Article Text

Abstract
Breast pain has no association with breast cancer yet is a frequent reason for referral from Primary to Secondary Care, often on an urgent (2-week wait) referral. The referral often causes significant patient anxiety, further heightened by screening mammograms and/or ultrasound scans in the absence of an associated red flag symptom or finding by the patient or general practitioner. This paper reports the pilot implementation of a specialist Primary Care Breast Pain Clinic in Mid-Nottinghamshire where patients were seen, examined without any imaging and assessed for their risk of familial breast cancer: numerous studies have reported 15%–>30% of patients with breast pain only have a family history of breast cancer.
177 patients with breast pain only were seen in this clinic between March, 2020 and April, 2021 with a 6-month interim suspension due to COVID-19. The mean age of patients was 48.4 years (range: 16–86). 172/177 (97.2%) patients required no imaging although there were three (1.7%) inappropriate referrals and two additional abnormalities (1.1%—hamartoma, thickening/tethering) that were referred onward. There were no cancers. 21 (12.4%) patients were identified to have an increased familial risk of breast cancer and were referred to the specialist familial cancer service. 170/177 patients completed an anonymous questionnaire on leaving the clinic. 167/169 (99%) were reassured regarding their breast pain, 155/156 (99%) were reassured of the Familial Risk Assessment, 162/168 (96%) were reassured regarding their personal risk assessment while 169/170 (99%) were ‘extremely likely/likely to recommend the service’.
This specialist Primary Care Breast Pain Clinic provides service improvement across all levels of care (Primary, Secondary and Tertiary). Patients were successfully managed in the community with high levels of patient satisfaction and together this obviated referral to secondary care. The familial breast cancer risk assessment also helped identify unmet need in the community.
- healthcare quality improvement
- hospital medicine
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The Primary Care Breast Pain Clinic is a novel service, and first in the UK, tackling the rising tide of breast symptomatic clinic 2-week wait (2WW) referrals. Attempts at managing some patients appropriately within the community, using existing structures, have to date had a limited impact.
Breast cancer is the most common cancer in the UK, accounting for 15% of all new cancer cases. There are around 55 200 new cases of breast cancer every year with incidence rates projected to rise only 2% by 2035.1 Meanwhile large proportions of patients are currently being referred to specialised cancer services with breast pain who are at no increased risk of breast cancer based on breast pain alone. In the absence of cancer related symptoms, these patients should not be automatically referred to specialist services on an urgent diagnostic pathway.2
In 2000, the NHS Cancer Plan3 introduced a 2WW standard from urgent general practitioner (GP) referral for suspected cancer to first hospital assessment. In 2010, the 2WW standard was expanded so that any patient referred with breast symptoms would be seen within 2 weeks, whether cancer was suspected or not.4 Breast cancer is the only tumour site to which this standard applies. The standard includes breast symptoms not covered by the National Institute for Health and Care Excellence (NICE) referral guidelines for suspected cancer, including those with breast pain alone.5 6
Nationally, there is an increasing demand for 2WW breast clinic referrals leading to delays to the patient pathway and failure to meet cancer treatment targets.7 8 The necessity of additional 2WW clinics and out-of-hours clinics is evidence current capacity has already been breached. This situation has been exacerbated by the COVID-19 pandemic which has reduced clinic capacity for staffing and infection control reasons. As a result, many services are struggling even with these additional out-of-hours and weekend clinics. This is unsustainable with already fatigued staff and the pressure of recovery and restoration of paused services such as breast screening during the pandemic. Transformation of the current pathway is urgently needed to help alleviate these pressures.
Literature review
Breast pain (mastalgia) may be cyclical (worse before a period) or non-cyclical, originating from the breast or the chest wall, and occurs at some time in 70% of women.9 The absence of a causal relationship between breast pain and breast cancer is highlighted in table 1.
