Article Text

Abstract
Background Patients in remote communities who risk premature delivery require transfer to a tertiary care centre for obstetric and neonatal care. Following stabilisation, many patients are candidates for outpatient management but cannot be discharged to their home communities due to lack of neonatal intensive care unit (ICU) support.
Problem Without outpatient accommodation proximal to neonatal ICU, these patients face prolonged hospitalisation—an expensive option with medical, social and psychological consequences. Therefore, we sought to establish an alternative accommodation for out-of-town stable antepartum patients.
Methods Quality Improvement approaches were used to identify process strengths and opportunities for improvement on the antepartum ward in a tertiary care centre. Physician and patient surveys informed outpatient accommodation programme development by a multidisciplinary team. The intervention was implemented using a plan–do–study–act cycle. Barriers to patient discharge and enrolment in the programme were analysed by completing thematic and strengths–weaknesses–opportunities–threats (SWOT) analysis.
Results Physicians broadly supported safe outpatient management, whereas patients were hesitant to leave the hospital even when physicians assured safety. Our alternative accommodation was pre-existing and cost-effective, however, we encountered significant barriers. The physical space limited family visits and social interaction, lacked desired amenities,and the programme proved inconvenient to patients. The thematic and SWOT analysis identified aspects of the intervention which can be optimised to develop future actionable strategies.
Conclusion The utilisation of acute care beds is costly for the healthcare system and must be allocated judiciously. Patient needs, experience and health system barriers need to be considered when establishing alternative outpatient accommodations and strategies for stable antepartum patients.
- maternal health services
- quality improvement
- length of stay
- patient satisfaction
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Patients with adverse obstetrical complications from remote communities may require medical transfer for obstetrical care due to the risk of premature delivery. Following stabilisation, many patients are suitable for safe discharge and outpatient management. However, patients must maintain close proximity to the hospital, often a tertiary level, due to the ongoing risk of urgent premature delivery.1–4 In the absence of financial support for hotels or local accommodation provided by family or friends, patients from remote communities cannot be safely discharged and therefore remain hospitalised.
Prolonged unnecessary hospital admissions are a significant problem. Admission to an acute care bed is costly for the healthcare system and should be used efficiently to prioritise those with the highest need. When all antepartum beds are occupied, patients requiring admission remain in the labour and delivery assessment ward until a bed becomes available. Therefore, prolonged admission of stable antepartum patients results in reduced capacity of the assessment ward and thus longer patient wait times, impacting patient flow in the system. Furthermore, patients admitted to the hospital are prone to frequent laboratory investigations, many of which may not be undertaken as an outpatient, resulting in unnecessary costs and potential iatrogenic harm.5 A study looking at quality of life of hospitalised versus outpatient preterm pregnant women found that hospitalised women scored significantly lower in subjective comfort and all domains of health-related quality of life.6 Prolonged admissions may lead to decreased quality of life for patients because of reduced sleep quality, disruption of daily routines, unnecessary monitoring, social isolation and feelings of implicit confinement to the hospital.7 Importantly, outpatient management of preterm labour is not associated with increased major adverse maternal or perinatal outcomes compared with inpatient management.8 In fact, one study found that outpatient management of preterm labour was associated with a lower incidence of preterm delivery, as well as fewer admissions to neonatal intensive care unit (NICU) and higher birth weight among neonates.9 These findings suggest that outpatient management of those at risk of premature delivery has the potential to benefit patients and neonates, and may optimise healthcare resource allocation and hospital patient flow.
Available knowledge
The Lois Hole Hospital in the Royal Alexandra Hospital (RAH) is an obstetrical tertiary referral centre located in Edmonton, Alberta, Canada. Over 7500 deliveries occur at the centre annually, and it has a large catchment area including northern Alberta, northern British Columbia and the Northwest Territories. Following stabilisation, out-of-town antepartum patients may be eligible for outpatient management but must remain close to the Lois Hole Hospital. In Edmonton, Larga House provides accommodation for indigenous patients with treaty status, but no comparable programme is available for other antepartum patients. Since the cost of privately arranged accommodation is prohibitive for most, the majority of out-of-town stable antepartum patients remain in hospital for a prolonged admission.
