Article Text

Abstract
The East London Foundation Trust (ELFT) psychiatric liaison team (PLT) at Newham University Hospital (NUH) is responsible for referring adult patients they have reviewed, on to community mental health services on discharge where appropriate, and also to notify their existing team for follow-up on discharge when already under the care of a community service. This should then lead to appropriate ongoing management of the patient’s mental health needs in terms of continued support and assessment of risk, further assessment of mental state, titration of medications and prevention of further admissions.
Following an ELFT incident review where it was noted that a patient was not referred to community services on discharge, a retrospective case note review was undertaken over an 11-month period to define the baseline efficacy of current referrals. Quality improvement (QI) methods were used to understand the issue, create a more robust process and measure the improvements made. We set up regular QI Project meetings and we used driver diagram, process mapping, PDSA cycles and run charts. The change ideas included moving from a white board based system to using Microsoft Excel, CRS millennium patient lists, Microsoft TEAMS and additional admin support. We studied the results for the following 14 months.
The percentage of patients being appropriately referred in terms of timeliness and correct documentation increased from a run chart baseline of 35% to 88% during the project period, and the number of patients with some evidence of referral having been completed increased from 83% to 100%.
The previous system used was ineffective in managing onward referrals for mental health patients from PLT. QI methods have allowed sustainable improvement in both the percentage of patients referred and those correctly documented, improving follow up and care for mental health patients who are admitted to NUH.
- Quality Improvement
- Community Mental Health Services
- Mental Health
- Patient Handoff
- Transitions in care
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Worldwide mental health disorders make up 13% of the total burden of illness from all diseases1. Latest guidance from National Health Service England published by the Royal College of Psychiatry relating to the Community Mental Health Framework for Adults and Older Adults as part of the 5-Year Forward View for Mental Health, advises there should be a more integrated community model2 3.
Evidence shows that more integrated adult mental health models can improve patient outcomes and reduce the overall burden on mental health services.4–6 We believe good onward referral for follow-up is a key element to that integrated process.
Problem
It is very important that patients have appropriate follow-up by community mental health teams following discharge from the acute hospital. If our process of referring or notifying the relevant team is not good enough there is a risk that the mental health needs of those patients will not be met.
We became aware that not all patients were appropriately referred as per plan at the point of discharge from Newham University Hospital (NUH) via psychiatric liaison team (PLT). In addition to this, a percentage of patients may have been appropriately referred but that was not documented appropriately on the clinical record system Rio. For a percentage of patients who were already open to a community mental health team, there was no appropriate notification to the team that they were discharged from NUH or that notification was not appropriately documented on Rio.
The East London Foundation Trust (ELFT) NUH PLT is located in the borough of Newham in East London. Staff numbers include 2 Full Time Equivalent (FTE) General Adult Consultants, 0.5 FTE Older Adult Consultant, 1 FTE Specialty registrar, 0.5 FTE core trainee, 1 Foundation Year 2, 1 Foundation Year 1, 1 band eight nurse (operational lead), 8 band seven nurses, 5 band 6 nurses and three administrators (2 band 4 and 1 band five admin lead). The number of referrals across both Accident & Emergency and wards range between approximately 280 and 380 per month with up to 1700 (43%) of those patients requiring onward referral in a 12-month period.
Case note review for a period of 11 months showed that only a median of 35% of referrals were being made and documented correctly.
Our objective was to look into our outbound referral process and to achieve 30% improvement in all quantitative issues identified, whilst also aim for qualitative improvement.
Measurement
Initial data collection involved random checking of case notes of patients who had been under the care of PLT to generate 8–10 records per month that should have been referred onwards going back to November 2018. Patient records (Rio) were checked to see if there was either documentation stating the referral had been made or the referral email had been copied into the notes, in which case it was deemed to be a correctly documented referral and a baseline of 35% was established on the run chart (median).
We also measured whether there was some evidence the referral had been made, such as the community team noted the referral or had offered an appointment or had seen the patient in clinic. A baseline of 83% was established on the run chart (median) meaning that 48% of referrals were being made but not correctly documented.