Reports of patients presenting with breast pain only
These publications included patients across nine decades of life (range 12–92 years of age) presenting with breast pain only.10–21 Six thousand two hundred and fifty-seven patients were identified with breast pain only across 13 studies. Twenty-nine cancers were identified in this group (0.46%), or equivalent to 4.6 per 1000 patients. Since the year 2000, 5101 patients were identified across 11 studies with 19 (0.37%) cancers identified, or 3.7 per 1000 patients. Of those patients found to have breast cancer where the side was recorded (n=20), 11 were regarded as concordant with the side/site of the pain. Otherwise, the cancer was regarded as non-concordant. This 50:50 split between concordant and non-concordant was maintained even in studies which reported focal breast pain.
Overall the studies show that the chance of a patient having breast cancer is very low when presenting with breast pain alone—well below the level recommended for population-based screening in the National Health Service (NHS)—but also that half of the cancers detected were not concordant with the patients symptoms. This latter finding further indicates that finding a breast cancer in a patient with breast pain only is simply coincidental and indeed the incidence of breast cancer in the concordant breast is ~1.9:1000.
Conversely, where family history was reported in these publications, more patients with breast pain had a significant family history of breast cancer than what you would expect to find within the population—ranging from 15%–30%, with one study reporting 38% for breast and ovarian family history.
