Article Text

Abstract
Introduction In March 2020, the Dallas Fort Worth Metroplex experienced a surge in acute COVID-19 infections. At that time, no consistent protocols existed for follow-up of discharged patients with COVID-19 from the William P Clements Jr University Hospital at the University of Texas Southwestern Medical Center. Simultaneously, medical students were suspended from in-person clinical activities to limit viral spread. In response to these events, a telemedicine elective was created to provide timely and high-quality telehealth follow-up for recently discharged patients with COVID-19.
Methods The pilot team, consisting of several second-year through fourth-year medical students, developed a call script that included warning signs and symptoms, Centers for Disease Control and Prevention (CDC) guidelines for isolation and primary care physician referral information. Patients with COVID-19 discharged from the emergency department (ED) and inpatient services were identified and assigned to student callers. All patients were discussed with an attending physician, who was available if an acute issue arose. The elective also included education on the SBAR (situation, background, assessment, and recommendation) handover technique, telehealth education, updated COVID-19 literature and CDC guidelines.
Results Improvement was noted in students’ ability to identify patients who required escalation of care, as seen by over 60% of patients who were advised to return to ED required hospital admission. Statistically significant improvement was observed in the students’ degree of feeling informed about the current state of COVID-19 and their degree of comfort with interviewing patients over the phone.
Discussion This elective provided quality virtual healthcare to patients with COVID-19 while allowing medical students to progress in their medical education and participate in patient care.
- COVID-19
- Telemedicine
- Clinical Decision-Making
- Graduate medical education
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Background/problem description
In late 2019, a cluster of community-acquired pneumonia cases was identified in Wuhan, China. Isolation of the causative pathogen of this outbreak led researchers to discover a novel strain of coronavirus.1 Infection with this new human pathogen was noted to cause an influenza-like illness; but unlike seasonal influenza, COVID-19 was more contagious, resulted in higher hospitalisation rates2 and initially lacked an effective vaccine.
Available knowledge
The USA diagnosed its first case of COVID-19 on 20 January 2020.3 By 13 March, the US government declared the COVID-19 outbreak a National Emergency.4 Schools, businesses and public meeting places began closing to prevent the spread, which led to a significant shift in the outpatient care delivery model from traditional in-person appointments to online audiovisual or telephone encounters.
The impact of the COVID-19 pandemic has been felt by all members of the healthcare community, including medical students. With climbing infection rates and shortages in personal protective equipment, the Association of American Medical Colleges issued a public announcement on 17 March 2020, recommending temporary cessation of all clinical rotations.5 As a result, students had to take an indefinite hiatus from in-person patient care activities.
Conducting medical consultations using audiovisual technology first began in the early 20th century6 and by the mid-1900s was used by many, including NASA (National Aeronautics and Space Administration). However, telemedicine never hit the pinnacle of its popularity until the COVID-19 pandemic, where social distancing and self-isolation became crucial to mitigating disease spread.
Rationale
The benefits of implementing a COVID-19 telemedicine elective were twofold. First, medical students could assist hospital staff in tracking the progress of COVID-19-infected outpatients and oversee the safe transition of their care from the hospital to primary care providers. Second, it enabled students to continue developing their skills in patient interviewing, outpatient care management, verbal presentations and telemedicine while unable to complete in-person clinical rotations. A systematic review7 has shown that post-discharge telephone follow-ups significantly improve patient self-management, the likelihood of follow-up appointment attendance, post-discharge health status and patient satisfaction with care. Discharge phone calls also provided an opportunity for healthcare workers to resolve problems related to medication management, re-educate patients on care instructions and give follow-up appointment reminders.
Several studies have discussed the utility of telemedicine during the COVID-19 pandemic.8 An article published in JAMA (the Journal of the American Medical Association) highlighted the impact of the pandemic on pre-clerkship and clerkship education9 but could not identify an original project that used telemedicine to advance medical education and optimise follow-up care for patients with COVID-19 after discharge, thus making this project unique.
Specific aims
The global aim of this quality improvement project was to improve the follow-up rate for COVID-19-positive patients discharged from William P Clements Jr University Hospital (CUH) inpatient and emergency department (ED) services from the baseline of 0 to 100% by the end of June 2020. Secondary aims included improving students’ understanding of COVID-19 and improving their confidence in providing care via telephone calls.