This sampling continued through the project with 8–10 records being checked each month. We investigated the possibility of reviewing more records but this was impractical due to time constraints.
Design
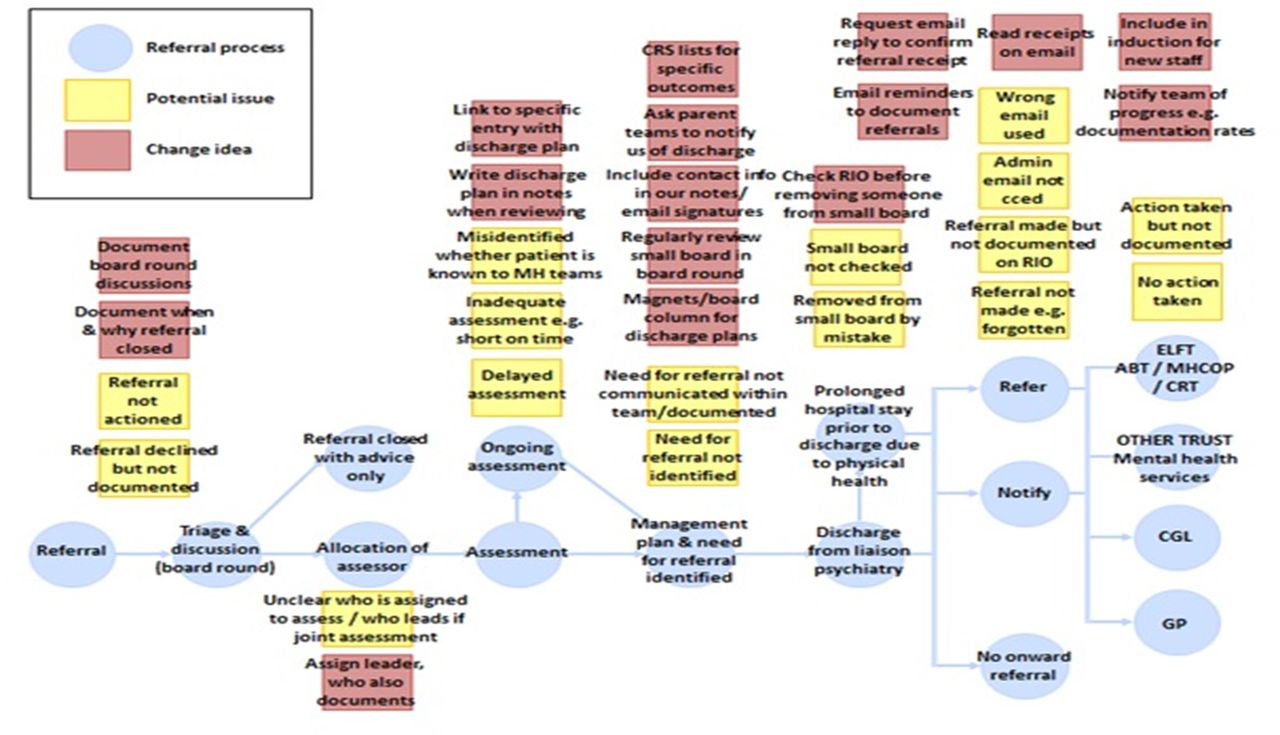
It was clear that the PLT needed to improve the percentage of referrals and documentation of referrals for patients who required continuing care in the community. A Quality Improvement Project (QIP) team was set up following invitations to a variety of members of staff from the mental health liaison team and other secondary care mental health teams. We used process mapping and driver diagram to develop a better understanding of the issue and generate change ideas (see figures 1 and 2).