Studies have highlighted the ‘Overutilization of healthcare resources for breast pain’. One study of 799 patients with a mixture of diffuse (30%), focal, (30%) and non-localised (40%) breast pain reported on the number of imaging examinations performed.20 Six hundred and twenty-four mammogram examinations were performed along with 550 breast ultrasounds and 8 MRIs. A further 17 image guided examinations were performed to enable a biopsy to be taken. For all these imaging examinations (n=1199) one breast cancer in the contralateral breast was diagnosed.20 In another study of 953 patients (794 with no personal history of breast cancer+123 with a personal history of breast cancer and 36 ‘unknown’) the authors reported 1578 imaging tests.21
Secondary care audit
At the same time, as the Primary Care Breast Pain Clinic pilot implementation was being launched in Mid-Notts, the authors performed an audit of their 2WW clinic in the neighbouring University Hospitals of Derby and Burton (UHDB) Breast Unit. Details of the results are included in table 1.
The purpose of this project was primarily to improve the care women with breast pain only receive through (i) establishing a dedicated Primary Care Breast Pain Clinic, (ii) improving service and patient experience, (iii) safely remove inappropriate imaging and (iv) identifying unmet need in breast cancer family history, while at the same time (v) reducing the demand on urgent 2WW referrals
Intervention: implementation of Primary Care Breast Pain Clinic
Mastalgia pathway
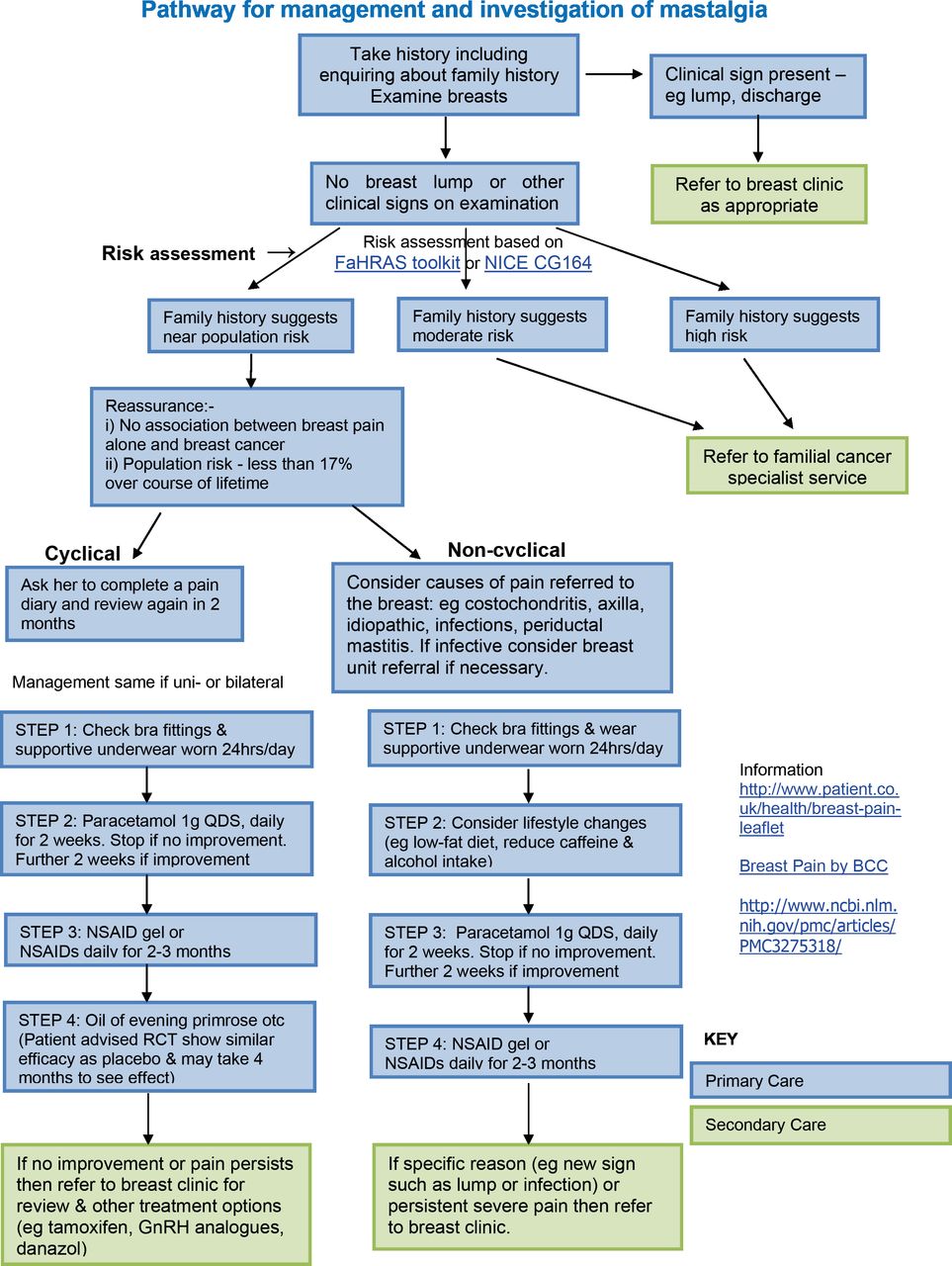
