Article Text

Abstract
The COVID-19 global pandemic dictated rapid change to outpatient services within our London-based maternity hospital. Coupled with long waiting times in the Consultant-led Antenatal clinic, we aimed to reduce hospital footfall and unnecessary contact with a clinically vulnerable patient population by reducing face-to-face consultations. Numerous specialties have already successfully implemented safe and effective teleconferencing, allowing remote review while reducing the risks posed by face-to-face contact. A target to see at least 15% of women remotely was set to reduce footfall in the Consultant-led Antenatal Clinic. We aimed to reduce face-to-face waiting times to a mean of 30 min. In March 2020, clinics were prevetted by the clinic consultant to carefully select appropriate women suitable for video or telephone consultations. Clinic templates were changed, increasing appointment times by 5–25 min each. ‘AccuRx’ software was tested and used to communicate appointment details and conduct the consultation. In-person waiting times in the clinic and number of virtual consultations over a 3-month period was recorded, along with qualitative feedback from service users and staff through surveys and departmental meetings. Mean waiting times were reduced by 33% from 45–30 min and multiple service-user benefits were noted, including partner involvement, convenience of waiting for appointments at home and removing requirement for childcare. However, limitations of internet connectivity, need for time to prevet clinics and lack of a robust administration system to inform women of their appointment type were highlighted. Further work is required in these areas to ensure sustainability and improvement of this process for the future.
- COVID-19
- quality improvement
- telemedicine
- maternal health services
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The COVID-19, global viral pandemic created a sudden pressure on healthcare services in the UK from March 2020. Vital, non-elective maternity services could not cease operations and had to adapt rapidly. While long waiting times in the Consultant-led Antenatal clinic had previously been highlighted as a problem through patient surveys and previous quality improvement work, the issue was seen to be multifactorial and complex. No previous attempts at improvement were successful. The COVID-19 response demanded a rapid change in practices throughout the antenatal pathway. Changes were put in place to reduce the number of face-to-face antenatal hospital visits required and to introduce telephone consultations.
On 16 March 2020, the UK government announced the following recommendations:
Pregnant women should stay at home and minimise contact with non-household members (‘shielding’).
People with pre-existing medical conditions should also consider shielding (after advice from occupational health).
All households with one or more symptomatic members (fever or continuous cough) should stay at home (‘self-isolate’) for 14 days.1
Many staff members were having to self-isolate or shield even if they were themselves well and asymptomatic of COVID-19. Considerable anxiety and confusion were generated among the patient population, with many women raising queries with regards to their antenatal appointments, whether they could attend with a partner, and how to self-isolate while ensuring their pregnancy care was unaffected.
Rationale
Many of our consultant-led clinic attendances are midwifery referrals for early medication review or due to risk factors necessitating a personalised schedule of antenatal care. Appointments occurring in the first or second trimesters, or in-between routine midwifery visits where a physical examination had been performed do not necessitate a clinical examination according to National Institute of Clinical Excellence (NICE)E standards for Antenatal Care and can be done remotely.2 It was hypothesised we could safely reduce the number of women entering hospital unnecessarily during the pandemic period so long as patient selection was cautious.
If consultation time for patients seen remotely was less than face-to-face, this would then minimise the waiting time for patients that required physical clinical attendance.
Specific aims
Reduce footfall in the Consultant-led Antenatal Clinic by seeing suitable patients remotely, reducing crowding in clinic waiting areas and enabling social distancing. The target set by outpatient transformation was to see 15% of patients remotely.
Reduce waiting times for patients who require face-to-face consultation to an average of 30 min from the appointment time.
Context
As part of the COVID-19 pandemic response, measures to reduce patients and visitors attending the hospital were rapidly implemented by the hospital trust:
Visiting restrictions for inpatients.
Restrictions on accompanying partners to ultrasound scans and outpatient appointments.
Working with hospital pharmacies to enable remote outpatient prescribing.
The antenatal pathway was altered to reflect the reduced schedule of routine visits, as seen in online supplemental appendix 1.
