Article Text

Abstract
Efficient handover of patient care is integral to clinical safety. Barriers in communication can lead to adverse outcomes. The Integrated Liaison Assessment Team (ILAT) has a daily handover meeting which presents several challenges to the multidisciplinary liaison team (MDT including high patient turnover, differing staff shift-work patterns, presence of visitors/students and lack of a unified approach to structured discussion at times. Areas identified for improvement included optimising efficiency, structure and handover documentation. Lack of teaching and learning opportunities were also identified. The primary aim was to reduce handover time to 30 min. The secondary aims were to improve communication by introducing the Situation-Background-Assessment-Recommendation (SBAR) tool, improve team satisfaction and introduce a teaching programme in the time saved. The Model for Improvement methodology was used with MDT focus groups and questionnaires to explore change ideas. This informed our ‘Plan, Do, Study, Act’ cycles to design a structured handover. Daily measures looked at handover length and individual team member satisfaction. Weekly measures included semiqualitative questionnaires highlighting areas for improvement. Feedback was gathered from emails and MDT discussions. A structured handover format incorporating SBAR, key task allocation and a shift handover lead was introduced. A regular MDT teaching programme was initiated. Over 4 weeks, ‘Good’ handover ratings increased from 22% to 65%; ‘Poor’ ratings decreased from 25% to 8%. Mean handover time decreased from 47 min to 31.25 min; a decrease of 33.5%. Overall, the team viewed SBAR positively as an efficiency-promoting tool. Structured handover has promoted staff competencies, team morale and information sharing practices among ILAT. MDT teaching improved team communication and confidence. Sustaining motivation to keep up interventions and documentation of handover were identified as key areas for sustained improvement.
- hand-off
- PDSA
- healthcare quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The Integrated Liaison Assessment Team (ILAT) is a liaison psychiatry service at a north London acute hospital which provides services to approximately 500 000 people.1 It serves a diverse range of patients from different socioeconomic backgrounds and ethnicities.
ILAT receives referrals from the emergency department and inpatient wards for patients over 18 years of age where there are mental health concerns. Examples include self-harm, depression/anxiety, psychotic illness and cases are often complicated by substance misuse and social deprivation. Team members have a diverse range of previous experience in community and inpatient mental health services which promotes interdisciplinary working. The multidisciplinary liaison team (MDT) includes nurses, doctors, social workers, assistant health practitioners, managers and administrators. There is an allocated shift lead responsible for coordinating the team.
The morning handover is used to present patients, highlighting relevant background information and risk factors and to help formulate robust management plans. It also generates tasks such as obtaining collateral information or onwards referrals to other services. Summarised patients’ details are written on a whiteboard and regularly updated. An electronic patient record system is used for formalised documentation and reference.
Liaison handover meetings take place twice daily and are recognised as central to safe patient care.
Historically several issues were identified that might impact on the efficiency and quality of MDT handovers. There were no assigned roles for the meeting and individual differences in the level of motivation, engagement and actioning of tasks. Handover was often interrupted by contact from other teams via the pager system. There was difficulty allocating workload fairly across the MDT and ensuring the best use of resources and clinical skills.
We chose to prioritise improving the efficiency of the morning handover as the majority of decision-making processes occurred here. Areas of improvement highlighted by initial team feedback included the length of the meeting (with a consensus that a maximum length of 30 min represented the most efficient use of time), repetition of information and an inconsistent structure.
The project’s aims were:
To reduce handover length to 30 min.
To improve team satisfaction with the handover process.
To improve handover structure by introducing Situation-Background-Assessment-Recommendation (SBAR).
To implement an MDT teaching schedule.
These aims were created through team consultation with an aim to address key concerns and were designed to be achievable in the given time frame (4 weeks). The influence of other factors such as the size and complexity of patient caseload, staffing complement and IT functionality were recognised as impacting on handover meetings that were beyond the scope of this project.
