Article Text

Abstract
During the COVID-19 pandemic, patients were apprehensive to seek acute care resulting in delayed diagnoses of serious conditions and reduction in emergency room (ER) visits by 50% in the Fraser Health Authority. Patients who did present to the ER left prior to their results being available and some refused admission and critical treatments.
At the Chilliwack General Hospital ER, a virtual care clinic was established to follow-up on patients after their initial ER visit, providing test results and ensuring patients are not clinically deteriorating at home. Specific criteria were created for safe referral to virtual follow-up. For 2 hours daily, an ER physician contacts selected patients by telephone to provide a virtual follow-up based on the patients’ needs.
Through the emergency department virtual care (EVC) pilot project, from May 14 to August 31, 2020, on average 58 telehealth visits were conducted weekly, with 19% of visits reaching unattached patients without a regular primary care provider. A patient survey revealed that 75% of respondents were very satisfied or satisfied with telephone virtual care as a follow-up to their emergency department (ED) visit, while 95% would like to continue to receive telephone follow-up care. Additionally, based on a physician survey, 80% of providers were satisfied or very satisfied with the overall EVC experience. The majority (80%) would like to continue to provide the service. One patient was referred for a virtual care follow-up for imaging results that did not meet the referral criteria; the patient was diagnosed with a perforated appendicitis. They had an atypical presentation of abdominal pain and their care was delayed by several hours than if they were to present to the ED for in-person follow-up. The process and referral criteria may require minor modification and must be followed strictly to ensure safety and efficiency in providing telehealth follow-up in the acute care setting.
- COVID-19
- emergency department
- healthcare quality improvement
- telemedicine
Data availability statement
Data are available on reasonable request. Supplemental data is available on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Problem description
Patients are afraid of accessing acute care services due to concerns of exposure to COVID-19.1 This is resulting in delayed diagnoses and treatment of serious medical conditions (eg, perforated appendicitis, strokes, haemorrhages, infections, heart disease). Some of the patients who present to the emergency department (ED) are anxious about the wait and leave prior to being cleared by a physician with pending laboratory and imaging results. Furthermore, with infection control and personal protective measures, patients are occupying an ED bed for long periods of time, thus limiting flow.
Available knowledge
Emergency telehealth care has predominantly involved consultation between specialists and emergency room (ER) physicians to support rural communities in the provision of acute care services, such as telestroke or tele-ICU (intensive care unit).2–5 The few studies of physician-to-patient virtual care in the acute care setting have demonstrated the safety and benefits of telehealth.6 7
Dadosky et al7 showed that telemanagement of heart failure patients in the postacute care continuum reduced rehospitalisation rates. Similarly, Davis et al8 used telemonitoring in a transitional care model following an acute event to show a reduction in all-cause 30-day readmissions by up to 50% with potential to reduce long-term acute care utilisation.
Player et al9 also attest to the quality of care that can be provided using telehealth. By comparing telehealth visits to in-person visits of common acute conditions, they report that the majority (81.5%) of in-person follow-ups did not result in diagnosis changes while most patients (92%) agreed that the telehealth visit had replaced an in-person visit.
Several studies have shown that telehealth can be successfully used by vulnerable and complex populations, such as the elderly, palliative and mental health patients10–12, as well as children with special needs.13
As for the patient perspective, Robinson et al14 report that based on acute telemedical care in an ED, 80% of patients were satisfied with the explanation of their medical condition and their treatment.
During the start of the COVID-19 pandemic in March and April 2020, ED visits in the Fraser Health Authority (FHA) decreased by 50%. At the same time, there was no established telehealth procedure in place to support patients who may have been seen in the ED but left prior to medical clearance, refused admission or needed prompt follow-up. Notably, the Ministry of Health (British Columbia, Canada) approved billing guidelines for ER physicians to be compensated for telehealth visits.
