Article Text

Abstract
Background In-hospital glycaemic management can reduce post-transplant morbidity, but is not always part of transplant care.
Objective We aimed to reduce the mean number of postoperative days in hyperglycaemia (≥2 blood glucose >12 mmol/L in 24 hours) in kidney and liver transplant recipients by 30%. We also aimed to reduce the mean number of days between transplant admission to endocrine consult by 2.0 days.
Design, setting, participants We conducted a quality improvement project in liver and kidney transplant recipients admitted to an academic transplant unit in Canada between 1 March 2019 and 1 May 2021.
Intervention We developed a bedside algorithm to monitor post-transplant capillary blood glucose; the algorithm also included thresholds for nursing-initiated inpatient endocrinology consultation.
Main outcome and measures We examined outcome (postoperative days in hyperglycaemia, days to inpatient endocrine consultation), process (nursing documentation of postoperative blood sugars) and balancing measures (nursing workload, postoperative days in hypoglycaemia) following implementation of our algorithm. We used Plan-Do-See-Act cycles to study three iterations of our algorithm, and used box plots to present outcomes before and after algorithm implementation.
Results In the pre-intervention period, 21 transplant recipients spent a mean of 4.1 (SD 2.4) postoperative days in hyperglycaemia before endocrine consultation. The mean number of days between hospital admission to endocrine consult was 10.7 (SD 13.0) days.
In the post-intervention period, we observed a 62% reduction in postoperative days in hyperglycaemia. The mean number of days between admission and endocrine consult was reduced by 6.3 days (59% reduction).
Conclusions Implementation of a simple, bedside algorithm for postoperative glucose monitoring and detection of hyperglycaemia in transplant patients, reduced the mean number of postoperative days in hyperglycaemia and time to inpatient endocrine consultation. Our algorithm continues to be used in our academic transplant unit.
- Healthcare quality improvement
- Hospital medicine
- Diabetes mellitus
- Nurses
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request to KKC.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Hyperglycaemia is common following solid-organ transplant; patients are prescribed immunosuppressive drugs, use enteral/parenteral nutrition, experience surgical stress and postoperative infection and may have underlying obesity and diabetes.1 In a study of 424 kidney transplant recipients in the USA, 87% of those without diabetes, and 100% of those with pre-existing diabetes, had at least one blood sugar >11 mmol/L (≥200 mg/dL) or received a dose of insulin during their hospital stay.2 Post-transplant diabetes mellitus (PTDM, new onset diabetes following transplant), is also very common, with a reported incidence of 10%–40% in the first 3 years after surgery.3 4
Post-transplant hyperglycaemia is important to mitigate; hyperglycaemia is associated with morbidity including ischaemia reperfusion injury and delayed graft function after kidney transplant.5 PTDM has been linked with reduced patient and graft survival and an increased risk of cardiovascular disease and infection.6 Moreover, post-transplant hyperglycaemia can heighten the risk of mortality in transplant recipients.7
In-hospital management of post-transplant hyperglycaemia including early administration of insulin, initiation of oral/injectable medications and lifestyle counselling, can reduce blood glucose (BG), PTDM risk, weight and fat mass.4 8–10 Unfortunately, hyperglycaemia management is not always part of routine post-transplant care. Transplant teams are often focused on the health of the transplanted graft, and may under-recognise or not address abnormal glucose values.
Inpatient endocrinology teams might have an important role to play in post-transplant care. They can educate patients with hyperglycaemia, promote early initiation of antihyperglycaemic medications and anticipate and manage high and low sugars,1 11 12 particularly when patients’ kidney function fluctuates and when immunosuppressants are changed or started.13 In this quality improvement (QI) project, we aimed to reduce postoperative days in hyperglycaemia and time to inpatient endocrine consultation with a bedside algorithm that both captured BG, and defined clear parameters for endocrine consultation.
Methods
We used the SQUIRE guidelines V.2.0 for the reporting of QI projects (online supplemental appendix table 1).14
Supplemental material
Setting
This study was conducted in an academic transplant unit at a large tertiary care hospital in Canada. The transplant unit performs about 200 solid organ transplants annually.15
At baseline, patients admitted to the unit for liver or kidney transplant had computer-based postoperative orders entered by a transplant physician, fellow or resident. Those with pre-existing diabetes had monitoring of capillary BG before meals, with a standard insulin correction scale to use if BG were high. Those without a history of diabetes had a venous BG drawn with their daily blood work. Transplant physicians and surgeons would use clinical judgement to act on postoperative hypo or hyperglycaemia, and request an inpatient endocrine consultation at their clinical discretion.