Supplemental material
Background
General practice and primary care are undergoing a technological revolution as the UK government has advised all primary care providers to have the provision of video consultations for patients.3 The British Medical Association now provides advice following this government legislation allowing doctors, not only in primary care but in hospitals also, to arrange equipment to be able to work remotely, as well as guide on when to consult patients via video.4
There are several challenges to setting up video consultations quickly. Patient selection is key—the population must be selected with chronic or stable conditions.5 Managing patients with acute and serious illnesses in this way is not appropriate. With this, from a clinician perspective, concerns have been raised regarding the quality of clinical care, training of clinicians, ensuring patients can use the software, as well as privacy and safety.6–8
As these challenges are overcome, preliminary data from this sudden change in practice are beginning to be published. A collaboration between Stanmore and Southampton published data from the Royal National Orthopaedic Hospital following a change in practice, reducing face to face consultations from 93% to 13% over 6 weeks with high patient satisfaction.9 In patients that require surgery or attend for a delivery of their baby, prehospital or admission COVID-19 screening is essential.10
Data from numerous medical specialties including psychiatry and mental health, dentistry, ophthalmology, obstetrics and gynaecology, endocrinology, neurology, dermatology and urology have now been published, which all highlight adaptation techniques for teleconferencing to be performed safely, efficiently and successfully.11–18 These publications focus on patient groups and provide insight on methods of safely triaging and when patients are required to be seen face to face, in order to limit exposure and protect those at higher risk of morbidity or death from COVID-19.
As practice is now adapting safely, high-quality online teleconferencing platforms are increasingly available to use. Between clinicians, Microsoft Teams is a safe platform now used across the National Health Service, enabling confidential information to be discussed remotely.19 For patient consultations, platforms are now available for both primary and secondary care, including AccuRx, Attend Anywhere, LIVI, Doctorlink, eConsult, EMIS Online, Engage Consult, Ask NHS and Visiba Care.20 21
Validated technology is now available to continue the process of exploring its role in 21st century healthcare. Although this has been prompted by the coronavirus pandemic, this is the perfect opportunity to see how outpatient maternity care can evolve in a way beneficial to both women and clinicians.
Measurement
Outcome
Waiting time for women attending in-person (time from appointment to being seen)—there was no electronic process for recording the time seen by the clinician, neither could we use the time between check-in and check-out as a proxy measure for length of stay in the clinic, as the administration staff did the patient check-out in batches. We defined waiting time as time between the scheduled appointment and when the electronic patient record was started by the clinician, as it is normal practice for clinicians to do this at the beginning of the consultation.
Process
Number of consultations done virtually per clinic—this was collected manually through reading the electronic patient record.
Balancing
Staff acceptability of the change was assessed qualitatively through feedback collected via forums such as Consultant meetings and Junior Doctors’ meetings.
Staff and women were involved in codesign of changes via the weekly Antenatal Big Room, which is an open multidisciplinary meeting held on Microsoft Teams during the pandemic and were able to feedback in real time as changes were being tested.22 23
Women’s acceptability of the change was assessed qualitatively through an electronic survey detailed in online supplemental appendix 2, which was sent to all women who attended remote appointments in March–June 2020 via text message, as well as through seven virtual ‘listening events’ held over Zoom in September–November 2020. Listening events used the format of a ‘Conversation Cafe’ to encourage equal contribution of participants to open questions such as ‘How has COVID affected your pregnancy and birth journey?’ and ‘What did you like? What could be improved?’ Conversation Cafe is a structure for facilitated discussion.24
Supplemental material
Design
Interventions
Clinic template change
Each appointment lasted 25 min rather than 20 min. We also built in administration time at the start and end of each clinic. The clinic template change preceded the COVID-19 pandemic, following data collected on consultation time in July 2019. The new clinic template was live by March 2020.
Prevetting of clinics
Consultants vetted their antenatal clinics from 13 March 2020 by reading the electronic patient record the week prior to each clinic and communicating to the woman to stay at home to await a telephone consultation or to attend in-person.
Telephone consultation
Telephone consultation commenced on 16 March 2020.
Video consultation
Video consultation was tested on 23 March 2020 using the platform Attend Anywhere. On 25 March 2020 the platform AccuRx was tested. A written framework for AccuRx and a demo video were made available to midwives and doctors prior to the publication of the ‘COVID Standard Operating Procedure’ on 26 March 2020. Video consultation for patients using AccuRx began on 31 March 2020.
Ethical considerations
At the start of the COVID-19 pandemic, ‘Gold command’ in line with Emergency Planning protocols were put in place and our service was told to implement telephone clinics overnight without any feasibility study or patient and public involvement. Our team assembled itself to study the effects of this change using Quality Improvement (QI) methodology. Using Plan-Do-Study-Act (PDSA) cycles we were able to rapidly address the staff and patient concerns that became apparent. No formal ethics review was required and there was no conflict of interest identified.
