Article Text

Statistics from Altmetric.com
Introduction
Vaccine uptake has been a long-standing challenge in public health spanning a wide array of patients and diseases,1 but the need to identify and address barriers to vaccine utilisation has never been more apparent for our generation than during the COVID-19 era. Even when effective vaccines are available, challenges surrounding implementation can lead to failure of disease control and eradication. Hepatitis vaccination serves as a telling example of this implementation gap and presents an important opportunity for learning. In patients with cirrhosis, the Centers for Disease Control and Prevention recommends hepatitis A and B vaccination, since hepatitis infection in those with liver disease is associated with increased morbidity and mortality.2 Despite this recommendation, hepatitis vaccination rates in this vulnerable population remain low.3 In this study, we chose to focus on hepatitis A for several reasons: the propensity for outbreaks among unvaccinated individuals,4 the association with other markers of social vulnerability5 and the relative simplicity of serology interpretation. While there are multiple points of contact between patients and the healthcare system which represent opportunities for improving uptake, the inpatient setting provides a unique environment where vulnerable patients have extended contact with providers and care bundles are already commonplace.6 Furthermore, few quality initiatives in the field of liver disease have focused on inpatient vaccination despite the opportunities for improvement.7 We implemented and evaluated a quality improvement (QI) initiative to increase hepatitis A vaccination rates in an inpatient population with cirrhosis.
Methods
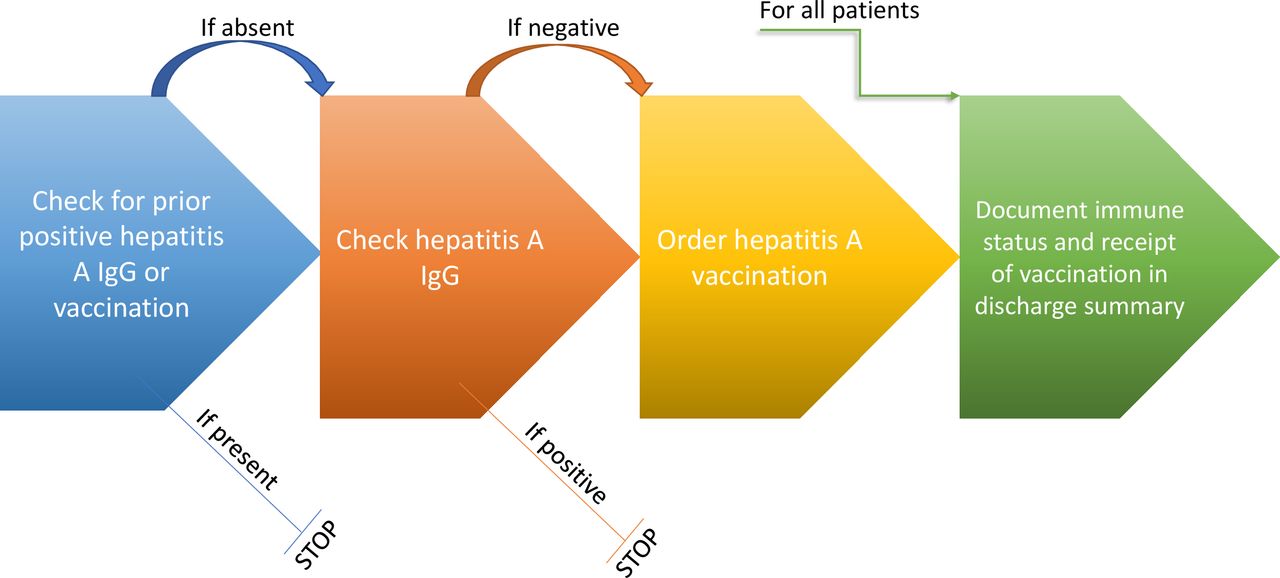
In April 2019, we implemented a two-step QI initiative targeted to the provider level at Beth Israel Deaconess Medical Center (Boston, Massachusetts). Step 1 altered note templates to include a checklist for hepatitis serologies and vaccination. These templates are commonly used by residents to write admission notes and include generic treatment plans for common diseases as a reminder to place frequently used orders. Specifically, a step was added to the generic plan for ‘cirrhosis’ which prompted the provider to review prior records for any positive hepatitis A antibodies or documentation of vaccination, order hepatitis A serologies if these were not present and order vaccination if serologies were consistent with non-immunity (figure 1). Providers were additionally instructed to include immune and vaccination status in the discharge summary. Step 2 was a brief educational session for residents promoting hepatitis vaccination in patients with cirrhosis. We identified patients with cirrhosis who were admitted to the hepatology service during a 6-month window prior to (October 2018 to March 2019, group 1) and following (May 2019 to October 2019, group 2) the intervention. The primary outcomes were serology testing, administration of the hepatitis A vaccine to non-immune patients during hospitalisation and documentation of hepatitis A immune status in the discharge paperwork. We used the Pearson χ2 test to evaluate for differences between the groups. We also collected data on demographics, cause of cirrhosis, characteristics of responsible providers, and receipt of hepatitis B, pneumococcal and influenza vaccinations, although primary outcomes were not adjusted for these variables. Patient data were captured using REDCap 10.0.19 and analysed using SAS V.9.4 (SAS Institute).