The inpatient endocrinology consult service is based out of another academic hospital within the city. The service is available for consultations in the transplant unit 24 hours a day. The endocrinology consult service includes residents, clinical fellows, diabetes nurse educators and an attending endocrinologist. The team manages hyperglycaemia (initiation or adjustment of insulin or oral/injectable medications) and educates patients about diabetes, the safe use of insulin, and the prevention of hypo and hyperglycaemia.
Patients
Our study included all patients admitted to the transplant unit following liver or kidney transplantation between March 2019 and April 2021. We included patients with or without a prior history of diabetes. We excluded those admitted for reasons apart from new transplantation (eg, admission for graft failure or sepsis).
Ethical issues
This project was classified as a QI investigation based on the requirements listed in the Tri-Council Policy Statement. Ethics approval was waived by our local research ethics board. All patients had confidential information protected.
Baseline assessment
Our baseline data collection took place between 1 March 2019 and 1 August 2019. We captured the number of postoperative days kidney and liver transplant patients spent in hyperglycaemia (≥2 BG >12 mmol/L) . We chose this definition of hyperglycaemia to balance postoperative targets for hyperglycaemia (guidelines typically recommend postoperative BG 5–10 mmol/L),16 with values that our endocrine and stakeholder team felt should be ‘actionable’ during postoperative stay (higher BG). We also captured the time between admission to the unit, and in-hospital endocrinology consultation.
Aim statements
Our primary aim was to reduce the mean number of postoperative days in hyperglycaemia (≥2 (BG)>12 mmol/L) in kidney and liver transplant recipients by 30%. Our secondary aim was to reduce the mean number of days between transplant admission and inpatient endocrine consultation by 2.0 days.
Root cause analysis
We used a Fishbone diagram (online supplemental appendix figure 1) to conceptualise root causes for post-transplant hyperglycaemia and reasons for delay in endocrinology consultation. This analysis was conducted alongside key project stakeholders including endocrinologists, endocrine fellows, hepatologists, nephrologists, transplant surgeons, nurses, care coordinators and QI leads. Our stakeholder team felt that a major cause of prolonged duration of hyperglycaemia was that the transplant team was focused on post-surgical issues apart from hyperglycaemia (eg, health of graft, infections). Moreover, there was uncertainty regarding consultation etiquette (ie, degree of hyperglycaemia that is ‘worthy’ of in-hospital, specialist assessment).
Intervention
Based on our root cause analysis, we created an intervention pick board (online supplemental appendix figure 2) to conceptualise potential tests of change (ie, interventions). We prioritised the development of a paper-based, easy-to-use bedside algorithm to facilitate postoperative glycaemic monitoring, capture of hyperglycaemia, and inpatient endocrine consultation. Our hope was that this algorithm would not only facilitate the transplant team’s awareness of hyperglycaemia, but alleviate concerns regarding consultation appropriateness, reduce care burden on transplant services and promote earlier glycaemic intervention. Stakeholders felt it extremely important for nurses to be empowered to request consultations directly from the endocrine service.
Our bedside algorithm is illustrated in online supplemental appendix figure 3 and 4. Key features are the following:
Patients with a kidney or liver transplant have a capillary BG every 6 hours (if not eating) or before meals and at bedtime (if eating) for 10 days.
An endocrinology consultation is triggered by the transplant nurse based on the following:
For postoperative days (POD) 0–2, if there are two readings with BG >15.0 mM in any 24-hour period, the inpatient endocrinology team will be called the next morning for new consultation.
From POD 3 and onward, if there are two readings with BG >12.0 mM in any day, the inpatient endocrinology team will be called the next morning for new consultation.
We decided against implementing a protocol for insulin administration by the inpatient endocrinology team. This is because insulin treatment regimens can be highly variable among transplant patients depending on the clinical circumstance (pre-existing diabetes, variable kidney function, immunosuppression regimen, corticosteroid and other immunosuppressants, severity of obesity),1 patient circumstances (eg, cognition), family supports, social situation and patient preferences.
Family of measures
In addition to capturing outcome measures (mean number of days in hyperglycaemia and mean number of days in hyperglycaemia before inpatient endocrine consultation), we assessed both process and balancing measures. Process measures included nursing documentation of postoperative BG. Balancing measures included number of POD with hypoglycaemia (defined by ≥1 BG <4 mmol/L per day), and nursing workload following implementation of the intervention.
Analysis
We summarised the characteristics of pre-intervention and post-intervention patients descriptively using Microsoft Excel (numbers and percentages, means, SDs or SD). We used Plan-Do-See-Act (PDSA) cycles with multiple iterative steps to collect data through project implementation. We used QI macros and Microsoft Excel for analysis including the creation of box plots. We elicited routine feedback from project stakeholders through routine team meetings and email correspondence throughout implementation.
