Article Text

Abstract
Variable rate intravenous insulin infusions (VRIII) are frequently used in hospitals and incorrect use can lead to electrolyte imbalance, hypoglycaemia and adverse outcomes. The Joint British Diabetes Societies (JDBS) published guidelines in 2014 and recommended the use of a balanced fluid as substrate. There was no published data to demonstrate the superiority of this fluid in reducing adverse events. This quality improvement project aimed to review the existing practice at our Trust in accordance with JDBS guidelines. We predicted introducing this fluid would reduce adverse events and demonstrating this was a prerequisite condition from our Trust Medicines Management Committee to approve its long-term availability. We carried out an audit of our practice in 2015, at which time the JBDS recommended fluid (0.45% sodium chloride/5% dextrose with 0.15% potassium chloride) was not available in our Trust. Our VRIII guideline was re-written with recommendation for use of the balanced fluid, after procurement from pharmacy. Our primary areas for improvement as highlighted from the 2015 audit were correct substrate prescription and rate reduction of hypokalaemia (potassium <3.5 mmol/L) and hypoglycaemia (glucose <4 mmol/L) during VRIII use. Analysis of the pre-intervention (December 2016) and post-intervention (September–November 2017) data showed a significant increase in correct fluid use; 11% pre-intervention to 76% post-intervention (χ2, p<0.0001). The number of hypoglycaemic events per VRIII reduced from 0.73 (±1.78) to 0.28 (±0.84) (p<0.05) peri-intervention. Similarly, the number of hypokalaemic events per VRIII reduced from 0.15 (±0.54) pre-intervention to 0.05 (±0.25) post-intervention. There was also a significant reduction in number of VRIII episodes associated with a hyponatraemia event from 26% at baseline to 12% post-intervention (p<0.01). Some of these marked improvements were not sustained at 1-year post follow-up. We reduced adverse outcomes with a substantial net-cost saving during this period, through implementation of new and accessible guidelines, trust-wide education programmes and posters to raise awareness.
- diabetes mellitus
- quality improvement
- cost-effectiveness
- adverse events, epidemiology and detection
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The use of variable rate intravenous insulin infusions (VRIII) is common during inpatient care, usually to achieve normoglycaemia.1 2 They are frequently associated with adverse events and complications if not managed properly. At this tertiary centre with >1200 beds, VRIII are used more frequently than most hospitals. This is due to the higher prevalence of inpatients with diabetes (22.1% vs 17.2% nationally)1 and the complexity of the patients it treats, such as complex cardiac, renal and liver patients and transplant patients. The use of VRIII in 2016 among inpatients at this centre was 16.8% vs 8.2% nationally.1
The Joint British Diabetes Societies (JBDS) published guidelines on the use of VRIII in medical and surgical inpatients,2 aiming to standardise practice across the National Health Service (NHS) and reduce the risk of adverse events. Key points of recommendation were the use of 0.45% sodium chloride/5% dextrose with 0.15% or 0.3% potassium chloride, addition of potassium to the fluid if serum potassium level of <5.5 mmol/L, ensuring basal insulin was continued and oral hypoglycaemics stopped where applicable prior to starting the VRIII and safe monitoring with daily urea and electrolyte monitoring and 1–2 hourly blood glucose measurements.2
A local audit undertaken at our centre in 2015 was prompted when a junior doctor noticed the fluid advised as a substrate alongside insulin in our VRIII guideline (0.45% sodium chloride/5% dextrose with 0.15% or 0.3% potassium chloride) was neither available nor being used on the ward. The audit showed we were not working in accordance with these guidelines, identifying cases of hypokalaemia associated with inappropriate fluid administration alongside intravenous insulin.3 Sixty-four per cent of the VRIII identified did not have recommended supplementary potassium as part of fluid substrate resulting in a significant reduction in potassium levels and new-onset hypokalaemia. This instigated the procurement of the expensive JBDS recommended new fluid to achieve reduction in adverse events and improve patient safety and re-writing of our guidelines. We therefore planned a quality improvement project (QIP) with the following aims:
Aim #1: to ensure correct fluid use alongside VRIII, aiming for >80% of episodes of VRIII to be on the JDBS recommended fluid.
Aim #2: to reduce the rate of hypokalaemia (serum potassium <3.5 mmol/L) to <5% of VRIII episodes.
Aim #3: to reduce the rate of hypoglycaemia (capillary or venous blood glucose <4 mmol/L) to <20% of VRIII.
We aimed to do this by the end of the intervention period (2017, 1 year) and hoped to sustain this at follow-up 1 year later (2018).