Successful models for outpatient accommodation, such as Ronald McDonald House, Easter Seals House and Larga House, are typically funded by private donations, hospital foundations or government programmes. In the absence of comparable funding, a low-cost intervention was developed using existing infrastructure at our hospital to provide outpatient accommodation and support responsible use of limited healthcare resources.
Specific aims
We sought to develop an outpatient accommodation programme for out-of-town stable antepartum patients. We aimed to reduce out-of-town antepartum admissions longer than 1 week due to threatened preterm labour, preterm premature rupture of membranes (PPROM), short cervix and cervical incompetence by 50%. Secondary aims were to maintain or improve patient experience compared with inpatient management and avoid out-of-hospital births.
Context
The intervention targeted out-of-town patients admitted to the 26-bed antepartum ward. Baseline obstetrical and admission data from 2016, including data on length-of-stay, were collected from the Alberta Perinatal Health Programme (APHP), a provincial obstetrical database.
Quality Improvement (QI) tools (process mapping and a cause-and-effect diagram) were completed to identify barriers to discharge of stable antepartum patients at our site. We developed an alternative outpatient accommodation programme with the input of a multidisciplinary team of social workers, attending physicians, residents, unit nurses, unit clerks, Antenatal Home Care (ANHC) nurses, a QI consultant, a patient care manager, a spiritual care provider and administrative staff. QI methods revealed four salient intervention themes to be considered for programme development: infrastructure, care team, referral process and check in/out process.
Intervention
Infrastructure
The NICU Boarder Rooms are a pre-existing outpatient facility located near the RAH, connected by pedways and tunnels, that provides accommodation to mothers of infants in the NICU. The facility contains 17 individual dormitory-style rooms and 2 family suites, as well as a communal kitchen, living space, activity room and laundry. The facility is not staffed by healthcare workers, and occupants live independently. This shared space has a high uptake by the NICU mothers, but the available number of rooms is much greater than the need, leading to frequent vacancies. Due to availability, ease of access and low upfront cost, the NICU Boarder Rooms were chosen as a pilot alternative accommodation facility. The facility administrators allocated two rooms to this programme, to which minor improvements were made to enhance the appearance and function. Hospital and community social events were made available to the programme participants. However, visitors such as spouses and family were not allowed in the facility due to pre-existing facility regulations. Many out-of-town patients travel independently and visitors often find hotel accommodation, therefore, we anticipated that these regulations would not significantly impact our target population. Instead, hospital public spaces were recommended to programme participants for visitation when needed.
Care team
We sought to replicate the typical outpatient community management provided to Edmonton antepartum patients, which consisted of routine visits by ANHC nurses and appointments with their obstetrician. Hospital social workers coordinated discharge from hospital to the boarder room facility and provided facility orientation. Patients were responsible for their day to day needs although information regarding grocery delivery and community supports were provided. Hospital security was available for patient safety and assistance navigating the hospital as needed. Additionally, ANHC nurses were provided with an examination room located in the neighbouring room from the participant rooms to perform routine fetal and obstetrical monitoring. Standard Operating Procedures were created to inform and guide the relevant healthcare providers supporting this antepartum boarder room programme.
Referral process
Physicians were made aware of programme launch through email and obstetrics grand rounds presentations. Patients were eligible for the boarder room programme if outpatient management was recommended by their attending hospital physician, if they fulfilled ANHC intake criteria and if they lived at least 30 min from hospital (online supplemental appendix A). Antepartum ward charge nurses were trained to identify and flag eligible patients, and referral forms were completed by physicians and sent to the social work department for further screening. A member from the social work team provided a case-by-case assessment to determine suitability for the programme. A tracking system was developed to review and log all referrals. The assigned social worker provided eligible patients with a boarder room facility information package, tour of the facility, and obtained written consent on boarder room entry and hospital discharge.
Supplemental material
Check-in/out process
A formalised process overseen by the social work team was developed for participant check-in and check-out. Participants were followed until giving birth at the RAH or discharged to their home community by their physician. Preintervention surveys were distributed to antepartum inpatients and RAH obstetricians to gauge interest in, and perceived need for, a safe outpatient accommodation programme. Patients were surveyed on their psychosocial well-being using original and validated tools.10 Postintervention participant experience surveys were developed to measure the following parameters: participant demographics, participant–provider communication, functionality of accommodations, accessibility, safety and experience. The authors reviewed patient records for all patients referred to the programme.