The pilot implementation of the Primary Care Breast Pain Clinic was informed by the mastalgia pathway developed by the breast team at Royal Derby Hospital, NHS Foundation Trust. The pathway (figure 1) has subsequently been endorsed and supported regionally and beyond by the East Midlands Expert Clinical Advisory Group, the Association of Breast Surgery and the East Midlands Primary Care Transformation Group. It also was included as an exemplar of good practice in the annual NHS England and NHS Improvement (NHSEI) Getting It Right First Time Breast Surgery report.
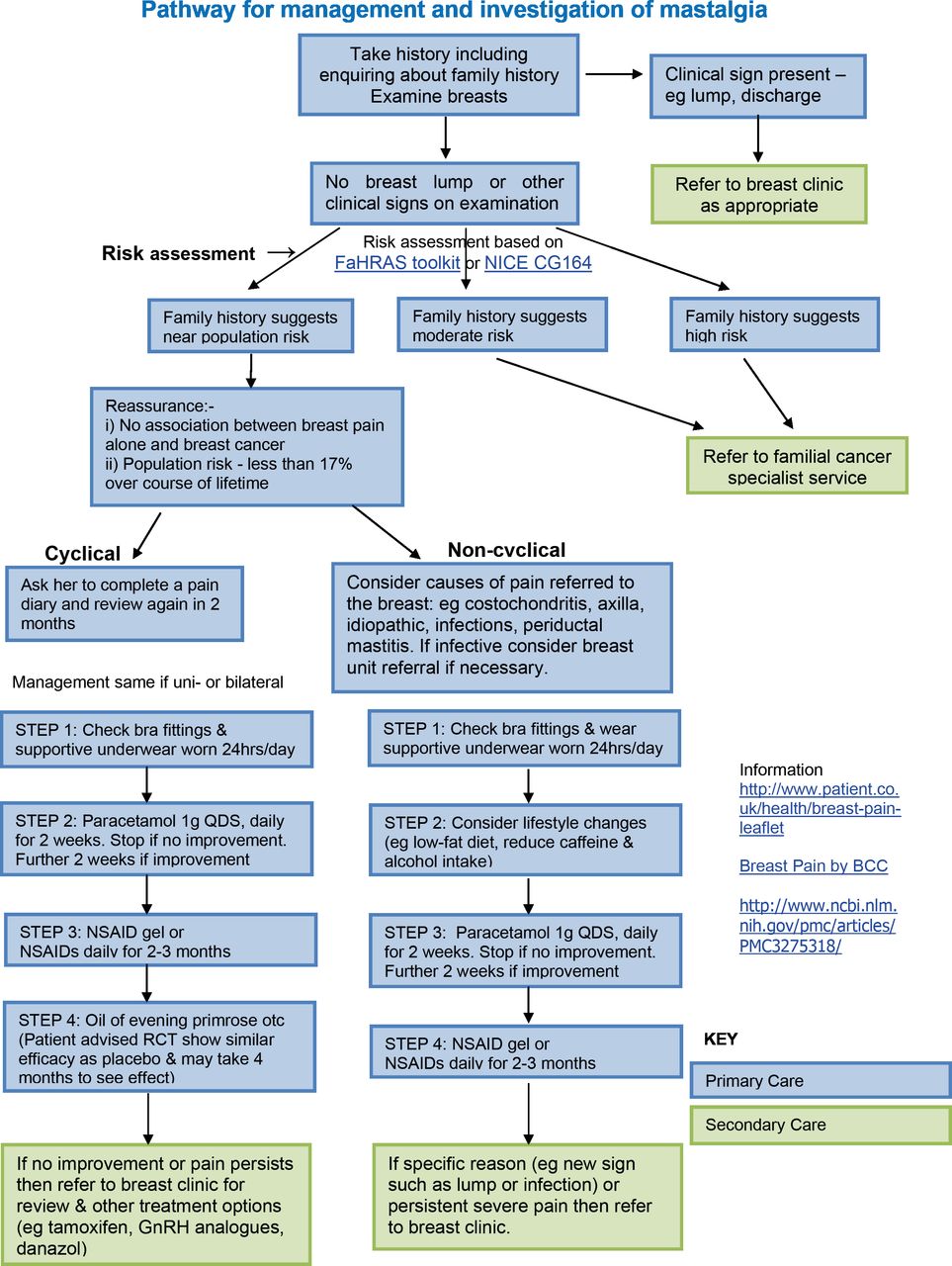
Mastalgia Pathway - Management and Investigation of Mastalgia. FaHRAS, Family History Risk Assessment Software; GnRH, Gonadotrophin Releasing Hormone; NICE, National Institute for Health and Care Excellence; NSAID, Non Steroidal Anti-Inflammatory Drug; RCT, Randomised Controlled Trial.
There are three important components of the mastalgia pathway that are as follows:
Reassurance: the patient is reassured that breast pain alone is not a symptom associated with cancer—that is, does not per se put the patient at increased risk compared with the normal population.
Examination: the patient is examined to confirm the patient’s own findings that there is no clinical abnormality such as a lump or other cancer related symptoms. If a clinical abnormality is found referral is made to 2WW diagnostic clinic as specified within the pathway.
Risk assessment: the patient receives a risk assessment based on their family history. Those identified at ‘near population’ risk are managed within Primary Care for their breast pain. Those at increased risk have their breast pain managed within Primary Care and are referred to the specialist familial cancer service as specified within the pathway.