Background
Diabetes represents one of the most common medical comorbidities in hospital patients, affecting up to 17% of inpatients in the UK NHS, according to recent nationwide data.1 Controlling glucose levels in acutely ill patients with diabetes can be challenging, and recourse to VRIII is inevitable in certain clinical settings, both on medical and surgical wards. VRIII requires close monitoring and can be associated with serious adverse events if not managed properly, including hypoglycaemias, electrolyte disorders and fluid overload.2–4
While there is limited research on the frequency of adverse events associated with VRIII, the evidence that is available shows high rates of adverse events.2 5–7 A local audit undertaken at our centre in 2015 showed a significant fall in potassium levels and high rate of hypokalaemia associated with inappropriate fluid administration alongside intravenous insulin.3 The National Diabetes Audit (NaDIA) in 2015 showed a national average of hypoglycaemia in 20% of VRIII episodes,7 while the 2011 NaDIA found that 3.3% of patients had hypoglycaemia (<4 mmol/L) >25% of the time while on VRIII.6 Bhadresha et al. found 30% of VRIII episodes were associated with hyponatraemia when glucose 5% was used as a substrate.5 As well as this, monitoring of glucose measurements while on a VRIII, which is paramount for their safe usage, is often poor, as shown in the 2011 NaDIA with 6.4% of patients on a VRIII having <4 glucose measurements in the preceding 24 hours.6
VRIII can be hugely costly to the NHS, both in terms of treatment and increase in length of stay.8–11 Although the proportion of inpatients with diabetes treated with VRIII has been declining slowly over recent years, little progress has been achieved in avoiding mismanagement during its actual use.
Measurement
During our baseline period of 10 weeks between September and December 2016, we identified 135 separate episodes of VRIII prescribed for medical and surgical patients at the Queen Elizabeth Hospital Birmingham (QEHB), corresponding to 114 patients, using the hospital’s electronic prescribing and clinical records system (Patient Information Communication System (PICS)). We excluded VRIII administrations that lasted less than <4 hours, those that occurred in an intensive care setting, those where patients were on total parenteral nutrition (TPN) or nasogastric (NG) feed as their fluid substrate, and any dataset that was not complete. Each episode was considered separate if the infusion had been stopped for >4 hours.
We collected data on demographics, duration of VRIII, fluid substrate usage and whether potassium was added to this, monitoring of biochemistry (urea and electrolytes, glucose measurements), adverse events (hypoglycaemia <4 mmol/L, hypokalaemia (<3.5 mmol/L), hyponatraemia (<135 mmol/L)) and compliance with best practice for diabetic medications during VRIII (continuing long-acting insulins, stopping all other insulins, stopping oral antidiabetic medications). We reviewed adverse events in two ways: the number of VRIII episodes with at least one adverse event, and the average number of adverse events per episode. This was because of the wide range of duration of VRIII and therefore likelihood of having more adverse events. If electrolytes were not checked while on the VRIII, the episode was not included in the results.
Within the QEHB, intravenous insulin algorithms and substrate fluids are prescribed separately on PICS. The fluid prescription is not automatically added to the insulin prescription as VRIII are used in many departments throughout the Trust including intensive care, cardiology and renal departments, where the substrate use may vary according to concern with fluid balance and alternative forms of substrate may be used such as continuous NG feed or TPN. The prescriber has to select their own fluid type and rate. During this QIP, the protocol was made accessible via the prescription page through an electronic link where the fluid and electrolyte recommendations could be found. Nursing staff administer fluids, check blood glucose and adjust insulin doses according to electronic prescription and record electronically the changes in the hourly rate of intravenous insulin. The point of care blood glucose levels are automatically uploaded to PICS.
The initial baseline characteristics are highlighted in table 1. Of 135 VRIII episodes, only 15 (11.1%) had the correct fluid used alongside the VRIII and only 49 (36%) had potassium added to the fluid. Ten (7.4%) had no fluid substrate at all. Electrolyte disturbance was common with hyponatraemia occurring at least once in 35 VRIII episodes (26%) and at least one hypokalaemic event occurring in 11 VRIII episodes (8.2%). Hypoglycaemia rates were also high, occurring at least once in 34 episodes (25%). The rates of hyponatraemia, hypokalaemia and hypoglycaemia were 0.36, 0.15 and 0.73 per VRIII, respectively. Daily urea and electrolytes were checked in only 59%. Diabetic medication management was also suboptimal with only 48/70 patients on long-acting insulins prior admission continuing appropriately while on VRIII (68.5%) (figure 2).