Study of the intervention
The Donabedian conceptual evaluation framework was employed to evaluate the efficacy of the intervention through a set of measures, including process, outcome and balancing measures.11 The Model for Improvement guided this QI project, which involved plan–do-study–act (PDSA) cycles, allowing for continuous innovation, evaluation and improvement. We planned to complete two PDSA cycles. PDSA cycle #1 involved recruiting a small number of participants with the goal of gathering feedback from participants and healthcare staff to address any unforeseen issues of the intervention. PDSA cycle #2 involved recruiting a larger number of participants to assess whether the intervention reduced out-of-town antepartum admissions on our unit.
Measures
The selected process measures were: number of stable antepartum patients at our site who are eligible for the boarder room programme, and number of participants who successfully completed the boarder room programme. The outcome measures were to reduce out-of-town antenatal admissions longer than 1 week due to PPROM or cervical conditions, increase discharge on our antepartum unit, ensure participant experience stays the same or improves as compared with those staying on the antepartum unit, and decrease unnecessary medical interventions for this patient population. Our balancing measure was that no out-of-hospital births would occur among programme participants.
Analysis
Descriptive analyses such as percentages, mean, median and range were performed. Qualitative analyses were performed on inpatient surveys and multidisciplinary team members’ feedback where themes were extracted and coded. A strengths–weaknesses–opportunities–threats (SWOT) analysis identified improvement strategies for future interventions.12
Ethical considerations
A pRoject Ethics Community Consensus Initiative risk screening tool was applied that indicated programme was QI with minimal ethical risk, therefore, no formal research ethics was sought.13 Patients or members of the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Baseline measurement
APHP data revealed that 1186 patients were admitted to the RAH in 2016 with the diagnoses of threatened preterm labour, PPROM, short cervix and cervical incompetence (figure 1). These diagnoses were selected as they were felt to be the most representative of stable patients suitable for outpatient management. Of these patients, 133 were admitted for >7 days, with a mean of 21 days and total 2823 bed-days. This accounted for 55.1% of cumulative bed-days for all patients admitted due to prematurity (figure 1). Forty-eight per cent were from out-of-town, of whom 73% (46/53) eventually delivered at RAH, 22% (14/63) in their home communities, and the remaining 5% (3/63) at other hospitals in Edmonton. This points to a significant problem where a very small proportion of stable patients, many of whom are from out-of-town, have extended admissions to acute care beds which could be allocated elsewhere.