Results
The baseline characteristics of the 21 pre-intervention patients are shown in table 1. There was no missing data. There was variation in days to endocrine consultation in the pre-intervention period with liver transplant patients on average having a longer time to endocrinology consultation.
Characteristics of liver and kidney transplant recipients pre-intervention
Implementation of algorithm
We aimed to implement our intervention in the spring of 2020. However, at this time, the first wave of the COVID-19 pandemic hit our region, and transplant surgeries slowed, in-hospital consultations moved quickly to remote visits, and hospitals became extremely burdened. Stakeholders decided to delay the start of our study to September 2020.
In early September 2020, we implemented our algorithm (PDSA 1). At the time of initial implementation, endocrine consultations took place remotely (telephone) with both the nurses, followed by the patient.
Within a few weeks of implementation, bedside nursing staff communicated that the algorithm led to increased workload due to multiple patient phone calls to support remote consultations (balancing measure). Where infection control practices would allow, and personal protective equipment was available, we converted our consults back to face-to-face visits (PDSA 2) which improved our efficiency. Then in January 2021, bedside nurses noted that checking BGs for a full 10 days following transplant did not appear necessary (ie, there were no new days in hyperglycaemia noted after 5 days of monitoring). BG monitoring up to 10 days also increased nursing workload. As a result, we limited postoperative BG monitoring to days 0–5. This third test of change was implemented as PDSA 3.
Post-implementation
The characteristics of patients included in the post-intervention period are illustrated in table 2. There was no missing data.
Characteristics of liver and kidney transplant recipients post-intervention
The total number of POD in hyperglycaemia pre-intervention and post-intervention is shown in figure 1. With implementation of our algorithm we noted a reduction in POD in postoperative hyperglycaemia by 59%.

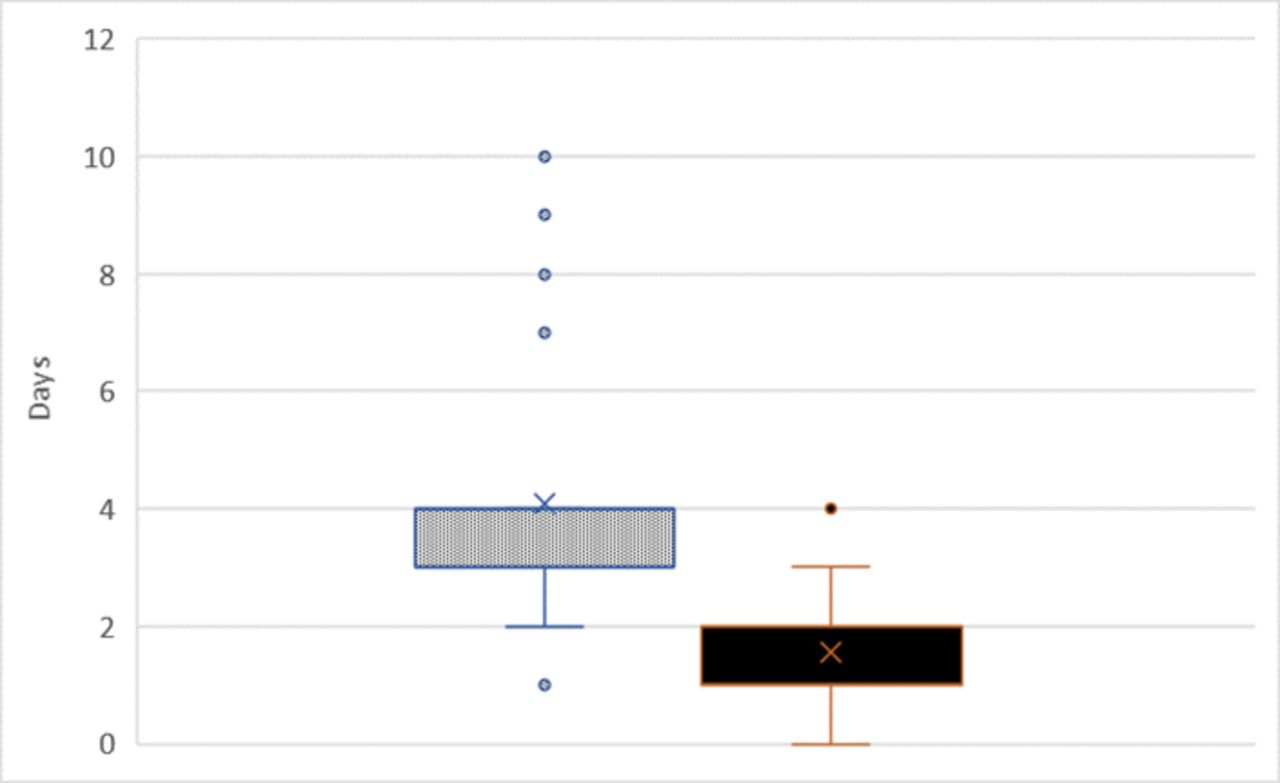{kind=link}
Box plot of mean number of postoperative days in hyperglycaemia before and after intervention. Shaded box represents pre-intervention period, solid box represents post-intervention period.