Methods
Study design
After the previously mentioned quality care gap was identified, a medical student pilot team developed a quality improvement project to provide follow-up telephone calls to patients with COVID-19 after discharge from the hospital inpatient or EDs.
Context
This project’s scope was limited to COVID-positive adult patients discharged home from the inpatient or ED services at the CUH. CUH is a large, private general hospital owned and operated by the University of Texas Southwestern Medical Center (UTSW) in Dallas, Texas. The patients contacted during this project had the following demographic makeup: 57% women, 15% were 65 years or older, 33% were 35 years or younger, and 52% were between 36 and 64 years old. Sixty-eight per cent of the patients had a body mass index of 30 or greater indicating obesity. Twelve per cent of patients were Spanish speaking and required a translator to facilitate the call.
Medical students in the clerkship phase of their curriculum were eligible to participate in the intervention created by this project, a 1-month long elective. These students were supervised by internal medicine specialists who work on the inpatient wards at CUH and provide primary care outpatient services at UTSW. The elective began with a pilot phase from 20 April to 1 May 2020. There have since been three 1-month long elective cohorts with five students per month. Data collection took place from April through June. The third elective cohort participated during July 2020 but the data from those patient interactions were not included in the analysis.
Organising
The pilot phase of this project included seven medical students, a nurse manager and two faculty physicians. Students and faculty worked together in the conception and execution of the elective. All students were in the clerkship phase of their education and were unable to return to on-site clinical activities due to the COVID-19 pandemic.
Intervention
The project team developed clinical protocols and a process map to improve efficiency and workflow during the elective (figure 1). A script was written to facilitate student callers’ conversations with patients regarding their symptoms and Centers for Disease Control and Prevention (CDC) guidelines. The script included open-ended questions to assess patients’ general health, followed by more specific questions to identify warning signs/symptoms that could indicate worsening of their disease and need to escalate care to an attending physician and/or recommend a return to the ED. The script also included CDC guidelines for self-quarantine and safe discontinuation of isolation, primary care physician referral information, crisis hotline numbers and a Health Insurance Portability and Accountability Act-compliant voicemail template if they were unable to reach the patient.

This process map details the workflow on a given day regarding completing telemedicine follow-up calls to COVID-19 patients. A much more detailed version is available if readers are interested in implementing a similar project at their institution.
Each day, the nurse manager would compile a list of patients with COVID-19 discharged 2 days prior from the CUH ED or inpatient services and route the patient charts via the EPIC electronic medical record (EMR) messaging system to the on-call students and the supervising physician. For Spanish-speaking patients, students would contact the CUH translation service to arrange a conference call with the patient, student and translator. A maximum of three call attempts were made over a period of 2 days, followed by a final call to the protected health information designee as a last resort. Patients were excluded if discharged to a long-term acute care facility or if they had already received a follow-up phone call from a healthcare worker on the same day as the call assignment, presuming they would already have adequate care.
If the patient reported any warning signs as described in the call script, the student would follow the escalation protocol, which involved ending the call and immediately paging the supervising physician. The attending physician would contact the student to receive an appropriate patient handoff and discuss the care plan. Then the student or physician would contact the patient to review recommendations. All telephone encounters were documented in the patients’ EMR using the note templates created by the project team and EMR specialists.
A debrief session was held at the end of each day for students to verbally present their assigned patients and discuss management plans with the supervising physician, if not already discussed previously. These meetings allowed the team to consistently re-evaluate the current processes, highlight problem areas and brainstorm solutions.
Throughout the elective, the students attended weekly interactive, virtual didactic sessions to master the SBAR (situation, background, assessment, recommendation) handover technique used to present patients in the debrief. Activities increased in complexity as the elective progressed and required students to incorporate clinical knowledge into their SBAR handovers. Students also worked remotely with attending physicians in a multispecialty clinic using the audiovisual platform Bluejeans to address the general healthcare needs of COVID-19-positive patients, as they were not able to see their providers in person.
The quality improvement tool ‘Plan, Do, Study, Act’ was used to identify the most beneficial changes and the protocols that could be refined or discarded based on analysis of each cohort completing the 4-week elective. Once these changes took place, the team used Failure Mode and Effects Analysis to determine if the suggested changes served as adequate solutions.