Rationale
If select patients had virtual care follow-up with an ER physician, then this would improve patient access to acute care thereby decreasing ED congestion from revisitation, as well as improving patient outcomes and satisfaction. Virtual follow-up visits would provide clinical reassessment, as well as access to laboratory and imaging results, which is beneficial for unattached patients and those patients whose primary care providers are not accessible in a timely manner. Furthermore, as these patients do not have to wait in the ED for results or return for follow-up the next day, this improves ED flow and alleviates patients’ apprehension about being exposed to COVID-19 in the hospital.
During the COVID-19 pandemic, the demand and financial resources for virtual healthcare increased; as a result, this initiative was implemented with support from senior leadership, front-line staff and patients.
Specific aim
The specific aim of this quality improvement initiative is:
To improve follow-up care for patients presenting to the Chilliwack General Hospital (CGH) ED with a Canadian Triage and Acuity Scale (CTAS) of 3, 4 and 5, specifically for unattached patients and those returning for imaging study results, from 14 May 2020 to 31 August 2020.
Methods
Context
During the COVID-19 pandemic, ED volumes were reduced by 50% in the Fraser Health region predominantly due to concerns about healthcare exposure. Furthermore, some patients who did present to the ED were apprehensive and left prior to test results and treatment, and occasionally declined admission where indicated. This in turn led to delayed presentations of serious illness, including strokes, myocardial infarction and infections.
Beyond the trepidations of the COVID-19 pandemic, it has been shown that patients recall only 49% of the recommendation provided by their doctor.14 Other patients bounceback within a few days due to progression of their illness, poor pain control or being advised by the attending physician to return for a follow-up depending on their access to a family physician. At the CGH ED, on average precovid, 39 daily patient visits were repeat visits for urgent imaging test results (30 daily visits during the first COVID-19 wave). This is due to limited access to same day imaging. There was also a 12% bounceback rate within 72 hours for all ED visits. Returning to the ED for in-person follow-up confers several inconveniences to patients, including long wait times, missed time from work or family responsibilities, and the need to arrange for transportation. This also leads to increased ED crowding.
Another important consideration is that infection control measures, such as social distancing, room deep cleaning and wearing personal protective equipment, have led to less efficient flow of patients through the ED. As volumes start to increase after the first wave of COVID-19, patient flow and space limitation will be a concern.
The CGH ED caters to a small and fast-growing community of over 113 000 people according to the 2021 Canadian census.15 On average 16% of patients attending the ED are unattached to a primary care provider in the community. For attached patients, there is limited after-hours and weekend care by primary care providers. A large proportion of patients especially the elderly and those of lower socioeconomic status have limited access to transportation.16 Given these barriers to access of care in Chilliwack, an ED virtual care follow-up clinic pilot was created.
A committee was established to design the virtual care follow-up process that consisted of ER physicians, family physicians, department managers, senior executive leaders, and registration and unit clerks. Some challenges arose related to devising a schedule that can be integrated with the existing physician rotation without increasing burden on physicians and nurses. Also, family physicians were concerned that this service would create disruption of continuity of care for their patients. The follow-up process was designed to align with existing primary care follow-up in the community. The follow-up clinic would provide after-hours care to patients that could not access their primary care providers in a timely manner. In addition, collaboration with the radiology department allowed for urgent next-day imaging results for a select patient population to be provided virtually to prevent long ED waits for imaging results.
Intervention(s)
In the CGH ED, a virtual follow-up clinic was implemented. A designated 2-hour virtual care shift (from 17:00 to 19:00 hours daily) was added to the schedule where a physician will call high-risk patients to follow up on their clinical status and to provide laboratory or imaging results.
Patients are selected for a virtual follow-up by the attending physician who assessed the patient at their initial ED visit. If the patient is deemed to be suitable for virtual follow-up at the attending physician’s discretion, then verbal permission from the patient is obtained for virtual follow-up, their contact number is confirmed and an appointment is arranged. The appointment is logged in a binder under a specific date and the patient is provided a discharge card with information about the date and time of their follow-up.
