Article Text

Abstract
The announcement of the COVID-19 pandemic in March 2020 had a huge impact on surgical practice in the UK. Many surgical trainees were redeployed to areas within the hospital to provide additional cover during this time. Providing adequate well-being and support to trainees is imperative during such times of hardship.
18 plastic surgery junior doctors were redeployed to either intensive care units, emergency departments or medical wards during the period of intervention. A 2–3 weekly quantitative survey was completed by trainees which aimed to explore rates of anxiety, depression and coping during the first peak of the pandemic. A ‘COVID-19 Care Package’ was provided and regular interactions with the parent team was encouraged via the online platform of Zoom to support surgical junior doctors.
The average anxiety score for trainees exceeded that regarded as ‘normal’ as predicted by the Hospital Anxiety and Depression Scale. Core surgical-level trainees were found to show higher scores of anxiety and depression throughout the course of project as compared with their senior specialty registrar counterparts. 43.8% of junior doctors reported greater levels of stress since the announcement of the pandemic. 81% of junior doctors stated they would value regular check-ins with work colleagues during difficult times.
Providing a strong support system for trainees is vital to ensure doctors are not overwhelmed during potentially volatile times in their careers. The use of psychological monitoring tools to guide the implementation of appropriate levels of support for individuals could aid in enhanced junior doctor well-being and support. Feedback from surveys during this time of study suggests that surgical trainees agree that contact with their parent team and colleagues has a positive impact on their well-being and trainees value regular ‘check-ins’ with their colleagues on a monthly basis.
- COVID-19
- Mental health
- Medical education
- Surgery
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The WHO declared the COVID-19 outbreak as pandemic status on 11 March 2020 following the rapid global spread of cases, originating from Wuhan, Hubei Provence, China. At this point in time there were over 17 000 cases reported in Europe, with trends mirroring that of the initial peak in China in mid-January 2020.1
The risk of healthcare capacities being exceeded for the National Health Service (NHS) was considered an inevitable event, causing uncertainty and anxiety among healthcare workers across Britain. Particular concerns pertained to perceived own personal health, the well-being of family and loved ones, the stresses of increasing workloads, delays and changes to training and overall perceived emotional hardships.2 Junior-level doctors were deemed a vulnerable group and comprised the majority of the cohort that were redeployed to areas such as the emergency department (ED), intensive care units (ICU) and medical wards to lend a helping hand during peak times of the pandemic. Providing a strong support network for the junior doctor cohort in aims to reduce psychological burden and adverse mental health outcomes is imperative during such unprecedented times.
Background
Literature reveals that during major disease outbreaks, healthcare workers in EDs, ICUs and isolation wards are at a greater risk of developing adverse psychiatric outcomes as compared with those working in other departments.3
This is theorised to result from direct exposure to infected patients and the workload itself being highly demanding.4 A systematic review revealed risk factors for healthcare workers in developing psychological comorbidites during the course of the SARS outbreak included lack of social support, maladaptive coping strategies and insufficient training.5 Moreover, a cross-sectional analysis in China following the announcement of the epidemic revealed that young people and healthcare workers were at the highest risk for experiencing mental health illness, namely generalised anxiety disorder, depression and poor sleep quality.6 It was additionally found that women and those healthcare workers with relatives of confirmed or suspected infection with COVID-19 were more susceptible to anxiety and depression.6 Moreover, healthcare staff in a Beijing hospital working in high-risk COVID-19 clinical areas had been found to show increased rates of post-traumatic disorder symptoms.7
The utilisation of online mental health education sites, counselling and telephone services have been widely encouraged since the initial outbreak in China8 to provide a source of well-being to workers at ensuing stressful times.