Background
Handover is the process whereby ‘responsibility and accountability for immediate and ongoing care (of patients) is transferred between healthcare professionals’.2 NHS England highlights it as one of the 10 key clinical standards integral to providing a standardised service and as a crucial step for ensuring clinical safety in patient care.3 Clinicians are responsible for ensuring relevant clinical information is communicated to all members of staff involved in patient care.4 Internationally, the WHO has suggested that formalising the process with checklists and rigorous documentation may improve outcomes.5
Handover processes should be formalised and reflected in hospital policy.2 Ideally handover should be led by a competent senior decision maker with attendance across the MDT, in an environment close to the clinical setting. It should be ensured essential information is communicated with electronic documentation recommended.2 3
In practice handover processes can be inconsistent or lacking clear structure. Poor communication can compromise clinical safety and has been identified as a factor in adverse events. Patient satisfaction can also be adversely affected by inadequate communication.6 7 The WHO has prioritised improved communication in handover in its top five patient safety solutions.8 Health professionals across of range of settings and disciplines reported being aware of adverse events where they noticed poor handover was a significant cause.9 Poor communication can lead to missed or delayed diagnoses and treatment.10 11 The language used can lead to negative framing or labelling of a patient with impact on care.6
The SBAR tool, originally developed by the US Military provides a structure to allow concise accurate information to be disseminated across a team, reducing the likelihood of error or confusion.12 SBAR implementation has been shown to have evidence for improved patient safety in the healthcare setting.13 SBAR is the most prevalent communication tool recommended for standardising handover structure in healthcare practice.14 Simulation training using the SBAR tool for psychiatry trainees found it was a useful tool for improving confidence in identifying deteriorating patients, communication and understanding the position/viewpoint of coworkers.15 Improvement in communication was also linked to improvement in junior doctor safety and satisfaction, and in psychiatry-specific settings has been linked to improved satisfaction among nursing staff and doctors.
SBAR was therefore used in this project as a starting point for handover improvement.
The authors note that the literature on nurses’ and doctors’ views regarding handover are often studied separately. However, creating sustainable changes in practice involves changing departmental culture and therefore requires buy-in from the whole team.
Measurements
Baseline data were collected over a week to understand current processes, including handover length. An MDT meeting consisting of nurses, doctors, managers, a social worker and other allied health professionals was held to collect feedback regarding handover.
A semiqualitative questionnaire was handed out at the meeting (see online supplemental appendix 1) ascertaining respondents’ rating of the current handover system and knowledge about the SBAR tool (we wanted to gauge the MDT’s familiarity with SBAR at this stage so that subsequent training would be delivered at an appropriate level). Two additional free text questions gave opportunities for feedback about the positive aspects of the handover systems and suggestions for improvement, respectively.
Supplemental material
To improve team engagement, we used the feedback to create interventions and measurements.
Over the course of a 4week period we collected daily measurements:
Total morning handover time (minutes).
Time taken to assign tasks to the MDT.
Team satisfaction daily using a simplified Likert scale.
Team members ranked whether they found the handover to be ‘Good’ (:)), ‘Average’ (:/) or ‘Poor’ (:() by placing a bead in a pot labelled with the corresponding face. This was a simple, quick method to improve the chance that the team would take part in data collection.
As a balancing measure a weekly semiqualitative questionnaire (see online supplemental appendix 2) was used to collect anonymous team feedback.
Additionally, we collected feedback about the teaching sessions and suggestions for future topics.
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Design
The quality improvement (QI) project was led by two junior doctors supported by the rest of the MDT. The baseline data were collected over 1-week period. Following this, a questionnaire was given out weekly to the team to gather collaborative feedback of improvements. We also gathered feedback about teaching topic ideas.
We developed a driver diagram (figure 1). In this the handover process was broken down into actions, generating a list of change ideas that could then be tested out in Plan, Do, Study, Act (PDSA) cycles, using the Model for Improvement over a 1-month period in October 2019.

Driver diagram. MDT, multidisciplinary liaison team; SBAR, Situation, Background, Assessment, Recommendation.