For imaging test results, specific criteria were established (figure 1) as a guide for studies appropriate for virtual follow-up. For example, patients over the age of 50 with undifferentiated abdominal pain were exempt from receiving imaging results virtually as they often require repeat physical examination and are likely to require in-person management of acute pathology.

Criteria for CGH ED virtual care imaging results follow-up. CGH, Chilliwack General Hospital; ED, emergency department; AST, aspartate aminotransferase; ALT, alanine aminotransferase; TIA, transient ischemic attack; ERP, emergency room physician.
For documentation, the night shift registration clerks create ‘Telehealth Follow-up’ charts for the next day’s virtual care clinic where the physician can document their telephone follow-up notes and orders. Orders are processed by the unit clerks. When complete, the telehealth charts are scanned into the Meditech Electronic Medical Record as are all other ER patient records.
Study of the intervention(s)
To assess the impact of the ED virtual care (EVC) clinic follow-up, the average ED length of stay (LOS) for CTAS 3, 4 and 5 patients were reviewed over the pilot period of 14 May to 31 August 2020. In addition, the number of weekly telehealth visits and the number of unattached patients virtual follow-up visits were tracked.
In order to assess satisfaction with the EVC clinic procedure, a physician survey was conducted consisting of five questions exploring the physician satisfaction and interest in continuing to provide the service. To understand the patient experience, a four-question telephone survey was carried out a couple of weeks following the virtual follow-up visit. Furthermore, physicians were asked to report of any safety concerns or missed diagnoses that may have resulted due to inappropriate virtual care follow-up.
To evaluate the use of the EVC clinic for imaging follow-up results, a random sampling of the number of imaging study results followed up at the EVC was tracked over the pilot period.
Measures
Outcome measures
Total number of virtual visits/week.
Number of unattached patient virtual visits.
Number of virtual visits/day for non-critical imaging results.
Process measures
Patient satisfaction.
Physician satisfaction.
Balancing measures
Number of negative patient outcomes.
Number of in-person visits/day for non-critical imaging results.
Fifteen-day ER revisit rate.
Data from Meditech were collected for the number of telehealth visits and unattached patient follow-up visits, as well as ED LOS data.
An online survey tool was used to administer the anonymous physician survey.
The patient survey was conducted over the telephone by a trained volunteer, using a standardised script. All questions were asked using a Likert scale and results entered into an Excel spreadsheet.
The imaging study follow-up data were manually counted from a daily summary sheet for the clinic that highlights the reason for referral for follow-up. Random dates over the study period were selected.
Analysis
The data was analysed using SQC Pack. The accuracy of the data is contingent on the integrity of the information in Meditech. For the purposes of this study, the number of telehealth visits and the average LOS by CTAS level is deemed to be relatively reliable information.
The ARECCI Ethics Guideline for Quality Improvement and Evaluation Projects was completed with a score of 23 and a second opinion review was recommended and completed.
There were two areas of concern for somewhat more than minimal risk:
That this is an original or novel process for which it would be difficult to establish a balance of risk and benefit in advance.
That there may be a significant departure from the routine care, programme, or service provided to participants or the gathering of information about participants beyond that normally collected.
In order to address these concerns, a plan was established with stakeholders to track and follow-up with negative patient outcomes for EVC participants in a timely manner. Also, strict EVC clinic criteria were created to ensure that there were safety checkpoints in place in advance. Patients were asked whether they would prefer an in-person or telephone follow-up prior to discharge. ER physicians were instructed to have a low threshold for asking patients to return to the ED in person in the event they cannot provide sufficient care remotely.
Telephone follow-up was selected as the modality for virtual follow-up as most people have access to a telephone and it requires little technical skills to operate. Several Plan-Do-Study-Act (PDSA) cycles were conducted by different ER physicians in order to create the EVC process before it rolled out to the rest of the department.