Strategy
We used Plan-Do-Study-Act cycles to assess the interventions and scale appropriately. These steps are summarised in online supplemental file 1.
Supplemental material
Results
Figure 1 presents the percentage of appointments performed virtually (via video and telephone) in the Consultant-led Antenatal Clinic by clinic date, demonstrating an increase of 44.9% in virtual consultations from the baseline in March 2020.

Percentage of appointments performed virtually in the Consultant-led Antenatal Clinic by date.
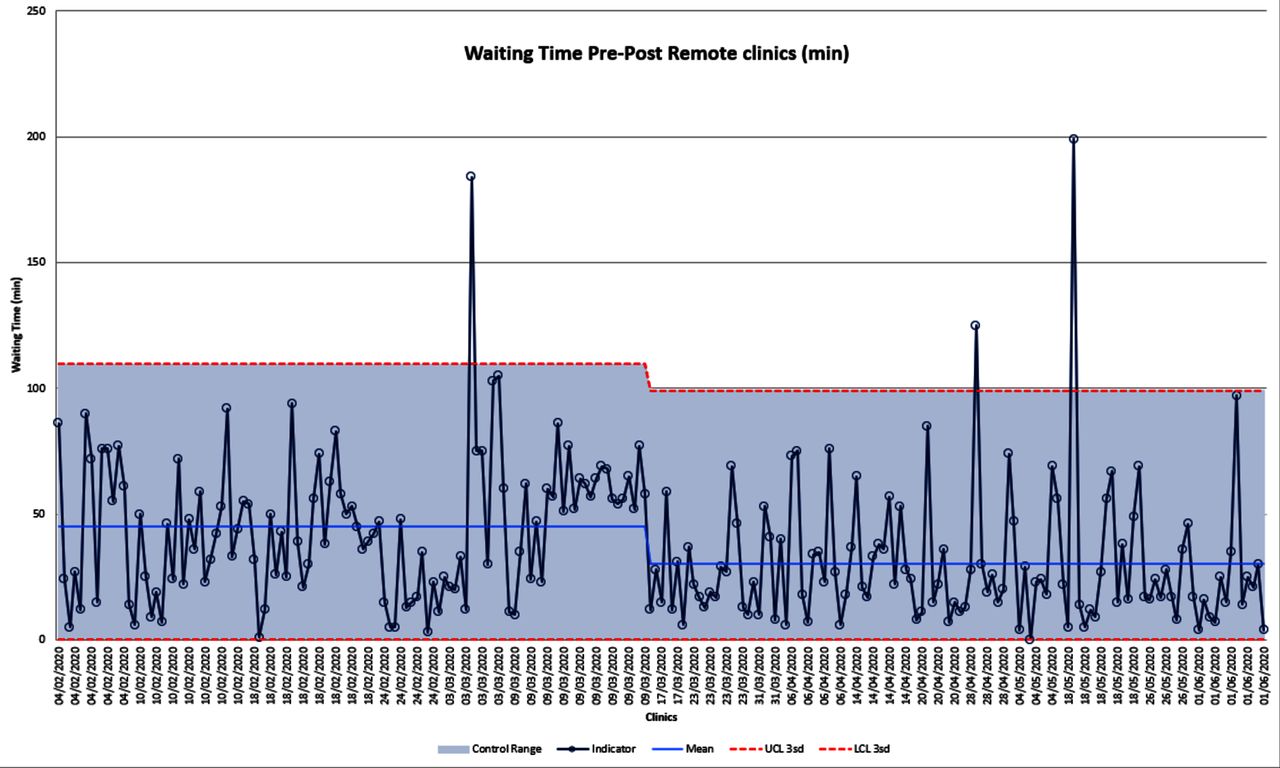
The statistical process control chart seen in figure 2 represents the face-to-face clinic waiting time in minutes. We conducted baseline measurements from 4 February 2020. After introduction of remote consultations, mean waiting times reduced from 45 to 30 min (a reduction of 33%). Efficiencies in clinic consultation time were achieved because the women selected for remote consultation did not require any examination and the time was used purely on counselling or explanation of results and management plans. In contrast, the traditional model of in-person consultation created an expectation of a full antenatal physical examination with every attendance, when this may not be necessary if already performed in the preceding 2–4 weeks by a midwife or other healthcare professional.