We tested the PDSA cycles while continuously collecting data (see the Measurements section). This feedback and further steps were discussed at fortnightly multidisciplinary meetings. We created weekly update posters regarding change ideas to be implemented and data collected which were displayed by the handover board.
The ‘Life QI’ web programme16 was used to input data and create figures and graphs. This report was written using the Standards for Quality Improvement Reporting Excellence guidelines.17
As shown in figure 1.
Strategy
PDSA 1: introduction of the SBAR communication tool
The first change idea was to introduce the ‘SBAR’ tool to the MDT. The aim was to improve the quality of information-sharing and handover efficiency. We led an interactive training session where staff practised using the tool. SBAR information posters were displayed in the office.
PDSA 2: shift lead runs handover
The next idea was to assign a specific team member to chair the meeting. We thought this would create a more efficient handover process by assigning individual responsibility for leading the handover. We decided that the shift lead would be appropriate for this role and that they would direct the meeting by standing at the handover whiteboard which meant that there was a visible leader. Their role included: reminding the team to use SBAR, timekeeping, efficient documentation of decisions and focus on agenda items.
PDSA 3: shift lead assigns MDT handover tasks
Originally MDT members would volunteer at the end of handover to do the tasks generated. This meant there was a lack of direction over ownership of tasks and could decrease efficiency of handover. To optimise efficiency, the shift lead was asked to assign tasks to individual team members.
PDSA 4: shift lead numbers patients and assigns to MDT
In order for handover to function smoothly patient notes need to be reviewed prior to the meeting and a summary provided. Historically this had been happening in an inefficient ad hoc manner. The inefficiency may be amplified if staff were unfamiliar with the patient caseload. The electronic notes can also be slow to load when IT systems are functioning suboptimally. To streamline this process prior to the start of handover, the shift lead was given responsibility for numbering the patients on the whiteboard. Each team member present was assigned a corresponding number(s) to retrieve records and present a succinct summary. This ensured equitable contribution to the meeting and minimised disruption by loading patient notes pre-emptively.