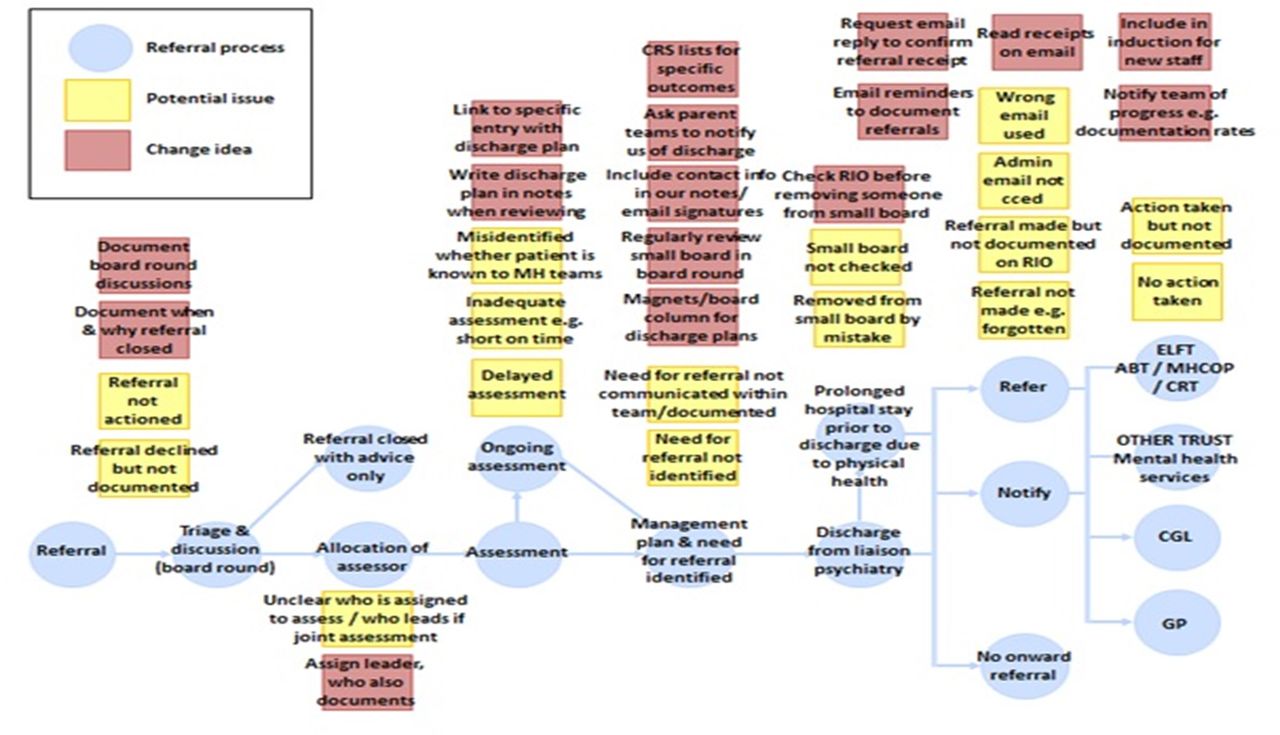
Process map. ELFT, East London Foundation Trust; ABT, Assessment and Brief Treatment Team; MHCOP, Mental Health Care of Older People; CRT, Community Recovery Team; CGL, Change Grove Live drug and alcohol service.

Driver diagram.
We used divergent thinking methods to generate change ideas. We then used convergent thinking to decide which ideas we wanted as a team to prioritise and start with. By using divergent thinking methods 17 change ideas were initially generated. They included: ensure there is clear allocation of tasks, explore creating a patient list on CRS millennium, poster reminder in the office, magnets or extra box on the white board so that onwards referral discussion starts early and the whole team is aware, ask recipient of referral for confirmation of receipt and to look at the quality of referrals.
Strategy
In our first Plan, Do, Study, Act (PDSA) cycle, which was implemented in October 2019, it was agreed that all referrals would be copied to the administration team and an email was sent to all staff advising of this new process. This was done to raise awareness within the team of the importance of making referrals and to be able to better track when referrals were being made retrospectively. We hoped the percentage of correctly documented referrals would increase.