The emerging adverse mental health effects experienced by health workers around the world during the COVID-19 pandemic highlight the fact that it is imperative to promote well-being and provide adequate support for all healthcare staff amidst this unprecedented time.9 Promoting strong teamwork ethics and maintaining cohesiveness between colleagues serves to build a robust support network and allows team members to share similar experiences during difficult periods of time.10 Timely contact with senior supervisors provides additional modalities of support for junior doctors, particularly with regard to anxieties about limited training opportunities and potential hindrances in career progression during this time. This is particularly true of surgical trainees where cancellations of many elective operating lists, clinics and reduced exposure to a variety of surgical pathologies as a direct result of the pandemic threatens a lower standard of training for aspiring surgeons. The scope to explore these premises further with psychological monitoring tools in the surgical environment could serve as a guide to provide trainees with appropriate well-being and support resources during challenging times.
Measurement
Eighteen surgical trainees within a Burns and Plastic Surgery department in Manchester, UK, were included in the project; this comprised 9 specialty registrars and 9 core surgical-level trainees. Core surgical-level trainees had recently embarked on their surgical training careers (previously known as senior house officers) and therefore were less experienced in the field of plastic surgery as compared their specialty registrar counterparts. Specialty registrars had completed their core competency surgical training and were on the plastic surgery specialty training programme. The majority of trainees were redeployed to ICU, ED or medical wards. The intervention period coincided with changes to standard working schedules for doctors within the plastic surgery department due to the COVID-19 pandemic.
Data were collected between April and July 2020. Trainees completed an online quantitative survey at approximately 2–3 weekly intervals. A 14-point psychometric scale aimed at measuring symptoms of anxiety and depression, the Hospital Anxiety and Depression Scale (HADS)11 was completed by each trainee. This was completed a total of 4 times by trainees during the course of the project. The HADS comprised seven items to screen for anxiety symptoms and seven items to screen for symptoms of depression, taking an average time of 2–5 minutes to complete. A total score of 0–7 was regarded as ‘normal’, 8–10 as ‘borderline abnormal’ and 11–21 as ‘abnormal’, this was calculated for each individual, every time the survey was completed. The HADS tool has been recommended by the National Institute for Health and Care Excellence for diagnosing anxiety and depression.12
Participants completed surveys anonymously and chose not to reveal their age or gender due to the small sample size of participants and this was respected by the project leads.
The use of the HADS in this quality improvement intervention was based on the premise that anxiety and depression often coexist, and that anxiety often precedes depression in response to a stressor. This has allowed occupational health professionals to predict outcomes in order to plan interventions for vulnerable employees and prevent mental health morbidities.13 The HADS has been validated in many countries and languages, and has been used widely for initial diagnoses of anxiety and depression as well as monitoring the progression of these disorders over time.12 14 This is an essential consideration for tutors and/or educational supervisors in attempts to provide a robust support network for their trainees and a standardised modality in monitoring rates of mental health in trainees during difficult times.
Design
During the period of the intervention, both a core surgical trainee-level doctor and consultant were assigned as ‘well-being officers’ for the group and stood as the first point of contact for trainees to reach out to. Well-being officers maintained regular contact with all trainees and ensured surveys were disseminated and completed within the specified time periods. A personal departmental psychologist maintained regular contact with the consultant throughout the course of the project and advised on well-being resources and offered individual support for trainees, if required.
A ‘COVID-19 Care Package’ was provided for all trainees (found in online supplemental materials section). This included resources aimed at promoting good mental health for trainees (see table 1). The care package encouraged regular contact with the parent team via weekly ‘zoom check-ins’, a doctors Whatsapp group maintaining contact with peers, optional one-to-one sessions with an assigned consultant supervisor, a 24-hour anonymous employee well-being helpline as well as various online mental health resources. All trainees received an adequate induction regarding teaching and training in their new job roles prior to the start date of the redeployment period.
Supplemental material
'COVID-19 Care Package’ contents
These interventions were based on literature reviews outlining that a lack of peer support predicts higher rates of anxiety, depression and burn-out15 16 and that predominant risk factors for developing psychological comorbidites during these times include lack of social support, maladaptive coping strategies and insufficient training5 in job roles.
Prior to this quality improvement project, there were no formal pathways sign-posted for trainees in difficult times; it was expected that trainees would consult with their assigned educational supervisor if they required additional support during times of work-related stress or personal hardship.