PDSA 5: teaching sessions
We used the time saved in handover to start an educational teaching programme within the team. We invited members to sign up to deliver a 10 to 15 min teaching topic. This type of informal MDT teaching programme was something we had both experienced before and a useful style of integrating learning into a busy workplace. Staff value learning as a way to improve personal and professional development and we anticipated that this would also help to build team morale. We also thought it would encourage the team to continue to invest in the handover process if there was a visible positive outcome of their hard work.
Results
Baseline results
The initial week-long audit demonstrated the average handover length was 47 min, 10 min of which was used for task allocation. The areas for improvement from the semiqualitative feedback from the initial group meeting included: the length of handover, time taken to assign tasks and lack of formal structure leading to repetition of information.
Handover length
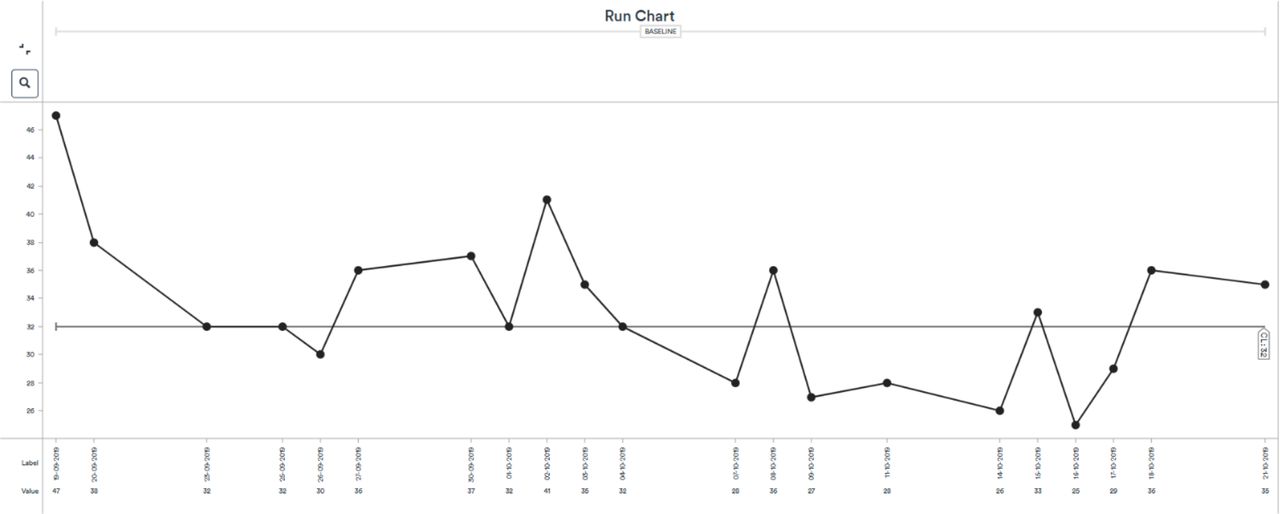
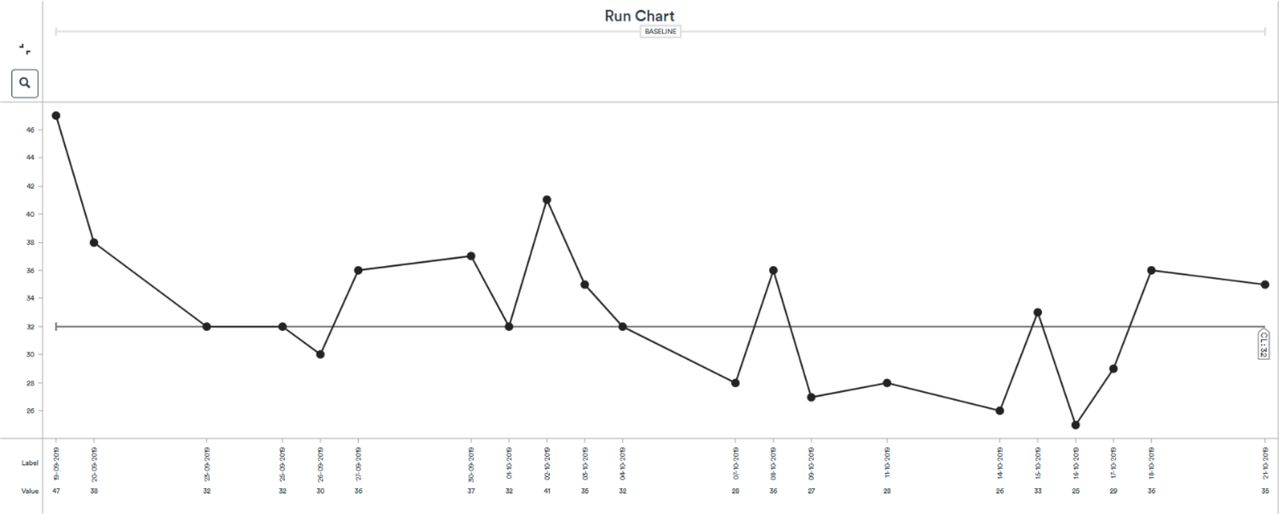
Our data showed that there was an overall decrease in the length of handover over the 4 weeks. After the first week there was a 29% reduction of handover length (from 47 min to 33.4 min).
As shown in figure 2.
{kind=link}
{kind=link}
Run chart demonstrating measured handover times over 1 month.
The mean handover time was reduced from 47 to 31.25 min. In week 3 the mean handover length was less than 30 min which met our first aim. Week 4 showed a slight increase to 31.25 min.
While our initial results are promising, there is insufficient data at present to conclude that a sustained decrease in handover time has been achieved.
Handover satisfaction
From week 1 to week 3, there was an increase from 22% to 65% for handover being rated daily as ‘Good’. ‘Average’ ratings decreased from 52% to 27% and ‘Poor’ ratings decreased from 25% to 8%.