In our second PDSA cycle, we presented data to the team as part of our business meeting in November 2019 and then 3 weeks later in December. We presented the initial case notes review results in the form of a run chart and the aim was to increase awareness among the team and encourage colleagues to join the QIP team. We hoped that our outcome measure percentages would improve.
In our third PDSA cycle, the correct content of referrals was discussed with and presented to the team by one of the consultants. An email was also circulated in early February 2020. The aim was to improve the quality of the content of the referrals. Prior to that we had also tried the change idea of collecting feedback on the quality of our referrals from recipient teams. Relevant emails were circulated, however we had no responses.
In our fourth PDSA cycle, an electronic patient list was generated on the acute trust millennium CRS system for patients currently being seen and a separate list of patients to be referred onwards. This change idea was the result of a member of our team discovering that millennium CRS has this list functionality which allows for easy visibility of patients who have been discharged from the acute trust as there is change of colour from black to grey. This change idea was introduced to the team in late February 2020. The team started using the CRS ‘currently being seen’/‘live’ list as part of the twice daily team board meeting. One of the advantages was that it was fast and easy to access or update our patient’s medical records and to move the patients from the ‘live’ list to the outbound referral list at the point of discharge from the PLT if the patient remained an inpatient at NUH at that time. Another advantage was that the patients from the CRS outbound referrals list were immediately visible as soon as they had been discharged from NUH, due to the change of colour to grey. This meant the onward referral could be done in a more timely manner. Our main white board patient list would then also be updated. We hoped the percentage of documented referrals would increase. We also hoped that for these patients who were discharged from PLT first and from NUH later, our referral would be done in a more timely manner.
In our fifth PDSA cycle the list of ‘live’ patients and those for onward referral was converted from a white board to an Excel file with three separate worksheets, one for current patients being seen/‘Live’ list, another for patients to be referred onwards/‘outbound’ list and a third to log the names of the patients with completed referrals and who had made the referral.This change idea was implemented in early March 2020. These changes were made to improve confidentiality as the white board was visible to anyone who entered the room, and avoid patients being removed from the list in error by being rubbed off. We also hoped to provide data of completed referrals and who had completed them. Soon after the Excel list was moved to Microsoft Teams. We also added a reminder on the list to check the outbound referrals once per day. We hoped the percentage of documented referrals would increase.
In our sixth PDSA cycle, we added a column to the ‘live’ list of patients being seen to flag patients for onward referral. We hoped that our outcome measures percentage would improve.
In our seventh PDSA cycle, we created handover/training documentation in July 2020 for the junior doctors to be able to pass onto the new incoming doctors. Our aim was to ensure that the improved process continued to be used with each new set of trainees when they changeover. We hoped this would make the changes sustainable.
Summary of changes
Admin to be copied on all referrals to track the process.
Present current data to team during team meeting to highlight the need to improve and raise awareness.
Presented data again at team meeting and emailed referral receiving teams about the quality of the referrals.
Implemented two patient lists on CRS Millenium system to improve visibility of patients being actively reviewed and those patients no longer being actively reviewed but who would require referral on discharge. This provided better visibility when patients were discharged and was reviewed during the two daily board meetings.
Moved from a whiteboard to a daily Excel file with three worksheets one for patients being actively reviewed, one for patients no longer being reviewed but who need onward referral once discharged and one for documenting the completed referrals. This was stored on Microsoft TEAMS.
Adaptation of the Excel spreadsheet to include a flag for patients actively being seen who will need onward referral on discharge.
Generation of training documentation to pass on to new incoming members of the team to ensure the system was sustainable.