Strategy
Plan-Do-Study-Act (PDSA) cycle 1
Interventions aimed to increase mental health well-being and provide junior doctors with adequate coping resources over the period of redeployment due to the COVID-19 pandemic. Participants were recruited for the quality improvement project and an online survey was created and disseminated to participants. The aims were to measure rates of anxiety and depression in participants and to promote utilisation of resources in the ‘COVID-19 Care Package’ to promote good mental health during this period of time.
PDSA cycle 2
Result analysis found that the average anxiety score across trainees was high. Feedback found that participants were not filling in all aspects of the survey. Zoom meetings were held and participants were encouraged to engage with the intervention in all aspects and to use the resources provided to promote adequate coping strategies and promote good mental health. Well-being officers checked in regularly with all participants during working hours and raised awareness of weekly zoom meetings.
PDSA cycle 3
It was hypothesised that raising awareness and benefits of weekly ‘check-ins’ with the parent team would encourage more participants to engage with the process and contents of the ‘COVID-19 Care Package’. These resources were disseminated within the workplace by well-being officers and this was reflected by an increasing number of participants attending weekly zoom support meetings. Feedback from participants highlighted that they valued these sessions and that it relieved their stress levels. It was clear that anxiety levels remained high as an average, therefore participants were encouraged to use resources such one-on-one support sessions with the consultant supervisor as well as the 24-hour employee helpline with a view to arranging structured counselling service on an individual basis.
PDSA cycle 4
Results analysis showed that all aspects of the ‘COVID-19 Care Package’ were being used more frequently by participants. Individual feedback suggested that although weekly meetings were very valuable, these may be more well received on a monthly basis and that this should be incorporated on a long-term basis for all trainees, and not just during times of hardship, due to the positive mental health impact it had on trainees.
Results
The survey, which included the HADS, was completed by each plastic surgery trainee a total of 4 times during the period of intervention.
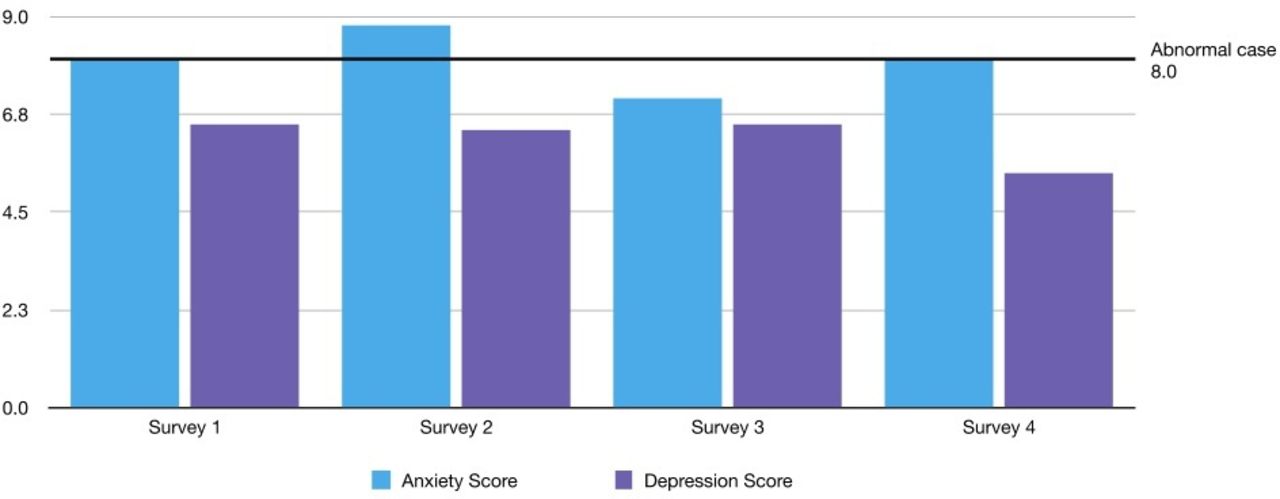
Scores higher than 8.0 were defined by the HADS as ‘cases’, indicating a ‘borderline abnormal case’ (please see online supplemental file 2).