In week 4, we noted poorer engagement with this method of feedback as there was approximately a 50% response rate. While ‘Poor’ ratings decreased to 0%, the number of ‘Good’ responses also decreased.
The majority of the team engaged with filling out semiqualitative questionnaires. Assigning a shift lead to run handover was particularly supported by the team feedback, well adopted and sustained throughout the process.
However, having the shift lead responsible for assigning tasks to the MDT received mainly negative feedback from the shift leads. The shift leads reported this was an inappropriate responsibility because members of the team preferred to have autonomy over their work. This change idea was not adopted by the team as the division of workload was routinely deemed fair and appropriate.
The change idea proposed in PDSA cycle 4 (see the Strategy section) took some time to be fully integrated as it required full commitment from all team members. However, as team members adjusted to the new way of working, they appeared engaged and actively participated in discussions. This was reflected in their subjective feedback of feeling ‘more included’ in decision-making. We also felt this was a good opportunity to practice SBAR.
Situation-Background-Assessment-Recommendation
Overall, qualitative questionnaire feedback demonstrated that SBAR was met positively by the team, with feedback that SBAR enabled a more concise, structured approach which also improved quality of information giving. Some quotes include:
There is support during complex presentations.
The process is considerably more concise and to the point.
SBAR has made handovers more efficient.
We noted that some team members felt that the SBAR format resulted in repetition of clinical information. However, over time as the team familiarised themselves with SBAR it became integrated into handover.
Teaching
The teaching programme was evaluated through team qualitative feedback. Members across the MDT were keen to deliver teaching sessions based on their areas of interest; topics included the acute confusional state, delirium and the dopaminergic pathways. Trainee doctors were able to achieve work place-based assessments of teaching. We found it helpful to initially give guidance around structuring teaching sessions to help encourage team members who had not delivered teaching before. Qualitative feedback included:
The teaching was useful for my day-to-day job.
It is interesting to learn from the others in the team.
I’m keen for the programme to continue.
There was positive feedback for both delivering and receiving teaching and helped a variety of team members to contribute and feel valued. One team member who spoke English as a second language gave feedback that the opportunity to give a teaching session in a non-judgmental space helped her to improve her confidence. This teaching programme continued once the QI project ended.
We found that due to on-call duties, annual leave and sickness it was not always possible to collect the data each day and this resulted in some missing data. This may have affected the sensitivity of change measurement.
Lessons and limitations
On reflection, we felt that there was a good uptake of the SBAR tool and teaching programme. Handover length was reduced and the MDT reported improved confidence and engagement with the teaching.
It was difficult to formally quantify the improvements and sustain these interventions. Additional barriers to change included high staff turnover due to shift working and differing team opinions regarding appropriate interventions.
To address these barriers, we collected feedback as a balancing measure and held meetings regularly to explore change ideas in an ongoing dynamic process acceptable to the department. We liaised with the trust QI team for advice and guidance on data collection and implementing change ideas throughout the project.
We acknowledge that there was a short period of collecting baseline data. However, we had informally assessed handover in the preceding months and after 1 week of collecting handover length believed there was room for significant improvement.
While we regularly liaised with the team and had buy-in from team leaders, consultants and nurses, coproduction could have been encouraged and integrated earlier in the project. Key priorities for the team were identified via their feedback, but to encourage coproduction individuals who generated ideas could have been encouraged to develop their idea and collect data. This would improve sustainability of the project by ensuring more team members were invested in its completion.
Collecting regular semiqualitative feedback from the team was a useful balancing measure to identify any unintended negative impact of the interventions. For example, our interventions placed large emphasis on the shift lead to structure handover and to assign tasks. The wider MDT felt positively about allocating a shift lead. However, the individuals nominated to be shift leads reported this to be a large burden of responsibility. Although background research indicated that a single lead was optimal for handover, this was a large shift in team culture and was perceived to potentially introduce hierarchy. Introducing a change idea that is against the working culture of a department can decrease overall satisfaction, even if it improves one project outcome.