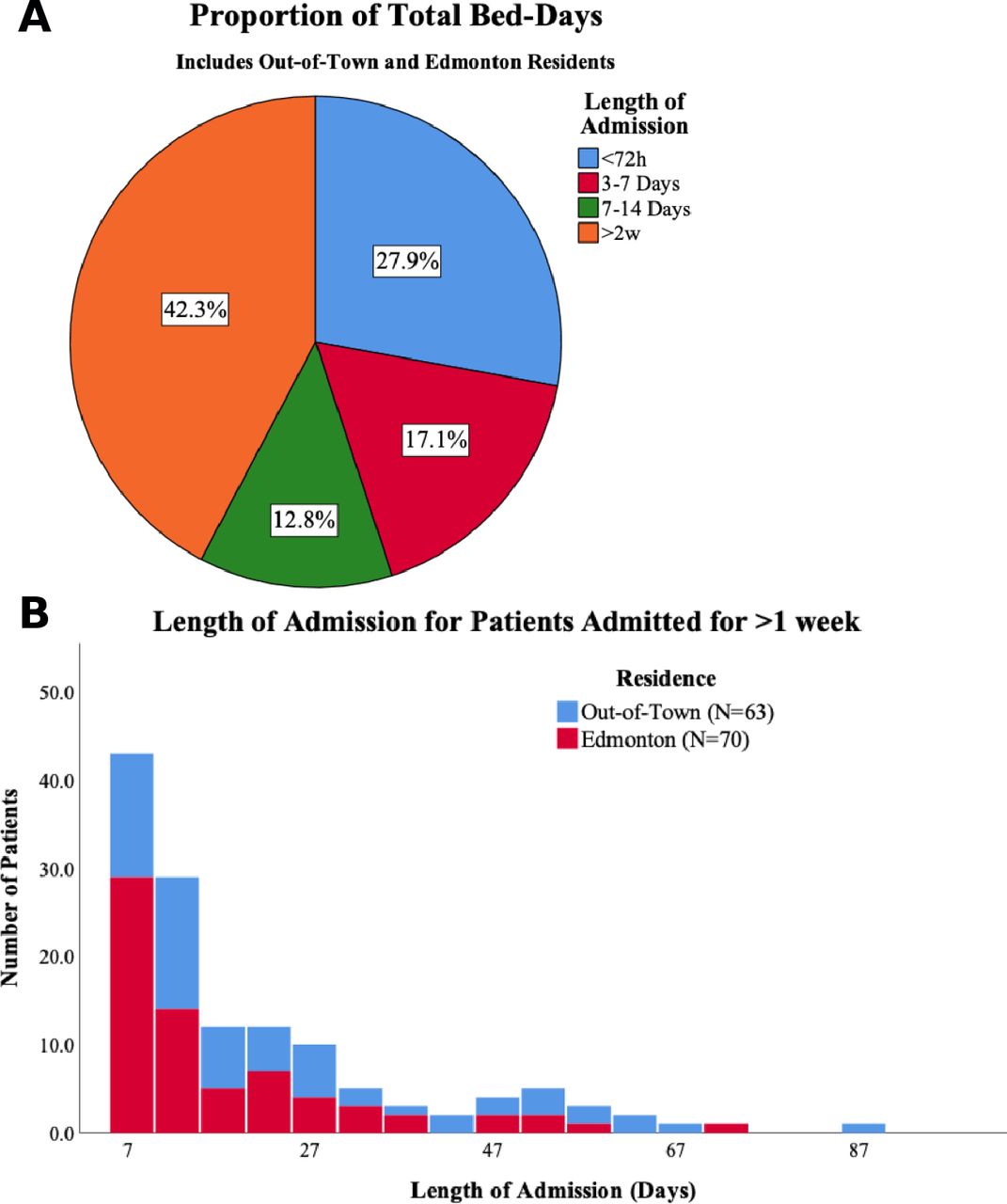
(A) Pie chart of patient length of stay as a proportion of antepartum ward total bed-days and (B) histogram of length of stay for long-term (>7 days) antepartum patients from Edmonton and out-of-town.
Readiness survey
A physician specific preintervention survey was distributed to all obstetricians at the RAH. All (13/13) respondents identified the need for an antepartum outpatient accommodation facility and would refer patients to a programme. Within the past year, respondents had admitted patients who would have otherwise been suitable for outpatient management had they not been from out-of-town (12/13), and all (13/13) had managed patients from hotels, or Larga House for indigenous obstetrical patients. Respondents indicated that the decision for outpatient management was influenced by Maternal Fetal Medicine recommendation (12/13), symptoms (12/13), patient social situation (11/13) and ANHC criteria (10/13).
A patient specific preintervention survey was distributed to 17 long-term antepartum patients (mean 22.5 days, range 7–58 days). Eight patients were from out-of-town. Most patients (82.4%) would have preferred outpatient management if deemed safe by their physician. Nine of seventeen (9/17) patients felt at least moderately depressed or anxious, while 6 of 17 had significant (somewhat to extremely disturbed) sleep disturbance. Seven patients felt at least somewhat socially isolated. Despite this, most (13/17) were satisfied or very satisfied by their inpatient status and described feeling reassured by frequent fetal assessments.
PDSA cycle #1
The first programme enrolment, PDSA cycle #1, started on 28 October 2019, with the aim of discharging two clinically stable antepartum patients to the Boarder Room Programme. Eight patients were referred to the programme, and one patient agreed to be enrolled. However, she immediately left for home, and later told social work that she was feeling depressed in the space. The first PDSA concluded shortly thereafter in June 2020, and PDSA cycle #2 was not pursued due to no uptake of the intervention. Of the seven patients who were referred to the programme but declined, their cumulative inpatient stay accounted for a total of 91 avoidable bed-days.
Following PDSA cycle #1, barriers to programme enrolment and discharge were gathered from both referred patients and the multidisciplinary team. A thematic analysis of textual data identified barriers were related to: the facility characteristics (boarder rooms), the care team, the health system and the patient (figure 2).

Barriers to discharge stable antepartum patients from hospital to boarder room programme.