Characteristics of VRIII episodes and patients
To meet our project aims of adhering to JDBS guidelines to reduce adverse events and improve the safety of VRIII usage, we implemented various interventions using the Plan-Do-Study-Act (PDSA) quality improvement (QI) tool, then re-collected the same data points using the same methods as the baseline collection.
Design
The QIP team consisted of multiple members of the diabetes team; diabetes consultants, junior doctors, several of whom had major roles throughout the project and diabetic nurse specialists. Additional project members who helped with the implementation of our interventions were the pharmacy, IT and graphics team. The PICS team were instrumental in allowing the collection of data throughout the project. Members of the team met regularly (monthly) to discuss progress. Patients and the public were not involved in the design, conduct, reporting or dissemination plans of our research.
We appreciated that by introducing the JBDS recommended fluid which was not available at our Trust in 2015 at the time of our baseline audit, this would require an update of our existing guideline, raising awareness of the new guideline to prescribers and investing in the new fluid with agreement from Trust Medicines Management Committee. We also assumed that linking the new guideline electronically to the prescriber at the point of prescription on PICS would result in increased prescriptions of recommended fluid once they were readily available in the clinical areas. Therefore, our assumption was that the primary drivers for improvement would be: (1) education to improve awareness, (2) guideline renewal and accessibility as system change, (3) resources to invest in new fluid which we assumed to improve our primary outcomes.
As this was a new fluid, the introduction was piloted in certain wards of the hospital before being rolled out widely. We did not insert alerts in PICS for prescribers as there are several in the system and our PICS committee actively discourage use of alerts if alternative safe options are available because of alert fatigue of prescribers.
To ensure sustainability after the initial year, the new VRIII guideline was included in staff induction training, as a visual aid in the form of a permanent posters on the wards and on the Trust Education portal as online resources available to access at any time.
Strategy
The interventions that were orchestrated at various stages of the QIP are illustrated in figure 1. The PDSA cycles and specific interventions were planned in advance but challenges arose if they were not able to be implemented in time. Each cycle lasted between the starting point of each data collection, for example, time between the diamonds as shown in figure 1.
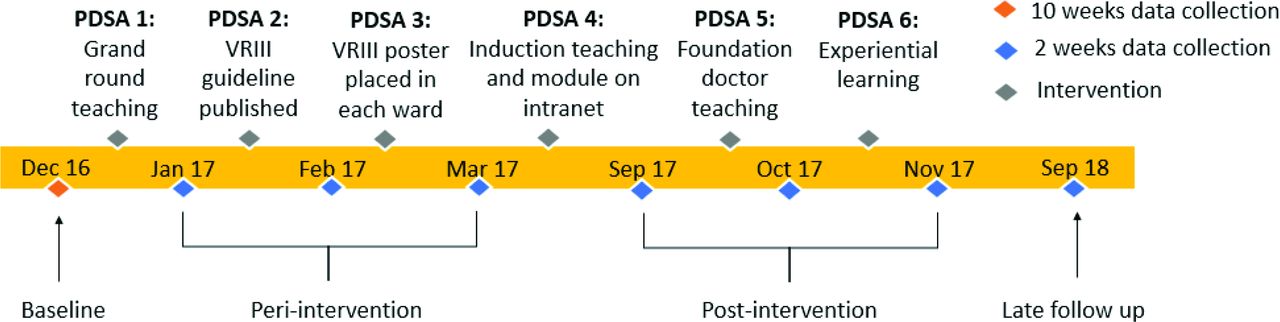
Timeline of interventions implemented (Plan-Do-Study-Act (PDSA) cycles). VRIII, variable rate intravenous insulin infusions.
PDSA cycle 1: 4 weeks
The aim was to widely disseminate the results from our baseline analysis at our medical Grand Round meeting in mid-December 2016 to educate healthcare professionals on the problems we had highlighted. We mapped out our improvement plan and informed of the release of the new VRIII guideline. The guideline could not be disseminated at this stage as pharmacy had not gone ahead with procurement of the fluids pending approval from Medicines Management Committee, who sat in January 2017. This was a challenge, as the message may have been stronger with the combination of information. It did however allow us to create the next PDSA cycle. We recollected data 3 weeks after the presentation with analysis of VRIII use in the first 2 weeks of January 2017. Presentation in the Grand Round was repeated in PDSA cycle 4 given its effectiveness in this cycle in delivering information to a wide cohort.