Supplemental material
The average anxiety scores for plastic surgery trainees were 8.0, 8.8, 7.1 and 8.1 and depression scores were 6.5, 6.4, 6.5 and 5.4. Therefore, the trend of ‘anxiety scores’ with each successive survey completed showed high initial scores, which reduced over a period of 6 weeks. These scores then increased once more towards the end of the project. Trends for ‘depression scores’ were persistently below the diagnostic threshold throughout the project period, with average scores for trainees remaining similar and then decreasing towards the end of the intervention period. These results are shown in figure 1.

Comparing average anxiety and depression scores between plastic surgery trainees throughout project period.
Core surgical-level trainees were found to show higher scores for depression and anxiety throughout the course of the quality improvement project as compared with their registrar counterparts (average scores of 8.5 and 7.6 for core surgical-level trainees; average scores of 6.2 and 5.3 for registrars, for anxiety and depression, respectively).
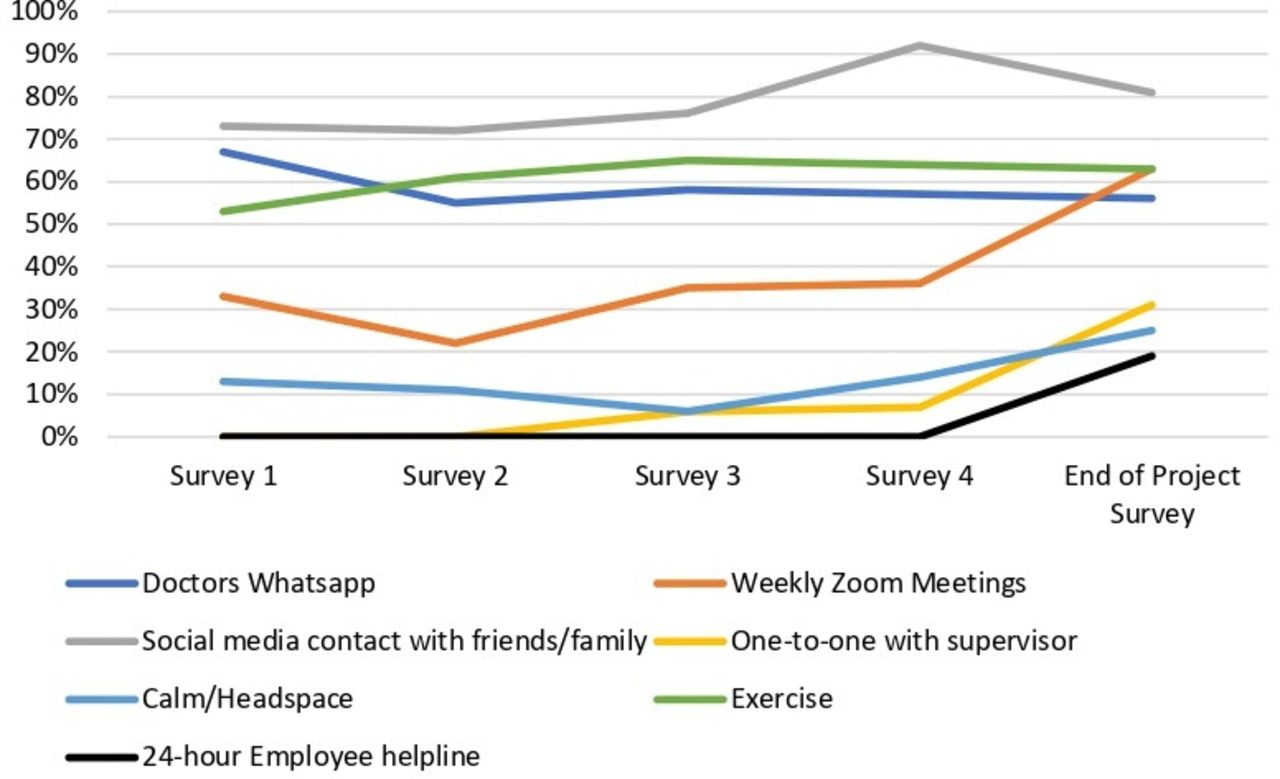
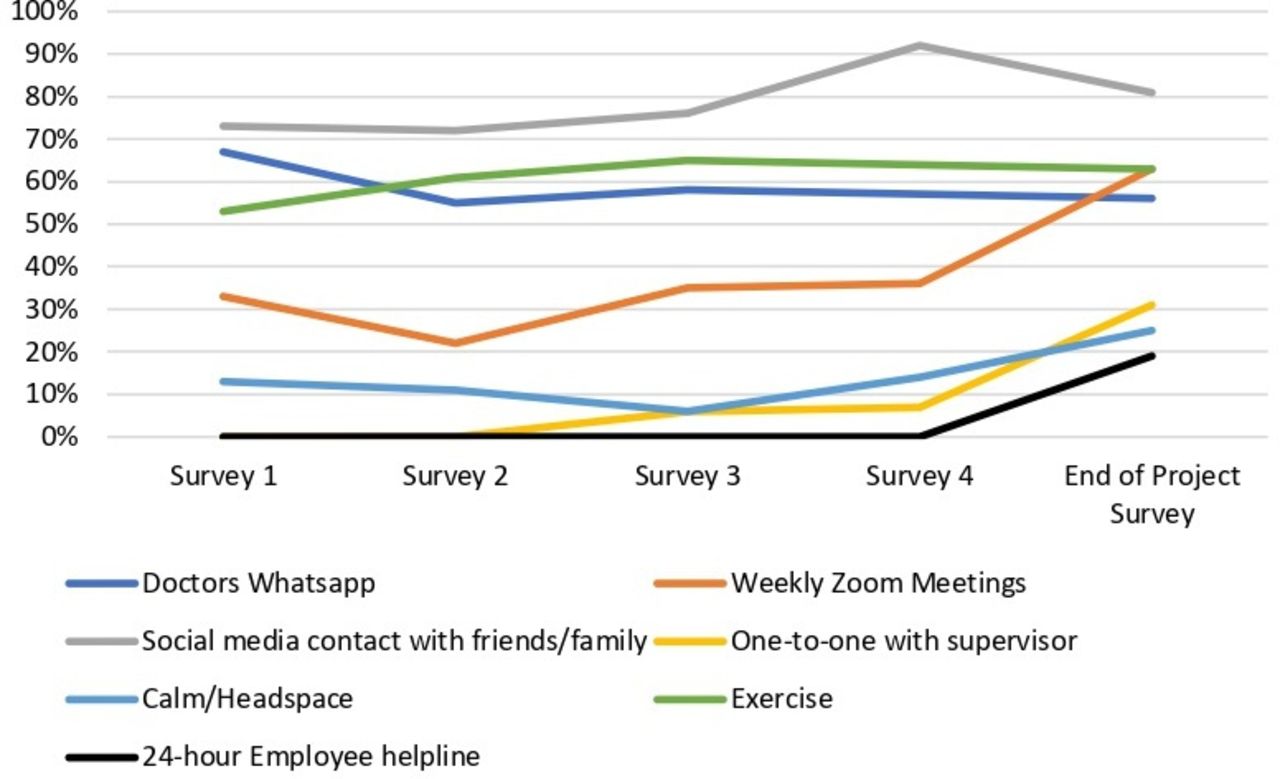
All trainees utilised the ‘COVID-19 Care Package’ resources, with the majority turning to online platforms to stay in touch with family and friends, regular exercise and tuning into weekly zoom meetings with their colleagues. The use of most resources within the ‘COVID-19 Care Package’ increased throughout the project, as can be evidenced by figure 2. Towards the end of the project, a smaller proportion of trainees used the one-to-one supervisor sessions with an assigned consultant and the 24-hour employee and well-being confidential helpline.