{kind=link}
Schematic of stepwise instructions prompting providers to review and evaluate hepatitis A immune status, vaccinate when applicable and document adequately.
Results
A total of 381 patients were included in the study: 187 patients in the preintervention group and 194 patients in the postintervention group. Patient characteristics by group are presented in table 1.
Select patient characteristics for patients with cirrhosis admitted to the inpatient hepatology service, by preintervention and postintervention groups
Demographics were similar between groups, as were the cause of cirrhosis, severity of illness as measured by the MELD-Na,8 utilisation of the healthcare system as measured by recent primary care visit and association with an outpatient gastroenterologist, length of stay and rates of immunity to hepatitis A in those who were tested. Although we did not detect a statistically significant difference in rates of hepatitis A serology testing between groups, non-immune patients admitted after the intervention were more likely to be vaccinated (21.7% vs 2.2%; p=0.008) during their inpatient stay (table 2).
Primary outcomes for patients with cirrhosis admitted to the inpatient hepatology service
Additionally, in the postintervention group there was a trend towards increased reporting of hepatitis A immune status in the discharge paperwork (p=0.0855).
Discussion
We implemented a QI initiative targeted at physician education and workflow with the goal of improving hepatitis A vaccination rates in hospitalised patients with cirrhosis. Several important points can be highlighted from this work. First, baseline rates of hepatitis A vaccination in the subset of eligible patients in our cohort were low. Multiple barriers likely contribute to this implementation failure, including lack of a protocolised inpatient approach, imperfect medical record-provider interfaces, delays in serology testing and competing priorities in a sick population. However, while absolute rates of vaccination preintervention and postintervention remained low, we demonstrated a 10-fold improvement in hepatitis A vaccination from the preintervention group (2.2%) to the postintervention group (21.7%; OR 12.5 (1.5, 102.3)), as well as a suggestive trend towards increased awareness by treating physicians. This is encouraging given the low-effort, easy-to-implement and generalisable nature of the intervention which signals that ongoing utilisation and even scale-up would be cost-effective. However, interpretation of these results is limited by the lack of randomisation and possibility of confounding by unmeasured factors. Additionally, significant improvement in hepatitis A vaccination rates above those measured in our study is still needed, which will require further examination of the complex barriers to vaccination and development of additional implementation strategies.9 One future direction at our institution is development of a standardised order set for patients with cirrhosis which would aggregate and serve as a reminder for common practices, including vaccination. Ultimately, dissemination and application of successful implementation strategies to other vaccine uptake gaps, including the looming example of COVID-19, is paramount to achieving efficient and comprehensive vaccination in our patient populations.
Ethics statements
Patient consent for publication
Footnotes
RJK and MH are joint first authors.
Contributors RJK and MH performed the QI intervention described herein and performed data collection. Statistical analysis was performed by RJK with ML and VP advising. All authors contributed to the writing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.