PDSA cycle 2: 4 weeks
The new VRIII management protocol was launched at the QEHB in late January 2017, reflecting the clinical practice recommended by JBDS.2 Our guideline and electronic prescription image can be accessed from QIC_QEHB_2018_VRIII_supporting_materials.docx. The aim was to provide up-to-date and user-friendly guidance that was accessible at the point of prescription. It was also made freely available on the Trust’s Intranet. The baseline data had shown that despite the JDBS recommended fluid being part of the old guideline, it was not being prescribed. Therefore, we predicted a release of new guidelines along with heavy advertisement would help to ensure correct prescription and adherence to other guidance. The challenge was therefore attempting to change behaviour with a document that needed to be detailed enough to cover a wide range of clinical scenarios, while remaining succinct enough to allow reduction in adverse events.
PDSA cycle 3: 4 weeks
Quick-reference poster guides were designed reflecting the VRIII guidelines in a simple but effective manner and were disseminated throughout the hospital in February 2017, available on every ward and patient area using VRIII. The aim was to reinforce and sustain good practice. The ease of use would make healthcare professionals more likely to follow them. We looked at previous posters that had had success and used the hospital Diabetes Steering Group for review prior to a formal hospital launch of the poster. There were logistical dilemmas in ensuring the posters were displayed in every clinical area in order to maximise effectiveness.
PDSA cycle 4: 6 months
The aim of this cycle was to continue reinforcement in existing medical staff and inform newcomers with education surrounding the new guidelines given the usual change-over of medical personnel within this period. A freely available online teaching module was designed in March 2017. The analysis of results after the third PDSA cycle were presented at the medical Grand Round in May 2017, including the now released new trust VRIII guidelines and quick-reference poster guide. Induction teaching sessions were delivered by Diabetes team members to new healthcare professionals to the hospital in August 2017. The challenge was instilling knowledge of the hospital guidelines to healthcare professionals who may have had differing guidance elsewhere to try and prevent bad habits and encourage those to subconsciously teach others when they came to use the VRIII.
PDSA cycle 5: 1 month
Teaching sessions were delivered to the foundation doctors new to the trust as part of their foundation teaching lecture series (September–October 2017). The aim was to specifically focus on education in the set of doctors that most frequently prescribe VRIIIs. We predicted that teaching this group specifically would have a good effect on adherence to guidelines, namely the prescription of correct fluids and diabetes medication management. We used the induction teaching sessions that had been delivered in PDSA cycle 4 as a basis for the foundation teaching sessions, with adaptations to aim at foundation doctors, namely prescribing and medication management.
PDSA cycle 6: 1 month
The aim of this cycle was to measure the effect of experiential learning and the continued reinforcement of prior interventions in the form of the available new trust VRIII guidelines, accessible poster reference guides and internet modules. Further teaching sessions were also arranged periodically (every 2–3 months) throughout 2017. We predicted that the combination of the above would further improve adherence leading to reduced adverse events. The challenge was the length of time between the final cycles, and we would therefore need a further post-intervention data analysis to truly assess sustainability.
We collected further data 1 year after the final data collection to see if our improvements in practice and associated reduction in adverse events had been sustained. Data were collected continuously throughout the process, with each data collection period spanning 2 weeks, as depicted by the blue diamonds in figure 1. For the purpose of data interpretation, the collections were grouped into (a) baseline (September–December 2016, 10 weeks), (b) early peri-intervention (January–March 2017, 6 weeks), (c) post-intervention (September–November 2017, 6 weeks) and (d) late follow-up (September 2018, 2 weeks) (figure 1). However, statistical control charts depict each individual collection dataset (figure 2).

