff had no input into planning and decisions around PACT [the Patient Aligned Care Teams project] and described an excess of ‘administrative red tape’ that inhibited innovation at the team level. (Butler et al44)
Implementing regional innovation
Some articles reported QICs had been effective in implementing innovation at a regional level. Examples included depression care models, chronic disease strategies, safety improvement methods, use of disease registers and models such the Chronic Care Model and the Patient Centred Medical Home. Resources such as guideline flow sheets either developed by QIC participant or by regional organisations were disseminated.
QICs offer a potentially powerful way of disseminating health care innovations through enhanced strategies for learning and change. Creating collaborative environments in which diverse participants learn, listen, reflect, and share together can enable them to take back to their own organizations key messages and change strategies that benefit them the most. (Shaw et al45)
QICs were reported as a strategy for targeting disadvantaged communities in a region.
…the CHIPRA [Children’s Health Insurance Program Reinsurance Act] quality demonstration targets a diverse set of practices that typically serve relatively large proportions of children insured through Medicaid and CHIP, which generally have fewer resources than practices that serve commercially insured children. (Devers et al46)
Building QI capacity
An important reported impact of QICs was the building of QI capacity at all levels of general practice. Studies reported the inclusion of patients in QI activities, increased QI skills in practice team members, the creation of a QI culture in participating practices and the creation of QI capacity at a regional level.
Patients in QI
Some teams included patients in QI efforts through sharing of outcome data and targets. One study recorded strategies for increased patient involvement as an important outcome theme of their project.
Eleven of 12 practices developed formalized QI team processes including active parent partner participation. (McAllister et al30)
Oregon collaborative organisers had parents give presentations at collaborative meetings, which they told us received practices’ highest ratings in meeting evaluations. (Burton et al37)
Theme 2. More active and involved patients
Information letter/sheet to patients with, for example, explanations of target values.
Questionnaire sent to patients before the visit.
Working more actively with patients’ individual targets.
Introduction of Diasend, which transfers, stores and displays patient data from different types of glucose metres, insulin pumps and continuous glucose monitors.
Active smoking cessation.
Procedures for blood pressure measurement at home. (Peterson et al47)
QI knowledge and skills
Respondents described satisfaction from gaining QI knowledge and skills which enabled them to change the way they provide care.
Practice staff generally valued…Satisfaction from learning more about quality measures, QI concepts and techniques, critical medical home components, and how to identify [Patient Centred Medical Home] capacity and performance gaps. (Devers et al46)
They reported increased awareness of QI opportunities, skills in data use and skills in making systematic change.
Participants said that the program: increased their awareness of opportunities for QI; helped build their knowledge, skills, and confidence related to chronic care; provided motivation and support to reach their goals; taught them how to use data to focus their QI efforts; and enhanced their appreciation of the time, continued effort, and support required for system-level change. (Paquette-Warren et al40)
Establishing a QI culture
Some recorded culture change towards a belief in the efficacy of QI methods to make sustained change.
A benefit of the collaborative nature of the QI process, as experienced through the [Australian Primary Care Collaboratives], was the ability for primary care teams to share ideas and solutions for common problems, which helped to build a culture of ‘Improvement’ within practice teams. (Hespe et al43)
Contact with peers was cited as a strong motivator for improvement.
Physicians benefited from peer-based learning, identifying the learning collaborative as ‘what got them started’ using an ongoing QI process. (McAllister et al30)
Some reported institutionalising change through articulation in job descriptions, remuneration plans, policies and in leadership.
Transformed practices also began to include QI activities in job descriptions and compensation plans for staff, thus institutionalizing the practice transformation. (Donahue et al25)
A strong narrative emerged of ambivalence about formalised improvement cycles. Some practices saw them as key to improvement while others saw them as formal, contrived and unnecessary.