Initially we were unsure about how instigating a teaching programme would be received, however, the feedback was overwhelmingly positive. A diverse range of team members contributed to the programme. The team viewed it as a direct and tangible benefit of improving handover. We also felt that the teaching programme boosted staff morale which had a positive impact on the team and patient interactions.
A limitation of introducing a teaching element was the reluctance of staff to commit to something that might involve preparation outside of working hours which was an additional pressure on top of their clinical work. It may be difficult to sustain as it requires individuals to voluntarily sign up to teach sessions. To address this in the future it would be useful to allocate a teaching coordinator to oversee the sessions and to involve medical students and invite professionals from other teams.
Our measurement scales for assessing team satisfaction were chosen as a quick and accessible way of collecting data, enabling a day-to-day assessment of fluctuations in responses. However, these were not based on pre-existing validated measures.
Factors including patient caseload, staff numbers and IT issues may have influenced the length of handover independently of any change interventions. However, this is reflective of day-to-day clinical practice and despite these variables we demonstrated an overall reduction in handover length and improvement in satisfaction.
To expand the project, we would like to have peer support worker input as well as service user involvement by collecting qualitative data regarding how prioritisation of their care and their experiences of the service could be improved. Indirect cost savings may include increasing time available for patient contact. The next steps would also be to improve documentation of key MDT decisions that are made at handover. Currently new information technology including an electronic whiteboard is being introduced to the team.
To sustain positive changes in the future, the updates to the handover process and team satisfaction will be made a standing agenda to the fortnightly team meeting. To prevent the project from stagnating, a QI champion was appointed within the team to continue driving the project and to reaudit it. Integration of MDT colleagues as QI leads could also increase team engagement.
Other means of maintaining and developing this work includes incorporating guidance in to training packs for new starters, reviewing other liaison teams’ handover processes and promoting a flexible and tailored approach to making further changes.
To explore if the positive changes are truly sustainable, data will need to be collected over a longer timeframe. The length of the project was limited by our time in post however the project was handed over to colleagues for continuation.
The results and conclusions have proved to be similar to other liaison teams and we feel that the lessons learnt may be of use to future projects not only within a broader psychiatric setting but in an acute hospital setting.
Conclusion
There is robust evidence that optimising handover is integral to clinical care and safety. It should be a formalised process that is kept as brief as possible. This project aimed to integrate these principles into a liaison psychiatry team by addressing the specific challenges encountered. We used principles from the background research alongside MDT feedback to develop a dynamic and individualised handover.
In terms of our primary project aim we demonstrated an overall decrease in handover time. By week 3 we had reached our aim although this rose marginally to 31.25 min. We identified various factors that are part of everyday clinical work that may have contributed to this. We acknowledge that further data collection and ongoing work to maintain the reduced handover length is needed.
We used SBAR to introduce a formal handover structure and introduced a teaching programme which received positive MDT feedback. Overall, our results are encouraging and support the idea that a robust and structured handover process, which optimises efficiency and communication, is generally a well-received change to support safe clinical care and containment in a dynamic liaison team. Our project has been presented at a trust QI forum, with a view to replicate this model in other teams.
We learnt that as handover is a multidisciplinary process, driving sustainable change in practice required investment from several different stakeholders. We consulted with nurses, allied health professionals and doctors at different levels to help inform different areas that could impact on handover. Equitable leadership and participation are essential to encourage team participation and to enhance learning and confidence.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. This was a quality improvement project conducted with verbal and written consent of team members. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the Whittington ILAT for their input and time with sustaining the project.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @KirtanaVallabh1
Contributors KV and JH contributed equally to this paper. KV is acting as guarantor for the paper. KV and JH designed project, implemented changes, collected data, conducted data analysis, manuscript production. LD: consultant of liaison team; active contributor to data and feedback for PDSA cycles, reviewed manuscript. FJ reviewed manuscript.
Funding Open access membership through ‘The Health Foundation-Q’; verification code: 0571246253.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.