{kind=link}
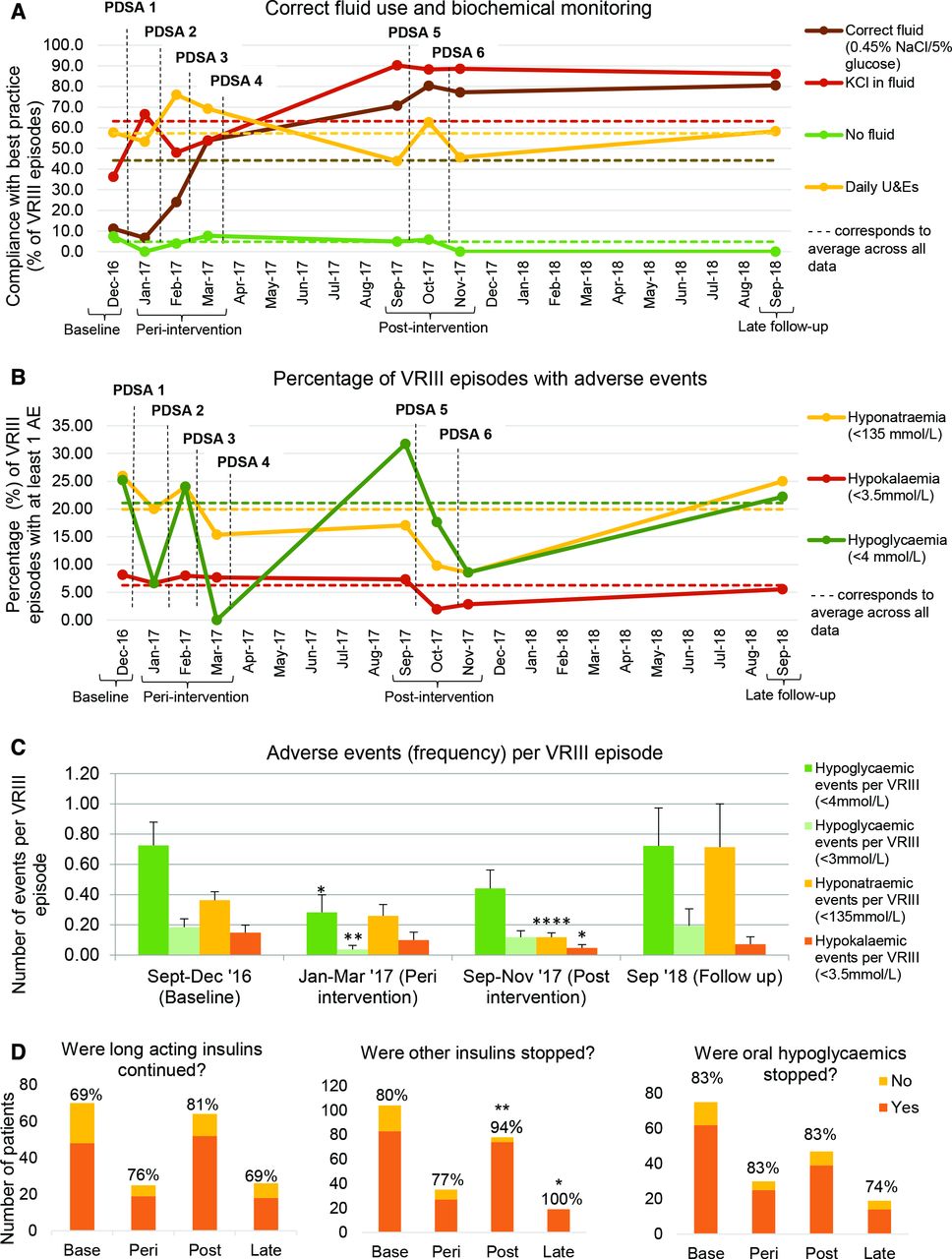{kind=link}
(A, B) Statistical control charts plotting each data collection point against a mean average across the timeline. (C) *P<0.05, **p<0.01, ****p<0.0001 statistical significance using Student’s t-test. Bars represent SEM. (D) *P<0.05, **p<0.01 statistical significance using χ2 test. PDSA, Plan-Do-Study-Act; VRIII, variable rate intravenous insulin infusions.
Statistics
Data analysis and graphic representation was completed using Microsoft Excel 2010. The Student’s t-test and χ2 test were used for statistical comparisons. P values of <0.05 were considered statistically significant. All statistical analyses and subsequent p values were calculated comparing the baseline data with each subsequent data collection. Therefore, all quoted p values relate to a comparison between baseline and the relevant data collection. SDs (±) are quoted in brackets where numerical data are analysed.
Results
The number of VRIII episodes, duration and patient demographics for each auditing period are summarised in table 1.
The availability of an electronic data record meant only one patient was removed from the entire dataset (part of the baseline data group) due to incomplete data. The rate of use of the recommended fluid (0.45% sodium chloride/5% dextrose with 0.15% or 0.3% KCl) increased progressively from a baseline of 11.1%–26.4% peri-intervention (p<0.01) and 76.4% post-intervention (p<0.0001) and remained high on follow-up 1 year later (80.6%) (p<0.0001). A similar improvement was noted in the use of potassium chloride in intravenous fluids, from 36% at baseline to 55% peri-intervention (p<0.05), 92% post-intervention (p<0.0001) and 86.1% (p<0.0001) on follow-up. The number of VRIII episodes where no fluid was used as substrate was also reduced from 7.4% at baseline to 3.8% peri-intervention (p=0.36) and 3.9% post-intervention (p=0.22), although the difference did not reach statistical significance. At follow-up, there were no instances of VRIII use without fluid as substrate (p=0.12). Compliance with daily monitoring of urea and electrolytes proved to be more resistant to change, with initially only moderate but non-statistically significant change (59.1% at baseline vs 67.9% peri-intervention, p=0.26). Post-intervention, there was a worsening of monitoring with reduction down to 51.9% (p=0.25). At follow-up, this change then reverted to the baseline levels of monitoring at 58.3% (p=0.93) (figure 2).