The telephone volunteer was provided with a script and list of resources for addressing any questions that may arise from patients during the interview. The physician quality improvement team reviewed the survey questions to ensure all survey best practices are met and that the questions support the measures.
Results
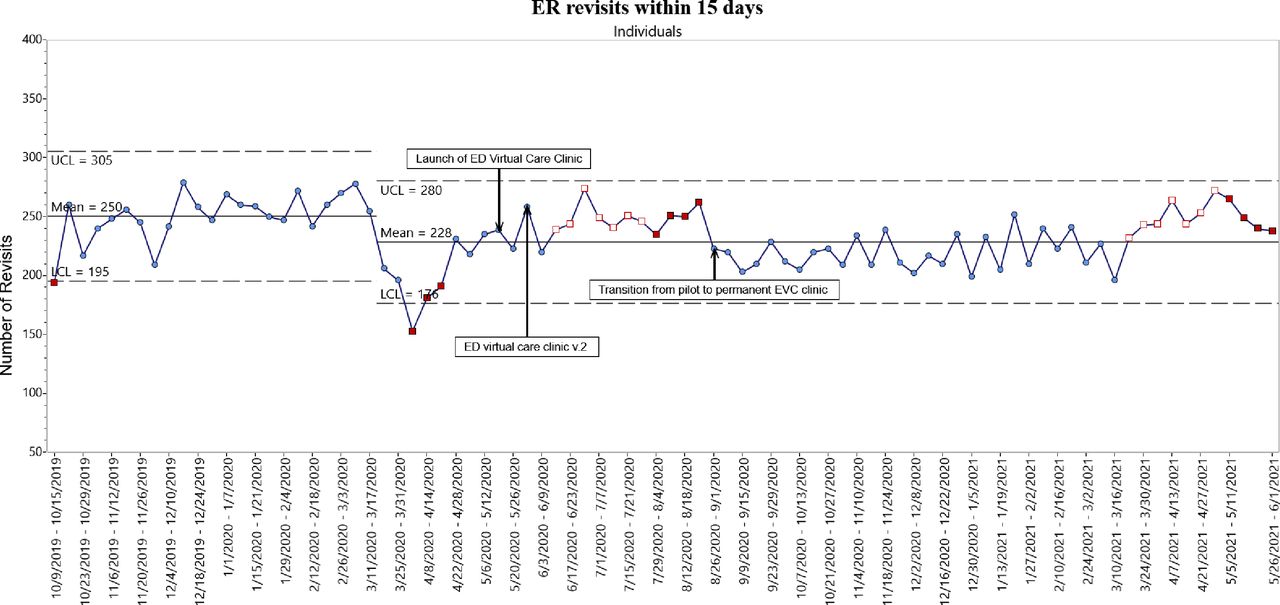
The EVC clinic pilot project took place from 14 May to 31 August 2020. On average, 58 telehealth visits were conducted weekly. Eight to 20 unattached patients received telehealth follow-up weekly, who otherwise may have limited access to primary care. On average, 26% of imaging study results were delivered virtually based on random sampling. Figure 2 demonstrates that following initiation of the EVC, the number of ER visits for imaging results was reduced compared with pre-COVID. Figure 3 shows ER Revisits within 15 days which decreased from pre-COVID and after initiation of the EVC. However, this number is climbing back up since April, which may be due to the third wave of COVID-19.