{kind=link}
{kind=link}
Trainees use of resources provided by ‘COVID Care Package’ throughout project period.
43.8% of doctors stated they had subjectively experienced greater amounts of stress at work or within their personal life since the announcement of the COVID-19 pandemic.
62.5% of trainees believed they were well supported by their parent teams during this time of hardship. 81% of respondents stated they believe it is important to have regular check-ins with work colleagues during difficult times, with 81.2% suggesting these should be held on a 1-monthly basis.
Lessons and limitations
This quality improvement project shows that the average anxiety scores in junior surgical doctors exceeded that as regarded as ‘normal’ as predicted by the HADS. This can be assumed to be due to the burden of the COVID-19 pandemic, however, it is difficult to draw causative inferences due to multiple confounding factors and a small participant sample size. Due to the sensitive nature of the project as well as the high turn around of doctors rotating to new jobs, additional data could not be collected after participants had left the department. Furthermore, it was decided by well-being officers before the commencement of the quality improvement project not to record the age and gender of participants; this was requested by participants prior to data collection and was respected by the project leads. This was a recognised limitation in this intervention and it would be suggested by the authors that similar studies conducted on a larger scale could further explore differences in mental well-being in doctors with consideration to their age, gender as well as other demographics.
Conclusion
Providing a strong support system for trainees is imperative in ensuring that our doctors are not overwhelmed as a result of this volatile time in their careers. This can adversely affect the ability of doctors to provide optimal patient care and directly lead to sickness and absences within the workplace. Analyses showed junior surgical colleagues were more likely to become overwhelmed, overworked and experience higher rates of anxiety and depression as compared with their senior colleagues. It is clear from the findings in this small observational project that junior trainees may be more adversely affected by new and unfamiliar challenges in the workplace. This could be due to less working experience overall and possibly limited confidence, however, this provides scope for similar studies to be conducted on a larger scale in order to make more robust inferences on these matters.
A ‘COVID-19 Care Package’ was well received by all trainees in this project. Feedback suggests that surgical trainees value well-being support efforts with monthly check-ins with their peers via the platform of ‘zoom’. Participants stated that the implementation of the ‘COVID-19 Care Package’ encouraged cohesiveness within the group, facilitated the formation of meaningful relationships with their colleagues and seniors alike, and these measures reduced subjective stress levels during this period of hardship. These outcomes were highlighted specifically by doctors recently moving to the United Kingdom from overseas with no direct support from friends and family members.
The authors of this communication believe it is prudent that this cohort of doctors are followed up in terms of residual symptoms of stress, anxiety and depression. The implementation of further national lockdowns since the completion of the project should dictate the requirement for regular monitoring for symptoms of these disorders.
The continued use of an appropriate psychometric scale to measure rates of anxiety and depression following such events can furthermore be utilised by departmental leads to plan mental health resources for their employees; this can be replicated and applied nationally within the NHS. Although beyond the scope of this work, it is suggested that participants ought to be screened for symptoms of post-traumatic stress disorder (PTSD); this has been highlighted by recent studies in China showing an increased incidence of PTSD among healthcare staff working on the frontline during the early phases of the pandemic.17 18
Surgical trainees seek a structured well-being support system which should be incorporated for all junior doctors to promote well-being and support throughout the surgical training curriculum, not only during periods of hardship. As a recognised highly demanding vocation, junior doctors should have access to appropriate mental health facilities. Perhaps resources to promote well-being in trainees and regular contact with the parent team should be incorporated into induction programmes for all junior doctors within the NHS.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Formal ethical approval was not sought for this study as there is no identifiable participant data collected as part of this quality improvement project. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to acknowledge the Burns and Plastic Surgery department at Wythenshawe Hospital for the support and cooperation provided during the period of intervention.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SA was the primary author and guarantor for this quality improvement project, with the support of senior Burns and Plastic Surgery consultant SM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.