There was a trend towards reducing rates of adverse events with the adoption of the new hospital protocol. The percentage of VRIII episodes associated with at least one hypoglycaemic event (glucose <4 mmol/L) declined from 25% at baseline, 13% peri-intervention (p=0.07), 19.7% post-intervention (0=0.28) and 22.2% at follow-up (p=0.71). For hyponatraemias (sodium <135 mmol/L), the corresponding improvement was more marked, from 26% at baseline to 20.8% peri-intervention (p=0.45) and 12% post-intervention (p<0.01). However, this improvement seemed to dissipate over the ensuing months, with hyponatraemias occurring at least once during 25% of VRIII episodes at follow-up (p=0.91). Similarly, there was a reduction in hypokalaemias (potassium <3.5 mmol/L), noted at 8% of VRIII episodes at baseline and declining to 7% peri-intervention (p=0.89) with further reduction to 4% post-intervention (p=0.15). The reduction remained modest with 5.5% of episodes recording a hypokalaemia 1 year later (p=0.6) (figure 2).
The number of adverse events per VRIII also showed general downward trend with the advent of our imposed interventions. The average number of hypoglycaemic events (glucose <4 mmol/L) significantly reduced from 0.73 (±1.78) events per VRIII at baseline to 0.28 (±0.84) events per VRIII peri-intervention (p<0.05). Unfortunately, there was then a rise to 0.44 (±1.37) events per VRIII post-intervention (p=0.07) and 0.72 (±1.5) at the 1-year follow-up (p=0.49). Similarly, there was a reduction in the severe hypoglycaemic events (glucose <3 mmol/L) from 0.19 (±0.64) events per VRIII at baseline to 0.04 (±0.19) events per VRIII peri-intervention (p<0.01). Again, this improvement did not continue at post-intervention, with the rate of events per VRIII increasing to 0.12 (±0.48) post-intervention (p=0.17) and 0.19 (±0.67) at the 1-year follow-up (p=0.47). For hyponatraemias (sodium <135 mmol/L), there was a significant reduction in number of events from 0.36 (±0.6) per VRIII at baseline to 0.12 (±0.32) post-intervention (p<0.001). At the 1-year follow-up, there was then unfortunately an increase in the number of hyponatraemic events to 0.71 (±1.51) per VRIII compared with baseline. The reduction in hypokalaemic events (potassium <3.5 mmol/L) per VRIII was more sustained, with a significant reduction from 0.15 (±0.54) events per VRIII at baseline to 0.05 (±0.25) episodes per VRIII at post-intervention (p<0.05) and remained low at 0.07 (±0.26) episodes per VRIII at follow-up (p=0.14) (figure 2).
Another important aspect of VRIII management pertains to correct adjustment of insulin and other diabetic medications. Here, we observed substantial improvements in standards of care. Of patients who were on long-acting insulin, the medication was appropriately continued alongside the VRIII in 69% at baseline, with a good improvement to 81% post-intervention (p=0.09). At follow-up, there was a reduction to 69% (p=0.95). Short-acting/mixed insulins were correctly stopped during the VRIII in 80% of patients at baseline, with a statistically significant improvement to 94% peri-intervention (p<0.01) and 100% on follow-up (p<0.05). Baseline compliance with cessation of oral diabetic medications was good, with 83% of episodes having the medication correctly stopped; this was sustained throughout the interventions, with a slight reduction at the 1-year follow-up to 74% (figure 2).
Estimated cost savings
Based on a recent study, an inpatient hospital stay costs 40% more if the patient experiences hypoglycaemia during the stay, the equivalent of approximately £650.8 There was a statistically significant reduction in hypoglycaemic events per VRIII from 0.73 at baseline to 0.28 peri-intervention, equating to around 6 months. Over this time, the estimated number of prevented hypoglycaemic events was 176, based on a calculated average of 15 VRIII episodes per week (390 in a 6 months). This is suggestive of a possible saving of over £100 000 to the trust if the reduction in hypoglycaemic episodes was sustained over further 6 months.
There are a limited number of UK-based studies that have reviewed the specific costs of hyponatraemia or data specific to intravenous insulin-induced hyponatraemia. However, several international large-scale studies have shown the financial burden associated with hyponatraemia is significant in comparison with eunatraemic patients; Corona et al. showed an additional $3000 expense during admission.12 We showed a reduction in VRIII-associated hyponatraemia from 0.36 to 0.12 events per VRIII from baseline to post-intervention (around 12 months), the equivalent of an annual prevention of around 118 hyponatraemic events (based on above figures). The financial savings during the year were likely to be considerable. However, we highlight again the importance of sustainability on savings as 1-year post-intervention, rates of hyponatraemia had risen again.