Results
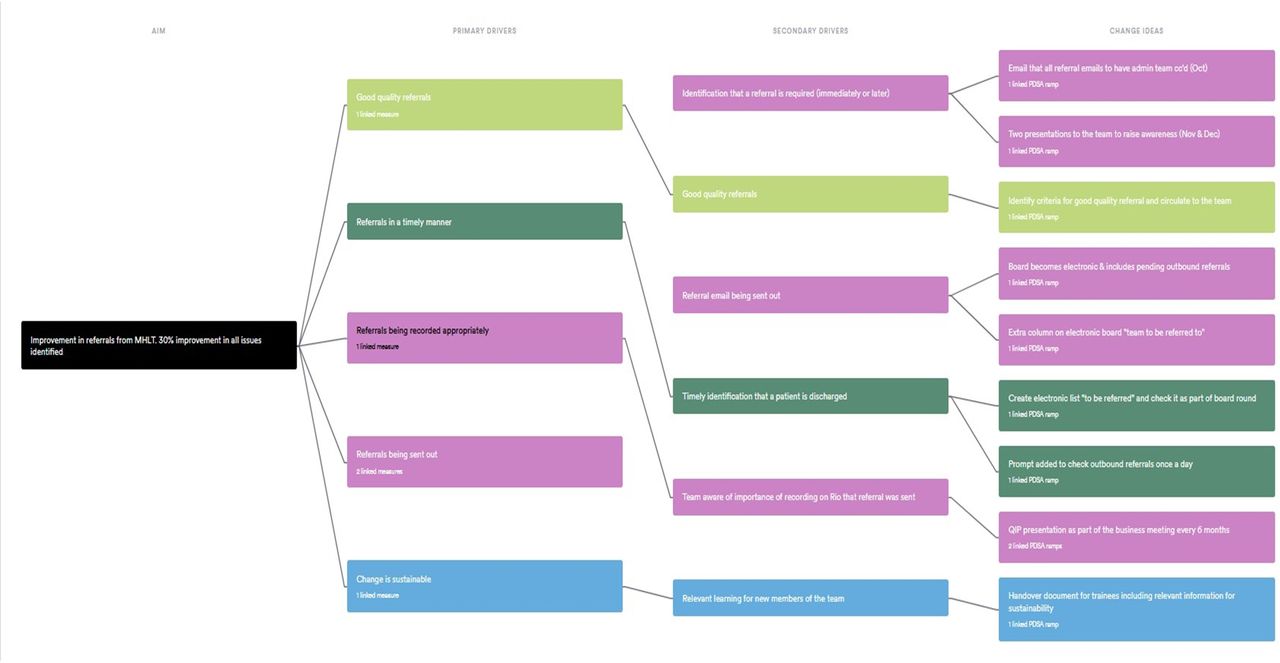
Our run charts (see figure 3A,B) indicate that for the 11 months before the first intervention the median percentage of patients with appropriate referral documented was 35%. In the 14 months following the first intervention that rose to 88%. The relevant average percentages were 38% and 86%, respectively.

{kind=link}
{kind=link}
{kind=link}
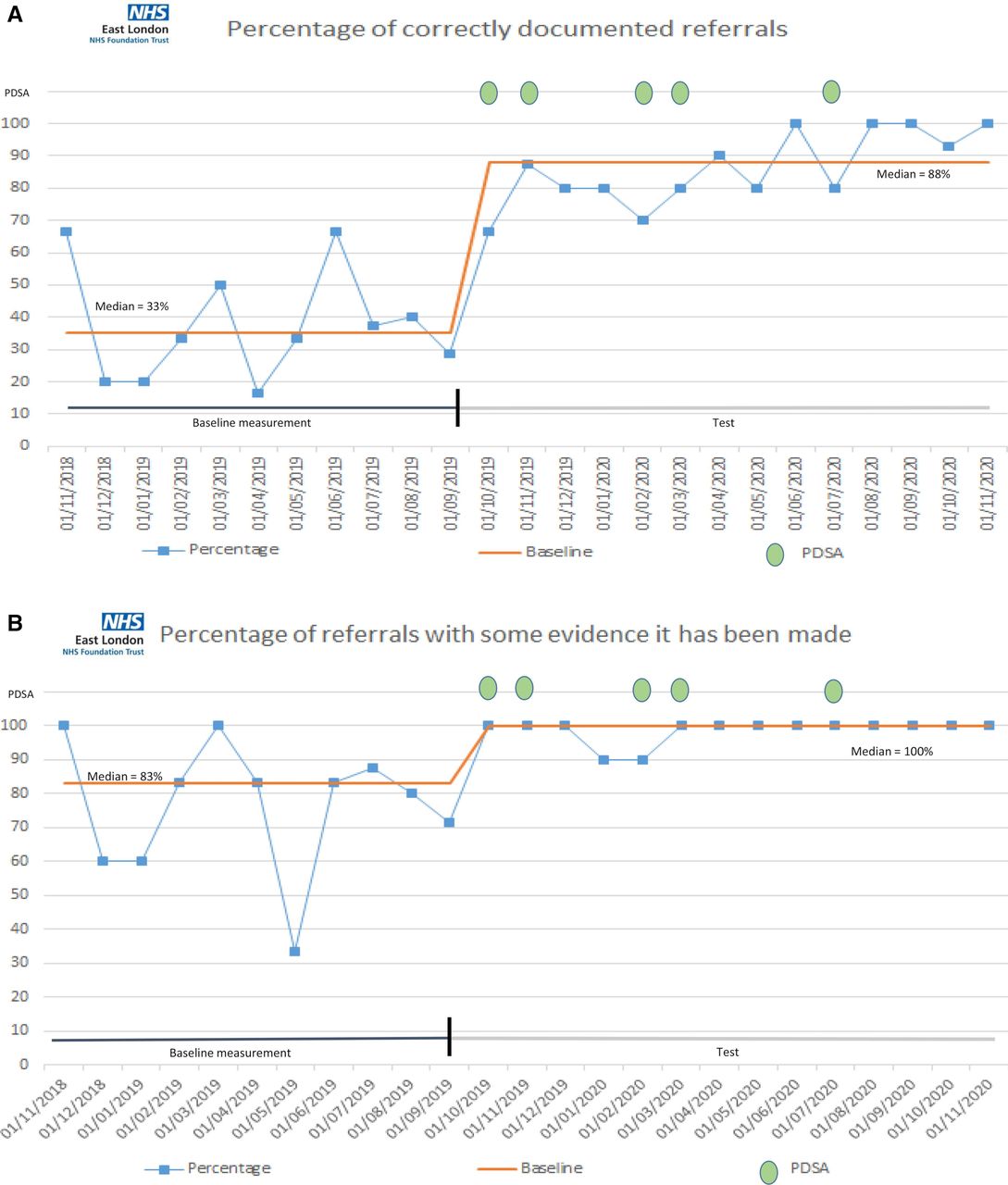
(A) Chart 1—run chart—% of patients that referral/notification was completed appropriately. (B) Chart 2—run chart—% of patients where there is some evidence that referral/notification was completed. NHS, National Health Service; PDSA, Plan, Do, Study, Act cycle.
Our run charts (see figure 3A,B) indicate that there is some evidence that referrals have been made for a median percentage of 83% for the same period. In the 14 months following the first intervention the median rose to 100%. The relevant average percentages were 77% and 99%, respectively.
In both our outcome measures run chart shift is observed (six consecutive points above the median), which is indicative of non-random variation and therefore proves that our interventions were effective. In addition to quantitative results on run charts we also sought qualitative feedback from members of staff. It was felt that the referrals were done in a timelier manner, particularly for the group of patients that was discharged from NUH at a later stage than discharged from the PLT. The acute trust millennium CRS list had played a key role in that improvement. The new process was overall significantly more effective than the previous one.
Lessons and limitations
The project aim was to improve the outbound referral process, including increasing the percentage of patients referred to community services appropriately. One of the main issues we faced was having awareness of patients that had been discharged by our team but remained as inpatients in the hospital. These patients could remain in hospital for weeks and therefore we could not complete the outbound referral at the point they were discharged from our team. The use of patient lists on the acute Trust millennium CRS system was critical for this, as it had the functionality of highlighting discharged patients with a different colour, making their identification timely and effective.