The total number of days between admission to inpatient endocrine consultation before and after the intervention is shown in online supplemental appendix figure 5. With implementation of our algorithm, time to endocrine consultation was reduced by a mean of 6.3 days. There was no appreciable difference in the mean number of POD spent in hypoglycaemia following implementation of the intervention (mean days in hypoglycaemia was 0.5 (SD 1.4) and 0.3 (SD 0.7) days in the pre-intervention and post-intervention periods, respectively).
Discussion
Main findings
In this QI project conducted in a Canadian academic transplant centre, we found that implementation of a standard algorithm for post-transplant hyperglycaemia reduced time in hyperglycaemia and facilitated a quicker referral for inpatient diabetes care. With some modification, we were able to continue this algorithm during the first, second and third waves of the COVID-19 pandemic in our province.
Although clinical practice guidelines recognise the importance of inpatient glycaemic control,17 we were only able to identify one other QI study on postoperative hyperglycaemia following kidney or liver transplantation. In a Midwestern US transplant centre (2016), investigators studied the utility of a nurse-driven clinical pathway with established criteria for endocrinology consultation in liver and kidney transplant recipients. While the study found that the clinical pathway promoted inpatient endocrinology referral, there were only 30 patients included over a 1-month period. Moreover, the pathway did not include guidelines for monitoring hyperglycaemia, nor standard criteria for endocrine consultation. It was up to the transplant team to call in a consultation based on their discretion.18 There was also no data on the sustainability of the intervention.
Strengths and weaknesses
We chose a strong intervention (algorithm) that was easy to use, did not require technology or electronic order sets, and could be executed in both a virtual and in-person clinical environment. It respected the principle of immediate advantage (ie, made everybody’s job easier in some way). The nurses had more autonomy, physicians had some cognitive load relieved, and the inpatient endocrine team got involved in patient care earlier. An additional strength was our ongoing engagement with nursing and transplant teams throughout the duration of this project.
In terms of limitations, we do recognise that our BG threshold for endocrine consultation was high and partially subjective (ie, BG >12 mmol/L). However, we felt that this BG threshold would provide the optimal balance between clinical practice guidelines, the volume of patient referrals to our team, and the influence of infection and stress on BG values. We did not formally survey staff about their experience with our algorithm, but maintained close communications with transplant/nursing teams and leaders throughout implementation. Our work was also delayed by the COVID-19 pandemic. The results are also limited to our tertiary care transplant centre in Canada.
Conclusions
Using a multidisciplinary QI approach, we reduced the number of days in hyperglycaemia and the time to inpatient endocrine consultation in kidney and liver transplant recipients. Our algorithm may not only reduce post-transplant morbidity, but has supported the surgeons, physicians and nurses who manage ill and often complex patients. This algorithm will continue to be used in our Canadian transplant unit.
Data availability statement
Data are available upon reasonable request. Data are available upon reasonable request to KKC.
Ethics statements
Patient consent for publication
Ethics approval
This project was classified as a quality improvement project. Ethics approval was waived by our local research ethics board.
Acknowledgments
We thank Endocrinology Fellows Sharon Lee, Stephanie Lubchansky, Jooho Lee, Parul Khanna, Raymond Li and Ryan Findlay for helping to advance this work.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @KristinKClemens, @agob2007
Contributors KKC conceptualised the study, performed parts of the analysis, interpreted results and drafted the manuscript. MB conceptualised the study, interpreted results and reviewed the manuscript critically. CW and KL helped develop the project, interpreted results and reviewed the manuscript. HR developed the study, interpreted results, contributed to the literature review and aided with the development of the manuscript. AB conceptualised the study, interpreted results and reviewed the manuscript. AG conceptualised the study, supervised trainees, performed the analysis, interpreted results and reviewed the manuscript. KKC is the guarantor of the study and accepts full responsibility for the work and/or conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Unrelated to this work, KKC has attended conferences sponsored by Merck. She has received honoraria for providing Certified Medical Education talks from Sutherland Global Services Canada, the Canadian Medical and Surgical Knowledge Translation Research Group and the CPD Network. There are no other conflicts to disclose.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.