These considerations are particularly important given that a substantial hurdle to instigating the change to allow widespread availability and use of the JDBS recommended fluid (5% glucose/0.45% sodium chloride with 0.15% or 0.3% potassium chloride) was the relative cost. This fluid costs comparatively more (£3.43/500 mL bag) than other traditionally used fluids such as glucose 5% and 0.9% sodium chloride (£0.70/1 L bag).13 The difference in cost in changing fluids would be around £8600 per annum, based on the average number of VRIII episodes per weekly being 15, and the average length of a VRIII being 16 hours (estimating four bags of fluid required).
Lessons and limitations
VRIII remains an indispensable mode of insulin delivery in challenging inpatient settings but entails important clinical risks which can only be effectively mitigated by the combination of correct insulin infusion rates, appropriate intravenous fluids and close monitoring of relevant biochemical parameters. VRIII is commonly initiated and managed by junior medical staff and nursing staff who lack expertise in diabetes, and therefore it is essential that an easy-to-follow protocol is in place and that awareness of its existence and understanding on how to apply the guidance in daily clinical practice is widespread among healthcare professionals caring for medical and surgical inpatients. The publication of guidelines on intravenous insulin use by JBDS in recent years has generated a new impetus to enhance practice in this area.2 With this QIP, we set out to improve standards of care in our centre implementing the new national guidance.
Evidence for the new fluid
One of the core changes in the JBDS guidelines was the introduction of 5% glucose/0.45% sodium chloride with 0.15% or 0.3% potassium chloride at 83–125 mL/hour as the recommended intravenous fluid choice. This is a balanced fluid which ensures the administration of a sufficient glucose substrate while meeting daily sodium and potassium requirements. This fluid was not available in most UK hospitals prior to the publication of the JBDS guidelines, and as a consequence, familiarity of most clinicians with it used to be low. In our 2015 audit, this fluid had not been locally available.3 At the baseline of our current QIP, it was only used in a minority of patients, but compliance steadily increased during the months of our interventions, so that 9 months later the fluid was used in the vast majority of patients on VRIII. Once this fluid was established as the first-line option, compliance with it proved durable and remained high 1 year later. As was expected, progress in the use of potassium in fluid closely paralleled the improvement in rates of 5% dextrose/0.45% saline fluid use. Interestingly, compliance with daily monitoring of sodium and potassium remained relatively low throughout our project. Possible explanations include an underestimation of the true risk of electrolyte disorders by junior clinicians and the objective difficulties with securing daily biochemical monitoring of inpatients outside intensive care.
Reduction in adverse events
From the data, our interventions delivered a clear, statistically significant improvement in rates of adverse events (hypoglycaemias, electrolyte disorders) that are important both in terms of patient safety and health economics. Considerable previous research has shown that inpatient hypoglycaemia is associated with an increase in length of stay and inpatient mortality.8–10 Similarly, hyponatraemia also comes with a risk to patient morbidity and mortality and financial cost. It has been associated with longer inpatient stay, poorer outcomes in terms of intensive care admission and mortality.12 14–16
The adherence to the correct fluid remained durable which could be a consequence of this fluid becoming entrenched in the hospital clinical practice of VRIII use after being established as a preferred option. Conversely, the reduction in adverse events did not endure, with deterioration at 1-year follow-up, particularly with hyponatraemic events. Practically, initiating a VRIII with a well-established protocol and easily available fluid is simple. However, encouraging good practice with the continued use of the VRIII, such as daily electrolyte monitoring requires more regular intervention to remind staff of their significance, especially in the circumstance of high junior doctor turnover. While speculative, this could be one explanation for the deterioration in adverse events.
Similarly, the increased rates of hypoglycaemia may also be explained by the cohort size at follow-up. While not statistically significant, the rate of hypoglycaemic agents being inappropriately continued and long-acting insulins being inappropriately paused was higher in the late follow-up group, which may have had an effect on glycaemic control and increased hypoglycaemia rate.
Cost savings
While there is limited data on the cost of each specific adverse event (hypoglycaemia, hyponatraemia, hypokalaemia) while on a VRIII, the financial benefits associated with reduction in adverse events is likely to be considerable to the trust; which if extrapolated nationwide would represent a significant saving, in addition to the reduction in patient morbidity and mortality. It must of course be mentioned that ensuring that adverse event reduction is sustained is paramount to continue cost savings and improve patient care. While not specifically reviewed in this project, there is likely to have been a reduction in length of stay given the reduced adverse events, which in itself would have incurred a cost saving to the trust. This could be reviewed in further research.