Barriers
While the facility was conveniently located and at no cost for patients, several facility factors were barriers to programme success. The boarder rooms are located in an ageing building with outdated features and amenities that require costly renovations. Centralised temperature control, inoperable windows, shared bathrooms and limited kitchen facilities further diminished appeal. The space was largely vacant during the daytime, which reduced opportunity for socialisation. In contrast, the inpatient antepartum ward is modern and comfortable, meals are provided, and there is ample opportunity for socialisation from both staff and patient visitors. Further, the boarder room building operating hours restricted the freedom of patients to come and go as they desired. While these limitations were acceptable to mothers with infants in the NICU, who spent little time in the facility, the limitations proved to be isolating and restrictive to antepartum patients.
Hospital care teams identified practice norms as a barrier to timely discharge. Team members noted that hospital culture is permissive of long-term admission, and the minimal pressure to discharge patients made it challenging to advocate for enrolment to the boarder room programme. In addition, comfort with outpatient management is provider-dependent and may impact the decision to refer to an unfamiliar programme.
Health system barriers included limited programme funding available to renovate the boarder rooms, as well as a lack of clear clinical guidelines to support clinicians in outpatient management of high-risk pregnancies.
Patient-related barriers were those identified by patients. Patients expressed hesitancy to outpatient management due to perceiving inpatient care as safer than outpatient, despite reassurance of safety by their care team. In addition, pre-existing policies did not permit visitors in the boarder room facility, which posed a more significant challenge for recruitment than previously anticipated. In contrast, inpatient rooms often had pull-out beds for visiting partners. Patients communicated the need to permit visitors and co-occupants, similar to other programmes such as Larga House and Easter Seals House. Ultimately, while our intervention sought to improve patient autonomy, it also demanded self-sufficiency. Patients were responsible for meal preparation, grocery delivery, discretionary transportation, and other activities of independent living. The burden of these additional responsibilities further diminished its appeal and was a considerable barrier to patients considering enrolment in the boarder room programme.
Summary
Using QI methodology, an outpatient accommodation programme was developed and implemented to reduce extended admissions of stable antepartum patients from remote areas. Patients and staff broadly supported outpatient management; however, due to barriers related to the facility characteristics, care team, health system and patient, the intervention was unsuccessful. In PDSA #1, eight patients were found to be eligible for the Boarder Room Programme, and one agreed to participate in the intervention, but shortly returned to hospital. Although our intervention was unsuccessful, feedback from referred patients and the multidisciplinary care team after PDSA #1 revealed important barriers to programme enrolment. As mentioned, these barriers were related to the facility characteristics (limited social opportunity, poor functionality and aesthetics compared with hospital), the care team (limited pressure to discharge, differences in provider practice), the healthcare system (limited funding, no clear outpatient management guidelines), and the patient (restricted visitation, preference for inpatient care, requirement for self-sufficiency).
Interpretation
Despite most patients in the readiness surveys indicating a desire for outpatient management, our proposed intervention was unsuccessful. This was mainly due to infrastructure and partly the referral process. The other two components of the intervention, namely care team and check in/out process seemed to work fine, as we were able to enrol a participant into the programme.
The dormitory style accommodation, older building, shared facilities and visitor restrictions overshadowed the proximity of the facility, aimed to allow more independence and self-sufficiency. The infrastructure and visitation policy are drawbacks that other successful outpatient accommodations in Canada, such as Larga House and Easter Seals House, do not have. This points to an important lesson that cost should not be a driving factor when designing an outpatient accommodation model (as this was a low cost development with no funding), and what works for postpartum mothers may not necessarily work for antepartum women. Social isolation was a key reason for our participant to leave the facility within a short time, highlighting the need to support the mental health of those from remote communities who may be at higher risk of feeling isolated. Similarly, having access from family members to the accommodation is another important consideration in designing an outpatient facility. This was cited by many of the eligible patients who chose not to be discharged to the facility.