Familial Risk Assessment
When an individual without any personal history of breast cancer presents with breast symptoms, such as breast pain, it is advised to perform a two-generation Familial Risk Assessment as per NICE clinical guidance CG164. It also recommends that tools such as Family History Questionnaires (FHQs) and computer packages exist and should be made available within Primary Care to inform a risk assessment.22 As such, the Family History Risk Assessment Software (FaHRAS)23 was used alongside a questionnaire to gather family history information and provide decision support in risk assessing these individuals. The FaHRAS risk assessment tool is a hosted, web-based service that is securely provided over the NHS N3 network. The tool provides a risk assessment in line with the recommendations made for Primary Care by NICE clinical guidelines 164 for familial breast cancer. Information is gathered from the patient with a supporting questionnaire and is inputted into a simple, quick-to-use, step-by-step interface. An objective, patient specific assessment is generated and stored with supporting patient outcome letters, based on the reason provided and NICE-recommended action. The FaHRAS tool was previously validated in the primary care setting through a study in Derbyshire that aimed to improve identification of familial breast cancer risk. The study showed the tool was fit for purpose and was beneficial in facilitating pathway improvements.24 FaHRAS has also been shown to be accurate and easy to use within a specialist setting, enabling clinicians to become more efficient gatekeepers to genetic services.25 The FHQ was used in this previous study alongside the FaHRAS tool and was also validated independently as a self-administered tool that enabled identification of those warranting specialist referral within Primary Care.26
The designations of ‘near population’ and ‘moderate/high’ risk were made as per NICE guidelines.21 Near population defined as 10 year risk of breast cancer <3% between age 40 and 50 years and a lifetime risk of less than 17%, moderate risk defined as 10-year risk of breast cancer of between 3% and 8% between age 40 and 50 years and a lifetime risk of between 17% and 30%. High risk defined as 10-year risk of breast cancer >8% between age 40 and 50 years and a lifetime risk of >30%.
Clinic organisation
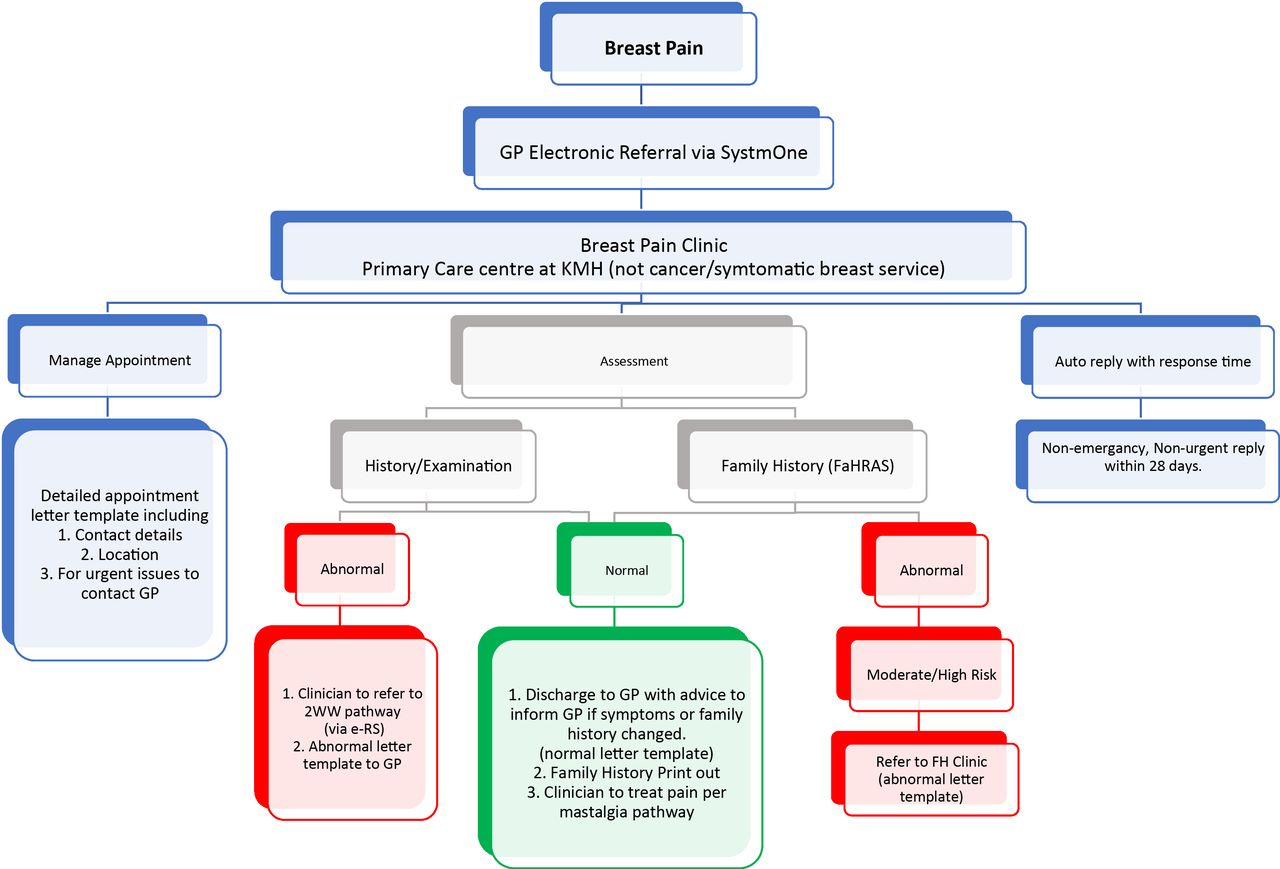
The standard operating procedure for the management of breast pain at the Mid-Nottinghamshire Breast Pain Clinic (figure 2) was developed by the Breast Unit at Sherwood Forest Hospitals Foundation Trust in collaboration with the Mid-Nottinghamshire Clinical Commissioning Groups to coordinate the administrative function of the clinic. This built on the key principles of the mastalgia pathway to ensure effective clinical care while embedding the pathway in the administrative work stream.
{kind=link}
{kind=link}
Management of Breast Pain in the clinic. GP, general practitioner.
Referrals