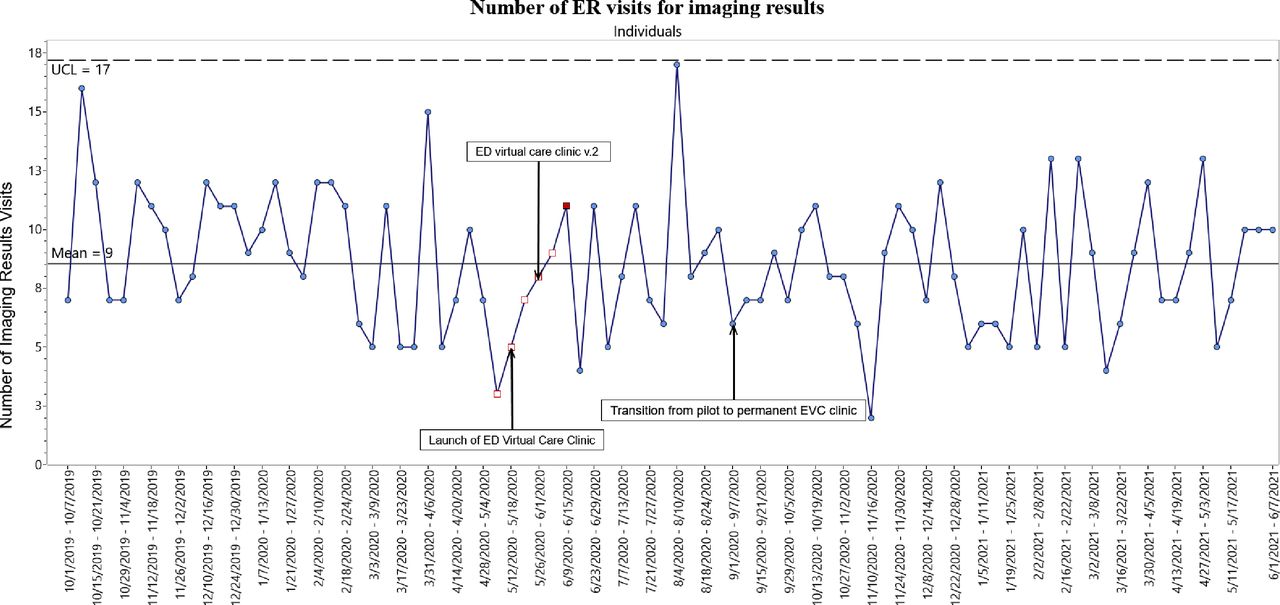
Number of ER visits for imaging results. ED, emergency department; ER, emergency room; EVC, emergency department virtual care; UCL, upper control limit.

{kind=link}
{kind=link}
{kind=link}
ER visits within 15 days. ED, emergency department; ER, emergency room; EVC, emergency department virtual care; UCL, upper control limit; LCL, lower control limit.
For the patient survey, 154 patients were contacted, 88 patients consented to and completed the survey with a 57% response rate. Seventy-five percent (75%) of respondents were very satisfied or satisfied with telephone virtual care as a follow-up to their ED visit. Sixty percent (60%) of patients strongly agreed while 25% agreed that they understood the explanation of their condition that was provided during the telephone follow-up. Finally, 95% of patients would like to continue to receive telephone follow-up care from the Chilliwack ED in the future.
The physician survey was completed by 15 ER physicians (68% response rate). Eighty percent (80%) were either satisfied or very satisfied with their overall experience as EVC providers and 80% found value in providing virtual follow-up care. The challenges physicians encountered with the EVC are inability to reach patients (55%), too few patients per clinic (20%), inability to arrange appropriate follow-up (20%) and too many patients per clinic (5%). In terms of future direction, 80% of physicians would like to continue providing the virtual care follow-up clinic, while 13% were neutral and one physician did not want to be involved. The majority wanted to continue to provide the EVC shift as an additional 2 hours attached to the evening shift.
Of the hundreds of EVC follow-up visits conducted in the pilot period, one case was identified by the provider as a potential safety concern. A patient was referred for virtual follow-up of an abdomen and pelvis CT result where they were found to have a perforated appendicitis. Of note, the presentation was atypical and the physical exam did not consist of peritoneal signs but this follow-up would have been more appropriate for an in-person visit given the undifferentiated nature of the pain. The concerns were discussed with the physician group at the monthly department meeting.