Measures
The project team collected pre-elective and post-elective survey data from 15 medical students involved in this intervention (five students per each of three elective cohorts) to assess the change in confidence with telemedicine and knowledge regarding COVID-19. Students elicited feedback from patients at the end of their conversation to determine if patients believed this interaction improved care regarding their COVID-19 infection. Process measures included the following: the average number of attempts needed to reach a patient, the number of successfully completed follow-up calls (defined as a call in which the student was able to reach the patient and complete a conversation using the call script) and the percentage of calls that were escalated to a physician due to a patient screening positive for any warning signs/symptoms listed in the script. Outcome measures included the following: ED return-discharge rate (refers to patients advised to return to ED based on call script parameters who were then discharged from ED after evaluation), and ED return-admission rate (refers to patients advised to return to ED based on call script parameters who were then admitted to the hospital after evaluation). Balancing measures included physician-based satisfaction with student handovers, students’ comfort level with virtual delivery of follow-up care, and patients’ satisfaction and understanding of the care they received. The patients’ satisfaction was assessed by asking if they thought the call was useful at its conclusion. Their understanding was assessed by asking if they felt confident in explaining the CDC discontinuation of isolation guidelines to a friend.
Patient and public involvement
Patients were not involved in the design or conduct of this project. Patients were recruited to join the study based on search of EMR for patients recently discharged from CUH with a new diagnosis of COVID-19 and provided verbal informed consent.
Results
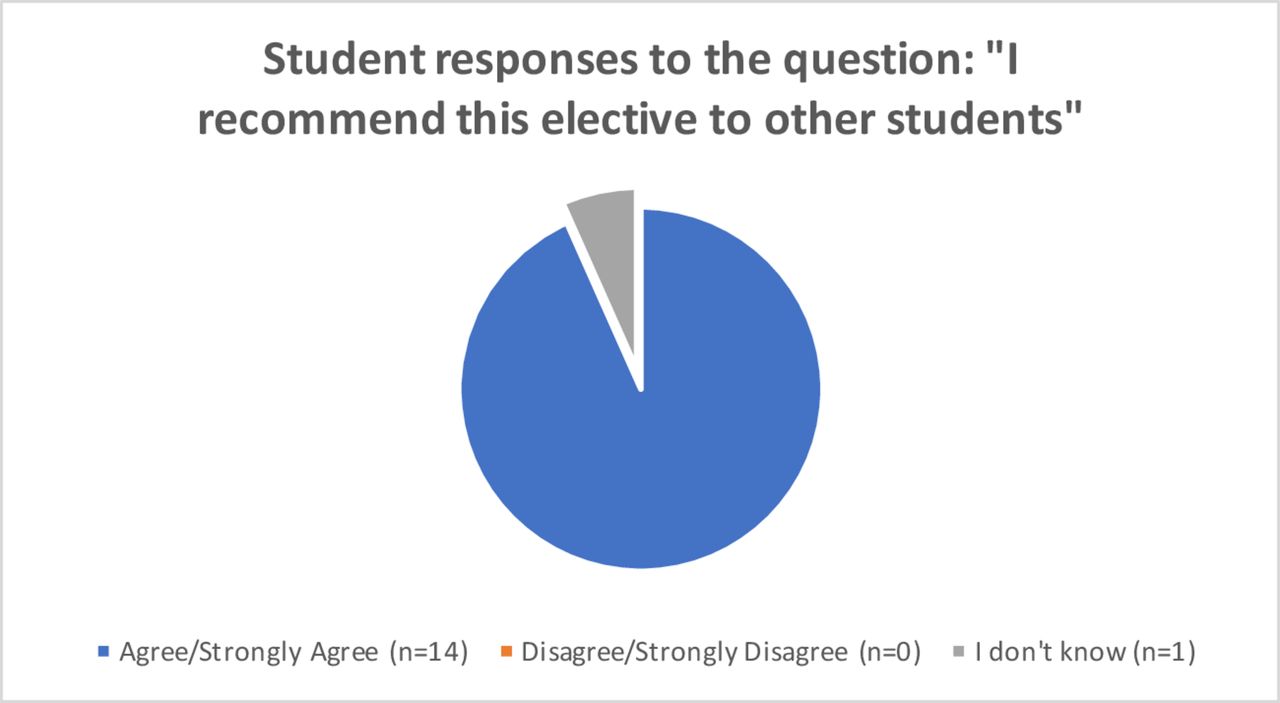
The results of this project include analysis of student responses to a pre-survey and post-survey, data from patients’ EMR and information collected over the phone. Our primary outcome was the per cent of patients who were able to be contacted via this elective to provide follow-up care. By the end of the data collection period, 75% of patients were successfully contacted. The baseline for this outcome measure was zero because there had previously been no patients discharged with a diagnosis of COVID-19 and we had no way to track the patients who were discharged early in the pandemic prior to the creation of this project. Patients were also polled at the end of the phone call to garner feedback on their experience. The student survey consisted of 20 questions, but the top three most pertinent to the aims of this study were the degree of agreement with the following statements (figure 2). The first was ‘I believe that with a proper understanding of telemedicine, I can deliver the same level of follow-up care during an audio or audiovisual encounter as I would during an in-person encounter with the patient’. The second statement was ‘I feel informed about the current state of COVID-19’. The final statement analysed was ‘I feel comfortable interviewing patients over the phone’. In the post-survey, a statistically significant increase to 100% agreement with the latter two statements was seen (p=0.035 and p=0.011, respectively). Also, 100% of students responded that they would recommend this elective to a fellow student and 93% of students said that they could see themselves incorporating telemedicine into their future practice (figure 3).