The referral process to the outpatient accommodation was also unsuccessful as many patients who met the discharge criteria were not identified by the clinician. Only eight patients were referred to the outpatient accommodation over 8 months, whereas a much higher number of patients were anticipated to be eligible. Some providers were not familiar with the programme, although there were several attempts to provide education and a tour of the facility. The work-around in our process was that our charge nurse identified eligible patients for physicians, and the social worker discussed enrolment in the programme. As mentioned, there seems to be a sense of permissiveness to keep these patients in hospital, which may not be the case at other sites. In this study, the cumulative inpatient stay of the patients who were referred to the programme but declined was 91 bed-days. We anticipate that the actual number of eligible patients and their associated hospital stays is much larger than this estimate, due to issues with the intervention referral process. These bed-days represent an opportunity cost, where other patients in need may have had to wait for a bed or could not be admitted as a result of bed shortage. Ultimately, the outpatient management of this patient population could also redistribute acute care beds to other units which have increased bed demands.
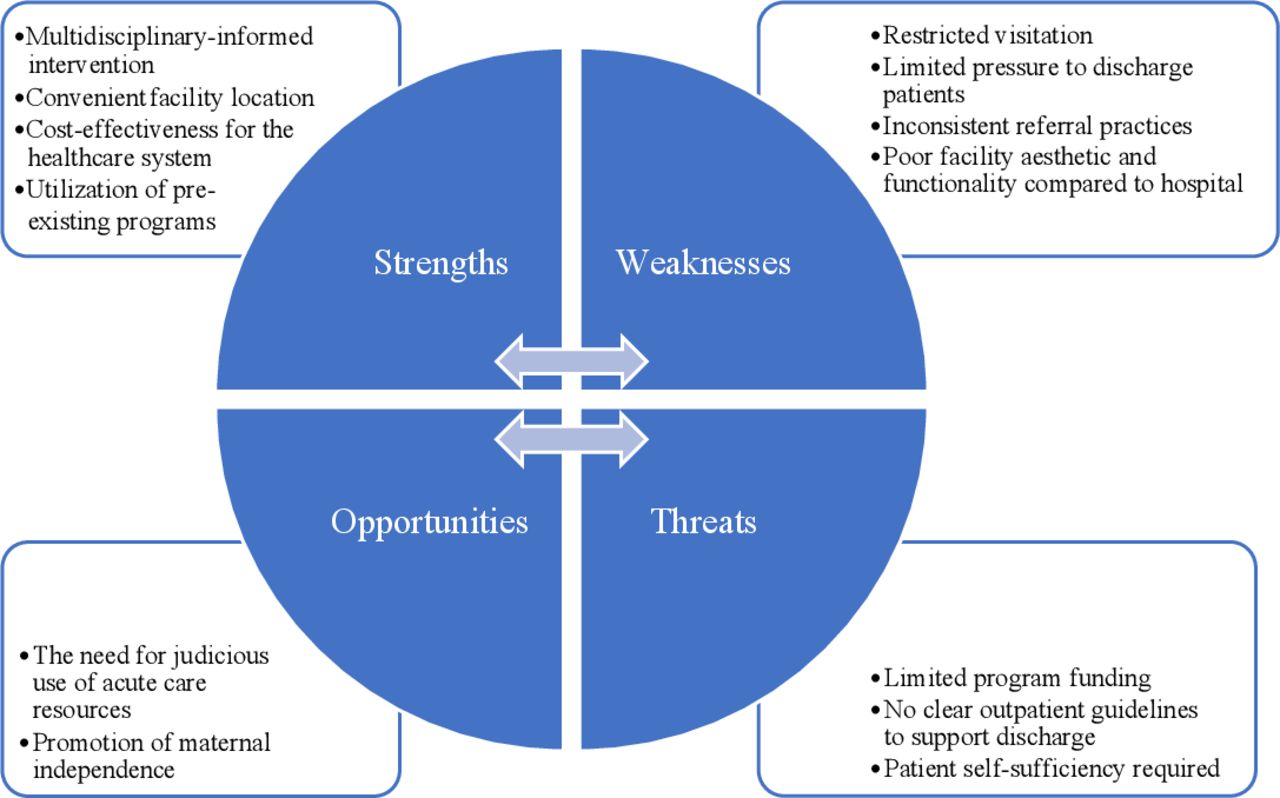
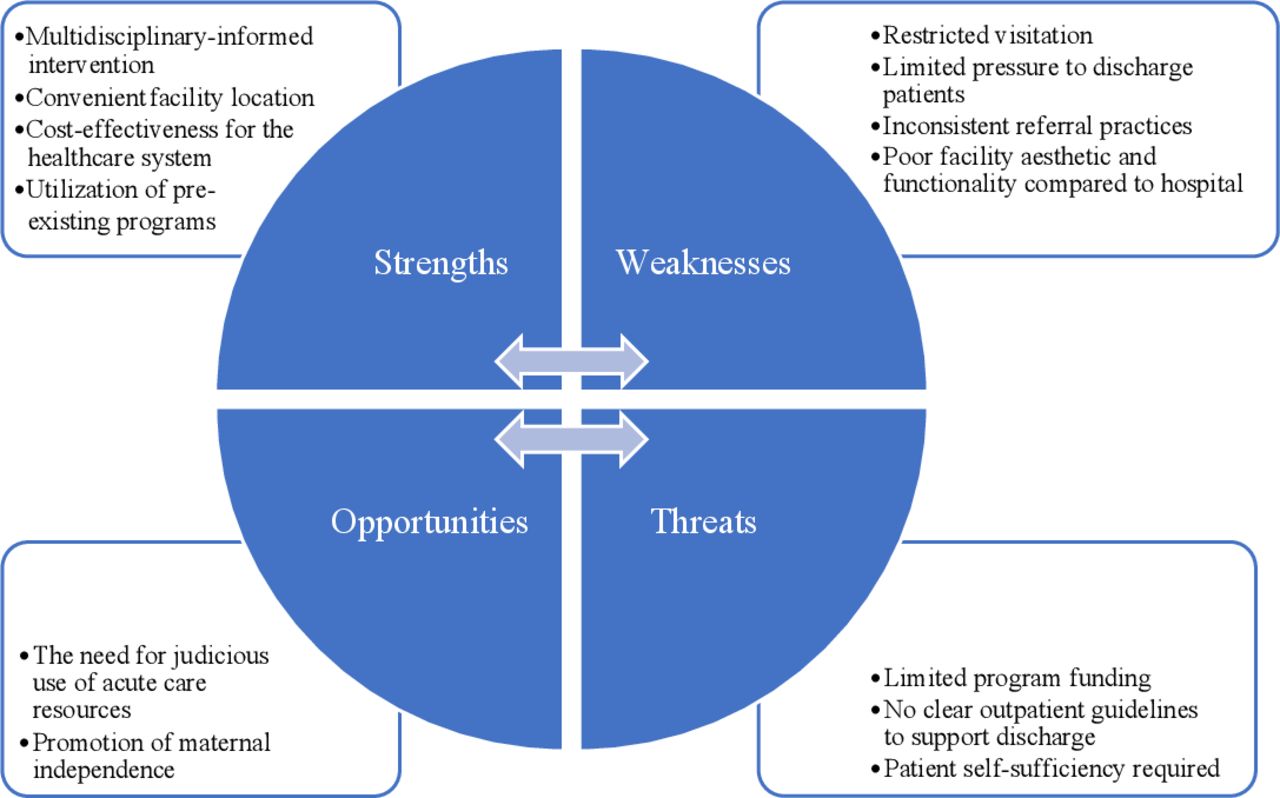
A SWOT analysis identified actionable strategies that may promote a successful future intervention (figure 3). The barriers of the intervention previously discussed in this study comprise the weaknesses and threats of the SWOT analysis. Strengths and opportunities are characteristics which may support the success of future interventions.
{kind=link}
{kind=link}
{kind=link}
Strengths-weaknesses-opportunities-threats (SWOT) analysis. Strengths and weaknesses are internal factors that may be controlled, while opportunities and threats are external forces that may not be controlled.
Strengths of the programme included convenient facility location, cost-effectiveness for the healthcare system, a multidisciplinary-informed intervention and utilisation of pre-existing programmes. Partnership with Antenatal Homecare informed an intervention that emulated outpatient management of Edmonton-based patients. Social work played a critical central role as the point of contact for patients, care team, and the research team. The social work team bridged the transition between inpatient and outpatient management, which is key to success in any similar intervention.
Weaknesses included visitor restrictions per boarder room facility policy, practice norms in which there is limited pressure to discharge patients, inconsistent physician referral practices, as well as boarder room aesthetics and functionality. Patients desire a safe, family friendly and modern accommodation. Actionable strategies were explored to meet the patient’s expectations in future interventions, such as using hotel accommodation, partnership with existing outpatient facilities or construction of a new accommodation space. While this intervention was straightforward to implement due to low upfront costs and an existing facility, resolving the barriers identified may require a large capital expenditure. Leveraging relationships with medical leadership and health economics professionals will validate these needs.