Patients the GPs would have referred to the Secondary Care symptomatic breast clinic were referred to the Primary Care Breast Pain Clinic by their GP electronically via the agreed pathway: the referral criteria included breast pain only and no sign of cancer reported by the patient or found by the referring clinician on examination. This pathway is separate to the suspected breast cancer pathway: erroneous referrals of patients with breast pain only were transferred to the correct pathway—that is, the mastalgia pathway. All referrals to the breast pain clinic were vetted by an experienced breast clinician.
Preclinic preparation
The FaHRAS FHQ, with supporting guidance on completion, was sent to all patients with their appointment letter and they were asked to complete the questionnaire in advance of their appointment. They were supported in this by the clinic coordinator on the day of the appointment, if required.
Clinic
The Breast Pain Clinic was run weekly with up to 13 patients in a 4-hour session. The clinic was staffed by an experienced breast clinician (an advanced nurse practitioner) and a clinic coordinator. Patients were advised to arrive at least 15 min prior to their appointment time. On arrival at the clinic the FHQ was received by the coordinator at reception and inputted into the FaHRAS risk assessment tool. A printout of this assessment was provided to the clinician. The patient was provided with a chaperone where required and received a consultation in line with the mastalgia pathway. The outcome of the risk assessment and breast examination was recorded on a dedicated clinic pro forma. Patients were advised of the outcome and received an information pack including the clinic pro forma, risk assessment outcome and supplementary educational information, such as breast awareness leaflets, in line with NICE guidance.
Measures: data audit
As part of the clinic audit, patient feedback, clinic output and follow-up data were collected. Patient feedback was gathered qualitatively using an anonymous questionnaire that was provided to the patients as they left the clinic.
Results
Secondary care audit (UHDB)
Over the 7-week period, 214 female patients presented with breast pain out of a total number of 1227 2WW referrals (17.5%). These 214 women were out of a total of 1063 women (20.1%) referred on a 2WW referral. The age range was 18–83 years. Of these, 125 had pain as their only breast symptom: 20% had no imaging while the remaining 80% had breast imaging (53% mammograms only, 16% ultrasound only and 11% both mammograms and ultrasound). All the imaging was classed as normal or benign. There were no breast cancers diagnosed. 121 patients had a family history recorded of which 32 (26%) had a moderate-high risk of breast cancer.
Primary Care Breast Pain Clinic patient feedback audit
A total of 177 patients were seen across a 14-month period between March 2020 and April 2021 with a 6-month interim suspension due to COVID-19 (table 2). The mean age of attendees was 48.4 years (range: 16–86). Data collected is shown in table 2.