Of note, there were a few cancer diagnoses made by telephone follow-up where a malignancy was suspected on X-ray and a CT was advised. In these cases, patients were made aware of the initial imaging result and consented in advance to have the CT imaging result provided virtually. In some cases, it may have even been more appropriate for patients to be near their families when the results were delivered instead of alone in the exam room due to visitation restrictions during the COVID-19 pandemic.
Discussion
Summary
Overall, the EVC pilot project was successful in connecting patients virtually to a physician for follow-up of acute care illnesses and in assisting to streamline ED flow for a subgroup of patients returning to the ED for imaging test results. On average, 58 telehealth follow-up visits were conducted weekly, of which 19% were unattached patients who have even less access to primary care in the midst of the COVID-19 pandemic.
The majority of patients reported that they were satisfied with the telephone follow-up (75%) and 95% wanted to continue to receive the service in the future. Likewise, the provider experience was also optimistic with 80% of physicians being satisfied with the overall experience that the follow-up clinic provided and 80% expressed interest in continuing to provide follow-up care virtually.
Interpretation
The number of telehealth visits conducted weekly and the unattached patient visits through the EVC reflect a need in the Chilliwack community for after hours and weekend care when family physician clinics are not available to provide follow-up. Patients were given a choice to follow up with their family physicians or nurse practitioners within 1–2 days when possible. There are several local family physicians who work part time or have large practices with longer wait times. The EVC can collaborate with and support those primary care providers and their patients as needed. The EVC continues to fill this gap in care through 2021 and 2022.
Imaging study and laboratory results follow-up were integrated into the design of the EVC in order to streamline ED flow and for patient convenience. Up to nine patient visits daily were diverted through the EVC for follow-up of imaging test results, and a process was built in to the EVC to follow-up on laboratory test results, such as wound, aspirate and urine cultures, as well as COVID-19 test results. This improves quality of care and promotes safe practice for our physician group.
Limitations
There was one patient safety case that was brought forward as an inappropriate follow-up for the virtual clinic with a delayed diagnosis of atypical perforated appendicitis. The patient was asked to return to the ED on the same evening and was assessed by a general surgeon and admitted to hospital. This case was brought forward to the ER physician group and the EVC referral criteria were reviewed. Unfortunately, despite a stringent criteria to prevent inappropriate referrals, some unexpected diagnoses may still present to the EVC, which will continue to be addressed on a case-by-case basis with modification of the referral criteria as needed.
One limitation worth mentioning is that although the patient survey was conducted by a non-medical volunteer and patients were informed ahead of time that their answers will not affect their care, there may have been acquiescence or desirability bias in their responses.
Another limitation of the study is that it was conducted in a single community centre but there are other hospitals in the Fraser Health Region that are interested in introducing a formal virtual care follow-up process to their departments and may consider applying the process outlined in this study.
Conclusions
The EVC project has been permanently integrated into the CGH ED workflow and continues to be well received by patients and physicians through the ongoing phases of the global pandemic.
Next steps being considered are the creation of an attachment mechanism for unattached patients to a primary care provider in the community. In addition, sustainability and spread across the Fraser Health region is a direction being explored currently in the context of the ongoing pandemic and beyond.
Data availability statement
Data are available on reasonable request. Supplemental data is available on request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but the process used in the article underwent A pRoject Ethics Community Consensus Initiative (ARECCI) assessment. It required a second opinion review which was conducted by physician quality improvement programme certified reviewers. Their suggestions were applied in the final protocol.
Footnotes
Contributors Guarantor: DE-Z. Conceptualisation and methodology: DE-Z. Data collection and patient interviews: JE, DE-Z, TS. Data analysis and graph preparation: JE. Original draft preparation: DE-Z. Review and editing: RJ, JE, DE-Z. CGH ED Physicians: participation in virtual care clinic and survey. Virtual care clinic patients: completion of survey.
Funding Fraser Health Physician Quality Improvement Programme—No award/grant number. Chilliwack Medical Staff Association—No award/grant number.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.