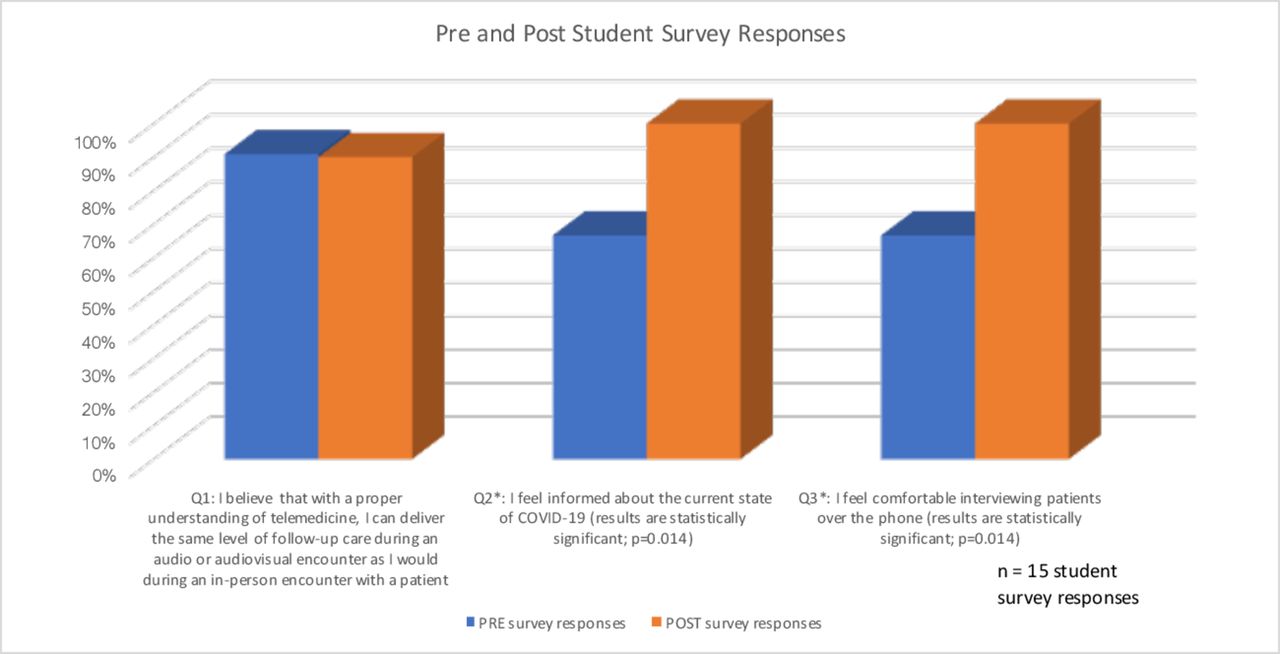
This chart shows students’ responses to the above survey questions before and after completing the elective. There was a significant increase from baseline to 100% agreement with the statements “I feel informed about the current state of COVID-19” and “I feel comfortable interviewing patients over the phone”.
{kind=link}
{kind=link}
{kind=link}
These pie charts are elective student responses compiled across the three cohorts in response to survey questions. Their responses showed 100% agreement with the statement “I recommend this elective to other students”, and 93% agreement with the statement “I can see myself incorporating telemedicine into my future practice”.