Mid-Nottinghamshire Breast Pain Clinic audit
All anonymous patient feedback (table 3) reported 99.4% would likely recommend the service with extremely high levels of reassurance. The vast majority (97.2%) required no imaging although there were 3 (1.7%) inappropriate referrals and 2 (1.1%) additional abnormalities (a hamartoma and a thickening/tethering) that were referred onward. There were no cancers and 21 (11.9%) identified at increased familial risk.
Mid-Nottinghamshire Breast Pain Clinic patient feedback
Discussion
Mid-Nottinghamshire Primary Care Breast Clinic is to our knowledge the first to demonstrate that patients with breast pain only, can be successfully managed in the community with improved patient care, reduce secondary care referral, addressing unmet family history, and with a high level of patient satisfaction.
There have been numerous unsuccessful attempts at transferring the management of patients with breast pain back from Secondary Care into Primary Care, including attempts by Secondary Care specialists at educating local Primary Care practitioners. The likely reasons why this has not been widely successful include:
GPs may have been reluctant to state and reassure patients that breast pain only is not a sign of breast cancer.
It is important for the clinician who examines the patient to be experienced in clinical examination of the breast. The vast majority of GPs simply do not see enough cancers and do not have the necessary breadth of clinical experience of examining the normal breast across the spectrum of ages.
It has also been reported that GPs have limited confidence in assessing familial risk and in ‘counselling on risk’.27 Indeed prior attempts in Mid-Notts at managing patients within the community using existing structures had a limited impact on reducing 2WW referrals.
Therefore, centralising the management of these patients within a specialist Primary Care setting was deemed crucial to provide effective patient care.
The key outcomes of this implementation were the establishment of a dedicated Primary Care Breast Pain Clinic that met the following criteria:
Reduce the demand on 2WW referrals.
Improve service and patient experience.
Providing an objective risk assessment per NICE clinical guideline 164.
Provides mutual security for patient and provider.
Identify unmet family history need.
Safely remove inappropriate imaging.
This transformation project has brought service improvement to Primary, Secondary and Tertiary Care. Primary Care now provides improved patient care with reduced Secondary Care referral costs. The service also addresses unmet need on an equitable basis in the early identification of those at increased familial cancer risk which fulfils local Integrated Care System’s objectives.28 The mastalgia pathway provides security to the provider through the objective clinical standards that are professionally endorsed. The objective risk assessment filed in the patients’ case notes provides additional reassurance both for the patient and for service providers that appropriate classification and care was provided. It also provides a historical record in a patient’s case notes should a patient return at a later date with a different family history, for example, they may have developed breast cancer and then subsequently identified that other relative(s) also had the disease.
For Secondary Care, a major service improvement is the reduction in 2WW referrals and subsequent freeing of resources (staff, clinic costs, imaging resources). These can be reused for other purposes, for example, to expand and improve familial history services to deal with the unmet need identified in Primary Care, to free up imaging resources for breast screening which is also struggling to meet its targets in many services, etc. The absolute reduction in 2WW referrals will depend on the size of the breast unit and the total number of 2WW referrals. For Mid-Nottinghamshire the community breast pain clinic freed up patient appointments for 13 suspected cancer patients per week at Sherwood Forest Hospitals which is a relatively small breast cancer service. Based on this data, several clinics worth of Ssecondary Care clinic capacity could be freed up for larger breast services.
For Tertiary Care, the increased detection of high-risk families should increase the detection of patients and families with genetic mutations (eg, BRCA1 and 2, PALB2).
Importantly, the transformation project has significantly improved patient care and experience. Previously patients attending Secondary Care came with high levels of anxiety, exacerbated through being ‘medicalised’. Their GP had referred them to the breast unit as a 2WW referral, they sat in a clinic with women who were genuinely at increased risk of breast cancer and then received further imaging. All of which engendered a feeling that medical professionals were anxious that their presenting symptom of breast pain might be a sign of breast cancer. By managing the patients in a Primary Care Breast Pain Clinic correct signals are sent to patients from the outset. There are also practical benefits such as local delivery of care, reduced travel time, addressing unmet need with the potential for identification of familial risk, preventative measures for those identified and, ultimately, early detection of breast cancer.