{kind=link}
{kind=link}
Waiting times for face-to-face appointments in the Consultant-led Antenatal Clinic by date. UCL 3sd, Upper Control Limit 3rd standard deviation; LCL 3sd, Lower Control Limit 3rd standard deviation.
Points above the upper control limits were investigated. These were women who had checked-in for their appointments but then left the department to have ultrasound scans prior to their clinic consultation, artificially inflating their waiting times.

Significant benefits were noted from service users, in particular the convenience of waiting for appointments at home and notably removing the need for childcare, as highlighted by multiple patients. Many considered the virtual consultations to be part of the routine antenatal appointment schedule and as valuable as a face-to-face consultation. Clinicians also particularly valued the ease of communicating virtually in order to provide a quick update to women on their test results, along with the opportunity to involve members of the multidisciplinary team in order to provide holistic care to women. The majority of pregnant women are from a generation that is familiar with the use of smart phone and video calling technology. Also, while many women were able to work from home during the pandemic, awaiting a video call from the clinic suited their home and work situations, where a longer waiting time while at working at home did not feel inefficient to the woman.
Positive feedback from women for remote consultations included
No need to arrange childcare for appointments.
Partners were able to attend appointments.
Waiting time was spent in the comfort of home, where time was not felt to be wasted.
 Where internet connectivity was good for video, the consultation was of high quality, with good interpersonal connection allowing the discussion of sensitive issues.
Where internet connectivity was good for video, the consultation was of high quality, with good interpersonal connection allowing the discussion of sensitive issues.
Positive feedback from clinicians included
Ability to facilitate multidisciplinary consultations easily with video, where another clinician such as a midwife could also attend remotely
Ability to bring women back to clinic for a ‘quick chat’ or to discuss blood results, as a remote clinic does not impose on patient time and commitments as much as face-to-face.
Less pressure in the clinic as there are fewer women in the waiting room, and a feeling that a long waiting time is more acceptable if the woman is at home.
Remote consultations were not appropriate for all women, however. One woman was deaf and relied on lip reading. While she was engaged in the video consultation, she gave up halfway and became upset as the lag time made it impossible for her to lip read. For women with safeguarding concerns, psychosocial issues, or those for whom English was not their first language, a face-to-face consultation was preferred by both patients and clinicians, in view of the loss of some non-verbal communication during remote consultations. During our listening events, we learnt that some women felt frustrated at being forced to adhere to these numerous restrictions in their pregnancy care, and the provision of remote consultation was put together with the limitations on the number of birth partners, restriction in visiting hours and provision of partners to stay overnight and so on. Where they live, access to transportation to the hospital, and personal preferences are all factors that could influence a woman’s preference for the in-person experience over the potential convenience of remote consultation.
Negative feedback from women for remote consultations included
Poor internet connectivity resulting in frozen screens or difficulty hearing.
Having to wait to be contacted rather than adhering to a specific time.
Being rushed during the consultation by the clinician.
The telephone clinics did not feel like a ‘real’ appointment.
Confusion with the preappointment communication system, especially initially when non-clinical administrative staff were instructed to phone each patient to tell them to stay at home for their appointments.
A feeling of loneliness during the entire pandemic, where they did not have regular physical contact with a clinician apart from ultrasound scans and blood tests until the third trimester.
Negative feedback from clinicians included
Inability to access a translator to join a video call.
Frustration with women sometimes not being ready to take the video consultation, or taking the consultation in a public place, which then impacts on the quality of the consultation.
Not enough administrative time and no robust system for preclinic vetting to take place, which in the current process is crucial to facilitate effective remote consultation.
Phoning women by the administrative staff was time consuming and often ineffective in communicating the appointment details to the woman.
Loss of non-verbal communication in telephone and video consultations where internet connectivity issues created a lag.
Summary of results
Virtual consultations, via the use of video or telephone, can be introduced to the Consultant-led Antenatal Clinic, reducing clinic footfall and potential exposure to COVID-19. Patients were selected based on suitability for remote review and NICE guidance was followed to maintain patient safety. Such a vetting process could easily be adopted by clinicians at other sites or in other specialties. The use of ‘Accurx’ facilitated the implementation of clinician–patient remote consultation.