Discussion
Summary
The project team believes the intervention created was successful in filling the identified quality care gap by providing necessary follow-up for COVID-19-positive patients and allowing medical education to proceed during a pandemic, based on the analysis of patient care data and survey results. The follow-up calls encouraged patients who were not clinically improving or deteriorating to seek additional medical care. After completing the elective, students reported increased agreement with the statements ‘I feel informed about the current state of COVID-19’ and ‘I feel comfortable interviewing a patient over the phone’. Every student reported that they would recommend this elective to a classmate.
Interpretation
The findings gathered during this project indicate that the elective was successful. The phone calls served an integral role in improving patient safety as a large portion of the patients who were advised by a medical student or physician to return to the ED ended up requiring admission (ED return-admission rate of 57% in April and 64% in May). This ED return-admission rate was determined by subsequent EMR review. Patient feedback surveys also revealed a general belief that the phone calls were helpful. Students felt more informed about COVID-19 and telemedicine by the end of the elective and reported that it was a worthwhile clinical experience.
Limitations
The generalisability of the study findings is limited by single-site intervention and the tailoring of protocols to meet the healthcare demands of the mostly privately insured patient population at CUH. For the indigent population, current protocols may not achieve the same quality of care delivery due to difficulties accessing healthcare resources, communication technology and transportation services. Other project limitations included an inability to reach some patients by phone or leave a voicemail as well as a lack of access to audiovisual communication tools for a more thorough assessment. Another limitation was that the assessment of patients’ satisfaction and understanding of the care they received was not recorded due to inherent response bias. In a setting where information is rapidly evolving, establishing a COVID-19-centred curriculum is difficult as it requires frequent modifications and updates as new information arises. If cases increase, the student team may not be able to balance the heavy patient load and provide quality care. As such, the number of phone calls was already to the point that students only followed up on patients who had concerning signs or symptoms and were encouraged to go to the ED. This means that patients could have been missed who presented to the ED after a phone call but had not been told to go from a student as they did not have symptoms consistent with the warning signs taught to students. If the number of cases drops, there may not be enough patients for each student and the quality of learning is diminished. Since this project was a single-site intervention, only a handful of CUH physicians were recruited to supervise the student callers. If the attending physician was called away to other responsibilities, the elective would not be able to function due to the lack of oversight. Additionally, their limited availability meant there was less time for teaching during debriefing sessions. The low number of students surveyed regarding their elective experience led to a diminished power to the study which can only be remedied by further iterations of the elective to get more student responses.
Sustainability
The pilot team is working to make the elective more sustainable by removing the necessity of student facilitators to oversee the process. The team has developed an orientation video to send to new elective students before their first day to introduce information about the elective and the process of making calls to remove the need for a facilitator to lead them through the protocol. The SBAR training sessions have also been updated to include audio clips on each presentation slide to walk the students through the activities while remaining an interactive module. In the future, the project team would like to expand this by creating a video module with which students can interact by clicking buttons that change situations in the preset scenarios. This would help to educate students so that future iterations of this elective could increase student responsibilities for triage decision-making.
The project was conceived to fill a need created by the COVID-19 pandemic. Increasing numbers of patients were being diagnosed with COVID-19, a novel pathogen with limited facts available to both the public and providers. When patients were discharged after having received a frightening diagnosis, they had limited access to physicians for follow-up care. Telemedicine has not traditionally been included in medical student education but is becoming more widespread in healthcare, especially due to the pandemic, so it is important to teach healthcare professionals how to use it successfully. The next steps for this project include disseminating the elective model to other hospitals to reach additional patients. This elective format could also be used in other clerkships and courses in medical school curriculum, such as incorporating telemedicine into ambulatory outpatient clinic visits.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
Patient follow-up and student participation were optional. All patient information remained confidential according to Health Insurance Portability and Accountability Act (HIPAA) regulations. Data were collected and stored on Microsoft Teams, a HIPAA-compliant software. Before beginning phone conversations, medical students required provision of two patient identifiers. If a voicemail message was necessary, no protected health information was recorded.
Footnotes
Contributors All authors were members of the pilot team creating this telemedicine elective. IW is the guarantor. IW, MIM and DM wrote the manuscript. HZ assisted in editing the manuscript. MR wrote the results section and created figures. EP and GR provided support and assistance with editing and submitting the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.