Using incremental, small-scale PDSA cycles was reported to be a key to successfully integrating changes into existing routines (Q8.12). (Gingold et al23)
In most cases participants did not continue to use formal PDSA cycles to make changes within their practices after their participation in the 18-month APCC [Australian Primary Care Collaboratives] program. Instead, many practices cited an ongoing ‘informal’ use that consisted of PDSA style thinking without writing a formal PDSA plan. (Brown et al20)
For some, participation in the QICs resulted in fatigue regarding QI. Improvement activities were described as extra work, often unremunerated, carried out at night and on weekends and therefore hard to sustain.
Participants indicated that time constraints and competing work priorities meant that they quickly lost momentum and motivation after initially implementing the PDSA cycle process to test changes in care practices. (Bowie et al21)
QICs were described as having a useful role in building QI capacity at the system level.
States and practices also seemed to agree that QI collaboratives and related activities may be necessary but are perhaps not sufficient to facilitate QI and [Patient Centred Medical Home] capacity improvement, suggesting the need for additional QI strategies. (Devers et al46)
Protected time
A strong theme from many articles was the positive impact of ‘protected time’, within the practice and in external QIC meetings, in which data could be reviewed and QI activities be carried out.
Protected time for clinical team meetings, and undertaking PDSAs and other quality improvement work was frequently cited as a key enabler for the Collaborative’s quality improvement processes. (Palmer et al48)
Provision of practice data
Many studies reported that QIC implementation led to the provision of practice-level data within regions. Regional-level data were reported as leveraging the competitive nature of clinicians through critical comparison. The provision of outcome data was reported to drive culture change through demonstrating gaps and improvements.
Interviewees in several states…thought that showing practices how they compared to their collaborative peers on selected quality measures helped promote healthy competition. (Burton et al37)
Data became a tool that enabled individuals and teams to make sense of their work and practice environment, visualising successes, and locating barriers. (Kyle et al35)
The impact of sharing feedback data on motivation for improvement was a key finding. (Lipman and Aspy28)
Improvement champions
An important reported capacity-building impact of QICs was the creation of peer champions and QI leaders who could promote change at the regional level.
Participating practices included clinical leaders from all PHOs [primary healthcare organisations] and some of these leaders are now working with their PHOs to extend the use of the Collaborative approach. (Palmer et al48)
Both Divisions reported that the project generated interest in the process as an educational tool at practice level, and both Divisions reported using ‘champions’ to promote, among other things, the use of care for chronic disease management. (Jones and Piterman34)
Discussion
Data in this review suggest an implementer or participant in a well-designed general practice QIC can expect a positive effect on a target topic. They should consider that as well as improving a target topic, a QIC can have a lasting impact on the professional lives of providers, on local practice organisations and at a system level. QICs can build QI capacity in the primary care system. These roles suggest that QICs are well matched to the improvement needs of general practice.
The data also indicate that poor QIC design and support may cause some participants to be discouraged and distrust QI methodologies. Implementers may consider that to extract maximum value from the implementation of a QIC in general practice, it should be designed to ensure effective peer interaction, provide high-quality local support, create real engagement with data and provide well-designed training in QI.
QICs in general practice were seen by participants to have a positive and sustained effect on the target topics addressed. The positive experiences described in this qualitative general practice data support general reviews by Schouten et al,2 Hulscher et al3 and Wells et al4 who found mostly positive effects on target topics in controlled studies. However, as in the general literature, not all collaborative projects included in this review found positive impacts on target topics. It is not clear from the current research which factors promote success. In the general practice context, organisations tend to be relatively small, may be under-resourced and more professionally isolated. Care should be taken to optimise implementation of the collaborative to take these factors into account. Participants highly valued peer interactions, access to data and local support which are discussed in more detail below. Maximising these is likely to increase success in improving target topics.
The data support a role for QICs in developing providers and the practice organisations in which they work. The effects on practices and providers are reported together because it is difficult to separate them in general practice. In small organisations like general practices, impact on providers can have profound impact on the organisation and vice versa. Identification of interventions which can impact general practices is crucial as health systems seek to become more efficient, effective and equitable through improved primary care.
Examples of reported roles of QICs in improving general practice organisations include improved communication, improved administrative, financial and care systems, and improved data collection and management. Disease registers and electronic medical records were noted as particularly important tools for improvement introduced through QICs. They support improved data collection which may in itself be an important outcome from participation in a QIC.