These changes tackled a longstanding problem of delayed clinics by reducing face-to-face waiting times by one third. Positive remote service user feedback, including convenience for childcare, ease of having a quick update with a clinician regarding something minor and the possibility of involving other members of the multidisciplinary team who may not be in the same location, reinforces the aim of maintaining and improving such a service. Most importantly, through our listening events, we learnt that the selection of suitable women was key in achieving an overall positive experience.
There are many factors outside of the medical history, such as access to technology and reliable internet, the home or work environment (availability of a private space in which to have the consultation), language and other communication needs that will determine whether a woman would benefit from remote consultations. Certainly, during the pandemic the risk versus benefit ratio may be tipped in favour of remote consultation, as women are able to avoid potential exposure to the COVID-19 virus. However moving forwards, we have found that we should not lose the lessons learnt in the potential benefits of delivering an antenatal clinic service remotely for suitable women. The system we have worked out currently is largely dependent on the consultant obstetrician’s clinical judgement from looking through the electronic patient record regarding suitability. Ideally, women would be able to have a choice in their preference for video or telephone or in-person appointments for each visit.
Lessons and limitations
While the COVID-19 pandemic provided a ‘burning platform’ for the adoption of remote consultation, the rapid implementation, initially through top-down structures, meant that high levels of compliance were soon met with low levels of engagement. Furthermore, the lack of ability to meet as a team to discuss and troubleshoot problems meant that a longer term strategy and vision for remote consultations was not present from the beginning.
Our qualitative and quantitative data shows:
Remote consultation by video (using telephone as a back-up option in cases of technical failure) is possible and is largely well received by women.
Staff notice tangible benefits in more organised clinics with shorter waiting times for women.
The 15% target for conducting clinic appointments remotely is achievable.
Our numerical data collection is hampered by the lack of an automatic process for recording the times women are called to be seen, and business intelligence units are so stretched that any requests to pull data from the electronic patient record have been denied. We had to rely on manual data collection, which means we only have data across 3 months.
The consultant prevetting process is required to accomplish the use of remote consultations and probably plays a large role in the efficiency of the clinic and reduction of waiting times, as does the adoption of remote consultations. A substantial part of the work is done outside the clinic, such as reading the electronic patient record and creating a draft management plan. Hence, the reduction in clinic waiting time cannot entirely be attributed to introduction of virtual consultations, but by a combination of factors; including changing the clinic template, essential preclinic preparation and initiating video and telephone consultations.
Our qualitative data, however, are robust, with feedback from 60 to 70 women via surveys and listening sessions and ongoing verbal feedback from staff at departmental meetings.
The main limitation of this intervention is the reliance on individual consultants to carry out preclinic vetting and sending text messages to women. Many consultants criticise this aspect of the process as it takes time and this administration is not adequately job planned. With the lack of an automated process, it is likely our process will only be adopted by motivated consultants who find that the benefits of using the AccuRx platform to contact women and conduct video calls outweigh the extra investment in time.
There is a risk of consultant burnout as the process is so reliant on individuals who have to prevet in advance, whether they are on leave or not.
Conclusion
Our use of PDSA cycles and QI methodology to measure and test strategies to implement telephone and video consultation has meant that we have a strong case to support the use of remote consulting in the antenatal clinic setting. Our experiences have uncovered unanticipated benefits, including a reduced waiting time and improved facilitation of multidisciplinary consultation for complex birth planning discussions.
The main limitation with our current approach is with our ability to sustain and spread the improvement. If we were to overcome the challenge of lack of a robust and accurate automatic process for communicating appointment type to women (remote or in-person), we may be able to ensure more consultant clinics can benefit from remote consultation in appropriate cases. In any longer term, postpandemic iteration of delivery of remote consultation in the antenatal clinic, consideration will have to be given to the woman’s preference in how she is being seen.
Ethics statements
Patient consent for publication
Ethics approval
This project was conducted as a quality improvement project during the COVID-19 pandemic under Imperial College Healthcare Trust Gold command. Ethical approval was not required. exempted this study. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are very grateful for the collaborative work of the members of the weekly Antenatal Big Room.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drsabrinadas
Contributors SD, AC and the Antenatal Big Room members designed the quality improvement project. CRT, CK and SD implemented the clinic changes and carried out the data collection and they also drafted the manuscript. IE performed data analysis and produced the graphs, along with AC. SD is the study guarantor and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. All authors contributed to the interim drafts and reviewed the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.