Opportunities include the need for judicious use of acute care resources, and promotion of maternal independence. Ultimately, the patient’s preferred length of stay should be incorporated into care planning, but must also be weighed against the demand of acute care beds and known risk of iatrogenic harm with prolonged admission. Any future intervention must seek to maintain or improve patient experience compared with inpatient management.
Threats included limited programme funding, no clear guidelines for safe outpatient management to support physician decision making and the requirement for patient self-sufficiency. There exists the need to develop clear clinical practice guidelines to support outpatient management, not only of our target population, but all stable obstetrical patients. Such guidelines would serve to improve care team and patient comfort with outpatient management and empower physicians to prioritise timely discharge. While supporting outpatient management could save valuable healthcare resources, it is important to consider the increased financial burden on patients. Supports such as gift-cards, care packages, recreation discounts and transportation passes may help patients transition to an outpatient accommodation.
Limitations
This study has several limitations beyond the weaknesses and threats identified by the SWOT analysis. As previously discussed, cost was a significant driving factor when designing the study, which likely led to insufficient consideration of potential barriers. Factors like cost of self care and facility visitor restrictions were more deterring than anticipated. These barriers may have been mitigated by early consultation with a patient representative in the design of the intervention and with patient feedback gathered sequentially in the planning process.
There are other perspectives which in retrospect could have had a meaningful contribution to the current study. Larga House is an Edmonton-based organisation that provides accommodation for Indigenous individuals travelling from remote areas to receive care. However, we did not consider that some individuals in our target population are indigenous but do not have treaty status, and are therefore ineligible for this resource. For this reason, since our vast Northern catchment area is home to many indigenous communities, it would have been culturally appropriate to consult elders from these communities in designing the intervention.
Lastly, while our intervention targets out-of-town patients, whose geography is a single factor requiring prolonged admission, it cannot be ignored that a large portion of prolonged admissions are of patients residing in Edmonton (figure 1B). We believe that the root cause of prolonged admission in these patients is due to multifactorial biopsychosocial factors, and that further research is necessary to elucidate these root causes and develop a targeted intervention.
Conclusions
Acute care beds are a valuable healthcare resource that must be allocated judiciously. In this project we attempted to implement a programme of alternative accommodation that would meet the needs of antepartum patients and the healthcare team, while reducing the burden on acute care beds. While our outpatient accommodation model was unsuccessful to entice eligible out-of-town stable antepartum patients to stay, many valuable lessons were learnt to inform future intervention planning.
This work has implications for hospital administrators given the high demand of acute care beds in a public healthcare system. This work also has implications for obstetricians, who bear the responsibility of discharging patients. Ultimately, the sustainability of this work depends on the ability of hospital nurses and social workers to devote time to this project, and the capacity of ANHC nurses to support more outpatients.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
A pRoject Ethics Community Consensus Initiative (ARECCI) risk screening tool was applied that indicated program was QI with minimal ethical risk, therefore, no formal research ethics was sought.
Acknowledgments
We thank the RAH Antepartum and NICU units, the Antenatal Homecare programme, the Lois Hole Hospital Women’s Society, and the Lois Hole Hospital Department of Obstetrics and Gynaecology.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors WWS is the corresponding author and designed and conducted the study, analysed the results and created the manuscript. WWS is the guarantor and accepts full responsibility for this work. MBS helped design and conduct the study, analyse the results and create the manuscript. AR helped design and conduct the study, analyse the results and create the manuscript. PM helped design and conduct the study, analyse the results and create the manuscript. MG helped design and conduct the study, analyse the results and create the manuscript. TL helped design and conduct the study, analyse the results and create the manuscript. ATT helped design and conduct the study, analyse and revise the manuscript. KKB helped design and conduct the study, analyse the results and revise the manuscript. RR helped design and conduct the study, analyse the results and revise the manuscript.
Funding This work was supported by the quality improvement innovation fund Alberta Health Services, Medical Affairs, and the Office of the Chief Medical Officer (CMO) for the Edmonton Zone. They did not influence the design, implementation or reporting.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.