An important and consistent report was that QIC participation had improved teamwork in participating practices. Effects included improved relationships between team members, empowerment of non-physicians to work to their scope of practice and redistribution of tasks. Of particular note was the frequent comment that participation in QICs initiated practice meetings.
Providers described improved knowledge and skills in the target topic areas and introduction of specific tools to help improve care. Some studies also reported enhanced enjoyment of work and success in making change. Providers highly valued provision of time for improvement activities and the opportunity to meet with peers. Peer interaction was seen as effective in reducing isolation, increasing motivation and increasing learning. Some studies described the building of a community of practice which continued independently of the QICs. A strong motivator described was the provision of data for comparison and improvement. These findings align with aspects of the realist review of Zamboni et al6 which found participation in a QIC could improve health professionals’ knowledge, problem-solving skills and attitudes, teamwork and shared leadership.
The WHO and the Organisation for Economic Cooperation and Development have identified a pressing need for a primary care-led transformation of health systems.11 12 They call for a reorientation of primary care to become more person centred, multidisciplinary and population based. Data from this study indicate QICs may facilitate this transformation. Participants reported that involvement in QIC activities helped their teams move from reactively caring for individuals that presented to them, to proactively reaching out to the practice population with systematic care. QICs can have a role in helping practices promote self-care and become more patient centred. These changes align strongly with international recommendations for primary care reform.
QICs can facilitate region-wide skill development and implementation of models of care, guidelines and data collection. They can be a context for building understanding and relationships between regional coordinating organisations and general practices. They may be useful tools for focusing on specific aspects of integration of general practice with the wider health system.
QICs can increase understanding, motivation and skills in QI in patients, practice teams and at a regional level. Studies reported that QICs equipped participants to manage data and make systematic change. QI skills and behaviours could become institutionalised in some practices. Participation in QICs was credited with creating protected time for improvement work within practices and during external QIC activities. A major reported role for QICs was the establishment of systems to collect, feed back and respond to improvement data in general practice. At regional levels, QICs had a role in establishing QI champions who could influence change beyond the life of the QIC. It was noted that participation in a QIC could also have adverse effects causing fatigue and, in some cases, undermining confidence in QI strategies. It is likely that high-quality local support may counteract these effects.
Strengths
This study presents qualitative evidence of the role of QICs drawn from participants and implementers of QICs in general practice. The methodology used in the review has ensured the inclusion of most qualitative literature dealing with the topic. Quantitative evidence for QICs in general practice is limited. The understanding of processes gained through qualitative synthesis of the opinions and experience of actual participants and implementers is valuable and should be persuasive to those considering the role of QICs in general practice.
Weaknesses
While this review is methodologically sound, constrained resources challenged the handling of a large amount of data. The research team addressed this by adopting strategies designed to reduce bias. Sampling, standardisation and checking strategies were used in reviewing articles for inclusion. The search methodology and careful screening of studies were highly inclusive, but it is possible important studies have been left out. This review analysed qualitative literature and as such collated the views of subjects included in the original studies as well as the findings of the authors of those studies. Important views may have been missed in those studies.
The coding of qualitative data is necessarily a subjective process. While the review employed qualitative methodologies designed to enhance rigour, it may be that some data were excluded. Previous reviews of QICs have noted that the literature reporting them appears to be subject to positive biases of successful participants.2 It is possible that the research projects included in this review are overly positive about QICs due to selection bias in the samples interviewed and confirmation bias in the individuals themselves.
Conclusion
QICs have a role in general practice in improving target topics, developing practices and providers, developing the health system and building QI capacity. Care should be taken with implementation to maximise effectiveness in achieving all four outcomes.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Dr Hyun Song contributed to the article selection process of this review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @vitualis
Contributors AWK conceived of the article, coordinated the research group and wrote the first draft. All authors contributed to protocol development and implementation. All contributed to data analysis and writing of this article. AWK acts as guarantor for this review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.