Improvement in overall care of diabetes
Correct management of pre-existing diabetic medication when starting on a VRIII is important. Our compliance with this across the intervention period and beyond into follow-up was mixed. Continuing long-acting insulins improves glycaemic control while on the VRIII and helps prevent rebound hyperglycaemia once it is stopped.2 17 We showed a trend towards improvement in the correct continuation of long-acting insulin post-intervention, however this improvement then reversed back to the baseline level at the 1-year follow-up. Interestingly, the correct stopping of other insulins improved significantly from 80% at baseline, to 94% post-intervention and 100% at the 1-year follow-up. One explanation for the results would be confusion over which insulins to stop, which would likely be exacerbated without regular reinforcement of the guidelines.
Limitations
Our QI processes led to significant improvement in outcomes in the short term. Analysis of the 1-year data showed attrition of initial benefits highlighting challenges in sustainability of improvement with a wider adoption. This phenomenon is well recognised in QI literature and has been described as ‘improvement evaporation’ and raises the question ‘Does quality improvement improve quality?’.18 Sustainability and spread of QI are influenced by a range of structural issues which in turn lead to consistency in processual and outcome measures. The structural factors as described in literature include the provider factors (frontline staff awareness, skills and agreement) and organisational factors like leadership and safety climate. For success in sustainability and spread of improvement, current literature highlight the requirements of leadership which would include alignment of the initiative with strategic goals of the organisation, multiple levels of leadership for the project, facilitative leadership and leaders’ boundary spanning activities.19 Our limitations were probably not being able to include this high impact project in organisational QI priority list, not being able to have leadership responsibilities for this project through existing Trust governance structures, not being able to encourage sufficient champions to own up local leaderships in ward areas. Our projects leads have made horizontal connections with specialist societies (Association of British Clinical Diabetologists, Diabetes UK, RCPQI Faculty) and the project was presented in national conference but the vertical connections within the organisation could have been better. The Trust in fact has recently revamped its QI strategy and structure after completion of merger of four local hospitals together.
In summary, analysis of our 1-year data highlighted the existing structural limitations and challenges for sustainability and spread of the benefits of project within our organisation at the time.
Conclusion
Through the implementation of new hospital guidelines, reflecting guidance provided by the JDBS in 2014, along with other important interventions such as teaching, presentations and publication of posters in clinical areas, there was a significant improvement in adherence to the correct guidelines and improved outcomes. This was shown with improvement in correct fluid administration and diabetes medication management and reduction in adverse events, with important implications in terms of patient safety benefits and economic savings for the hospital. At the 1-year follow-up, some of these improvements had reversed, which highlighted the importance of following factors for sustaining and spreading improvement: (1) alignment of the project to wider strategic plans of the organisation, (2) a stable and functioning organisational QI structure and (3) multiple levels of leadership. We demonstrated a significant improvement potential and the lesson we have learnt has been the importance of appropriate organisational structure and leadership attributes for sustainment and wider adoption of the improvement.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We would like to acknowledge and thank the following groups: Diabetes Specialist Nurses, Informatics Team, Trainees, Pharmacy, Medicines Management Group and Medical Education Team. The manuscript was shared with Diabetes Steering Group, the body responsible for overseeing Diabetes QIPs under the current quality governance structure of the Trust.
Footnotes
Contributors SG initiated the project and designed the interventions used in the PDSA cycles. He also collaborated with the medicines management team, pharmacy, informatics team and medical education team to ensure quality improvements could be made at each stage. AC helped with data collection and analysis, implementation of interventions and presentation of results at each stage. She also took the lead in writing the manuscript. VC conducted data collection and analysis at the 1-year follow-up mark. He also helped and supported writing and editing of the manuscript. SS helped in design and implementation of interventions in the PDSA cycles. WH provided support and mentorship throughout the project. All authors contributed to edits and approval of the manuscript. SG is the guarantor for the project. Non-authorship contributors were Dr Emily Austin, who helped with project design, data collection and analysis in the first phase of the project. Other contributors to intervention implementation and data collection were Dr Priscilla Sarkar, Dr Niraj Samani, Dr Priya Jalota, Dr Lloyd Rickard, Ms Bridhid Lane, Ms Deborah Dawson and Ms Lesley Peters. Dr Georgios Gkoutos and Dr Victor Roth Cardoso provided statistical support.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.