It was apparent that the white board we had for managing our lists of patients was lacking in terms of data security and robustness as names could be wiped off the board accidentally. So the move to an Excel based system where a file was saved on a daily basis, made it more difficult to lose patients from the lists, meant the data was more secure and very importantly we could add more information regarding the patient and their treatment plan. We could also audit historical data easily. We had to purchase a large screen television to use for board rounds so everyone could see the patient list which was an added cost versus the old system. Setting up the extra worksheet for completed referrals also improved the robustness of the whole system as it was clear the referral had been made by whom and when. We also included the criteria for what the referral should contain as a reminder to improve the quality of the referral.
As it was a completely new system it took a little time for all members of the team to understand how to use it, however clear instructions on the spreadsheet itself and training documents have helped embed the new process in the team and is handed over to new trainees when they rotate every 4, 6 or 12 months. Staff now feel the process is fully integrated within the team’s daily practise and feel it has improved our referrals to mental health community services.
The use of Microsoft Teams to store the handover spreadsheet on and also for holding the board meeting on via videoconference was particularly helpful as the Coronavirus pandemic hit the UK, as this allowed staff to socially distance while still being able to discuss the patients while reviewing a single list. It also allowed multiple people to access and update the spreadsheet at the same time without people having to log in and out of the spreadsheet. Using an Excel spreadsheet stored on Microsoft teams versus a white board does present a risk if there is no network or problems accessing Microsoft Teams but we feel currently the numerous benefits outweigh any risks and after using the new system for a year this has not been a problem so far.
An additional step for this improvement process could be to audit whether the referrals are being appropriately received and actioned by the service they are referred to, in order to close the loop on ensuring patients are correctly followed up in the community. However no concerns have come to our attention in this area.
Conclusion
In summary it was identified that referrals for patients being referred to community services in the liaison setting were not being sent or documented 100% of the time. This represented a flaw in the process which needed to be improved. Appropriately made and documented referrals increase the chances of correct community follow-up improving patients care and chances of recovery. Evidence shows this can reduce admission to mental health wards. We also hope it can make a positive difference in reducing the number of serious incidents relating to service users not being followed up by community services.
We used quality improvement methodology to improve a variety of aspects of outbound referrals in the liaison setting. A variety of change ideas were tested via seven PDSA cycles. We believe that our most impactful interventions included introducing more efficient use of acute trust patient electronic systems, moving to a more effective electronic patient board on Microsoft Teams, educating the team and consolidating our overall more effective process via a handover/training document. We are delighted that sustainable improvement was achieved. Given its simplistic and cheap design this model and the relevant change ideas could be rolled out to other liaison teams within our trust and other trusts in the UK.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to acknowledge and thank the whole ELFT NUH PLT for their contributions and persistence in trialling and integrating the new system into a fully working process. We particularly want to thank Dr Mazen Daher and Ulker Ali for their contribution to the project. Without their support this project would not have been possible. We would also like to thank Dr Amar Shah from the ELFT QI department for his recommendations at the stage of writing up the manuscript for publication.
Footnotes
Contributors LP led the project, including conceiving the idea, chairing the QIP meetings and providing supervision to all other members of the team. She also presented at the Newham QI forum after completion of the project and acts as the guarantor. AS, DD, APP and YE collected the data for the measures and inputted the data on run charts on QI life. AS, APP and YE delivered presentations of the QIP to the team as part of the business meeting. DD designed a poster for a conference. WHL set up the Excel file, transferred to TEAMS and generated training and process documents as part of change ideas. He also drafted the manuscript and inputted the data to create better versions of the run charts on Excel as part of preparing for submitting the manuscript for publication. All authors participated in QIP meetings and they were involved in making decisions around change ideas and implementing them. All authors discussed the results and commented on the manuscript.
Funding The cost of publication for this article was covered by East London Foundation Trust. There were no other funding considerations. Funding reference 0571246253.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.