The role of Primary Care at the front end of a cancer pathway can be broadly categorised as meeting one or more of the following requirements: (i) being part of screening programmes, (ii) comprehensive clinical assessment, (iii) carrying out necessary investigations to aid diagnosis and as part of subsequent referral and (iv) compliance with agreed referral protocols. Traditionally, once a patient has been referred during the initial stages of the patient journey, the role of Primary Care can be limited in helping to ease the pressures on a timed pathway. The Primary Care Breast Pain Clinic is a proactive Primary Care input to offer transformation in addressing downstream issues. In general, nearly one fifth of referrals to a 2WW breast clinic are for breast pain. Equally there is an overlapping cohort of patients who have ongoing health anxieties around family history. This cohort of patients is best served by referral to a non-cancer pathway to avoid unwarranted investigations and worsening health anxieties due to being referred to a ‘cancer’ service. Not only is this a more effective use of resources but it enhances patient experience. As patients have a complete family history risk assessment based on NICE guidance, this clinic is keeping with integration and achieving NHSE ambition of triple aim.29
One perceived limitation of this report might be that it does not provide evidence that the patients did not simply re-present at a neighbouring unit with the same symptoms to make sure they get a mammogram or that the patients did not re-present to Primary or Secondary Care some months later with the same symptoms. These data were not routinely collected and indeed are not routinely collected for the current 2WW patients either so that even if the data were available for the Primary Care Breast Pain Clinic it would not have been possible to compare them to the current standard management. Implementation of Primary Care Breast Pain Clinics is now being rolled out more widely across the UK with the support of regional Cancer Alliances. A core dataset is being collected for audit purposes which will be able to provide data on subsequent presentation with breast cancer in this population of patients with breast pain only. What this clinic does do is (i) to triage those patients who should have regular mammographic screening because of their increased familial risk and (ii) advise women within the age range for the NHSBSP that they should attend for regular screening mammograms. This results in more focused and appropriate use of radiological resources than random, opportunistic imaging of patients being referred to Secondary Care breast units with breast pain only.
Conclusion
The pilot Primary Care Breast Pain Clinic has been implemented and shown to provide service improvement across all levels of care (Primary, Secondary and Tertiary). Most importantly it provides improved patient care. The next step is widespread implementation and this has already ongoing across a number Cancer Alliance regions, CCGs and ICPs in England.
Ethics statements
Patient consent for publication
Acknowledgments
We thank the breast surgeons at the Royal Derby Hospital for their advice on the mastalgia pathway and breast unit staff for assistance in collecting audit data. We thank the commissioners within Mid-Nottinghamshire CCGs and managerial team at Sherwood Forest Hospitals for their service oversight. We thank the Primary Care Stratified Medicine research group at the University of Nottingham, and in particular Professor Nadeem Qureshi, for the provision of the Family History Questionnaire (FHQ). We thank FaHRAS for their role in promoting pathway transformation and support of the service implementation. We are also grateful to patients who participated in the anonymous questionnaire and follow-up audit.
References
Footnotes
MJ and TB are joint first authors.
Presented at Association of Breast Surgery annual meeting 2021
Contributors Conception and design: MJ, TB, VR, MS, JR. Collection and assembly of the data: MJ, NM VR, JR. Data analysis and interpretation: MJ, TB, NM, VR, MS, JR. Manuscript writing: MJ, TB, NM VR, MS, JR. Guarantor: JR.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests TB is GP with special interest in breast cancer, clinical lead for Integrated Care Partnership in Mid-Nottinghamshire. MJ is a breast surgeon with interest in breast cancer and identification of familial risk. JR is a breast surgeon with an interest in early cancer detection and has consulted for AstraZeneca, Bayer, Carrick Therapeutics and Cullinan Oncology. He also has provided expert testimony for AstraZeneca. He holds shares in Oncimmune Holdings, FaHRAS Ltd and Carrick Therapeutics.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.