Article Text

Abstract
In paediatric patients with acute gastroenteritis (AGE), ondansetron use decreases the need for intravenous fluids, reduces hospitalisations and shortens illness duration. Oral rehydration is also known to have excellent outcomes for mild to moderate dehydration secondary to AGE. Although these interventions are recommended in guidelines from international professional societies, baseline data at our clinic showed that <2% of these patients were offered ondansetron, and that few patients received appropriately detailed rehydration instructions. Therefore, we engaged residents and fellows as teachers and leaders in our university clinic’s quality improvement programme to promote evidence-based practice for paediatric AGE. Our gap analysis identified opportunities for interventions including educating paediatricians and paediatrics residents on the safety and utility of the medication. We created standardised oral rehydration after-visit instructions and implemented a trainee-led educational approach that encouraged appropriate medication use. We used a follow-up survey to uncover provider concerns and tailor future interventions. The process metrics included: proportion of paediatric patients appropriately treated with ondansetron (goal of 80%), and proportion of patients given appropriate oral rehydration instructions. The outcome metric was 7-day representation rates. To achieve sustainability, we restructured our process to have senior residents take ownership of teaching and data collection. Trainee-driven interventions increased ondansetron prescription rates to a median of 66.6%. Patients prescribed ondansetron were less likely to represent to care, although representation rate was low overall. Postintervention data suggests that prescription rates decreased without continued interventions and additional systems redesign may help sustain impact.
- Ambulatory care
- Continuous quality improvement
- Education
- Evidence-Based Practice
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
We conducted our project at an acute care clinic at the University of California San Francisco Benioff Children’s Hospital. The clinic has approximately 35 000 total annual visits (9000 acute care visits; 26 000 primary care visits). The patients’ average age is 8 years old and 51.6% are male. About 78% of patients identify as non-Hispanic, and 36% identify as white. Approximately 32% have public insurance— which includes MediCal, Child Health and Disability Programme, Indian Health Services—or are uninsured/underinsured. Most patients (75%) report English as their preferred language, with the two other prevalent languages being Spanish and Chinese (Mandarin or Cantonese). Twelve general paediatrics faculty staff the clinic and supervise trainees.
The problem we sought to address was the lack of adherence to treatment guidelines for paediatric acute gastroenteritis (AGE), which recommend the use of ondansetron and stress the importance of oral rehydration.1 Undertreatment of AGE can lead to emergency department presentation and overall higher utilisation of medical resources and costs to families.2 Preliminary data at our clinic revealed that general paediatricians prescribed ondansetron in 1.5% of eligible patients with AGE from January 2016 to July 2018. Additionally, most patients received non-specific free-texted or prepopulated after-visit rehydration instructions that lacked key details such as fluid amounts, appropriate options for rehydration solutions, or timing of rehydration. We sought to improve patient care by increasing adherence to published recommendations through physician education, standardisation of workflow and appropriate caregiver guidance. Through recurring provider training, we aimed to increase provider acceptance of the role and safety of ondansetron in the care of paediatric AGE.
Our process measures were:
To increase ondansetron use from a baseline of <2% to 80% of eligible patients within one academic year.
Implement the use of standardised oral rehydration instructions.
As our patient-centred outcome metric, we tracked 7- day representation rates to evaluate the efficacy of our process measures.
Background
Paediatric AGE represents a significant healthcare burden, including 1.5 million office visits, 200 000 hospitalisations and 300 deaths annually in the USA.3 Mild to moderate dehydration is a common sequelae optimally addressed through oral rehydration therapy.4 Ondansetron, a 5-hydroxytryptamine-3-serotonin antagonist, is effective at improving the success of oral rehydration and can be a safe and effective component of AGE therapy.5–9 It decreases vomiting, the need for intravenous fluid resuscitation, and hospitalisations for AGE.3 6 It has an excellent safety profile, with no attributed mortality, and only rare dysrhythmias in patients with congenital long QT syndrome, with no clinical examples since the 32 mg intravenous dosage was discontinued.6 10 In paediatric emergency department trials, intravenous ondansetron did not cause QTc prolongation on serial ECGs taken up to 1-hour postadministration.11 Given the extreme rarity of significant adverse events, joint guidelines published by the European Society for Paediatric Gastroenterology Hepatology and Nutrition and the European Society for Paediatric Infectious Diseases encourage prescribing a short course of the medication.1 Previous studies conducted in emergency departments show improved outcomes in line with our aims of ondansetron use. Retrospective studies in paediatric patients with AGE found a decrease in return visits and shorter length of visit2 12 associated with increased ondansetron use. A recent meta-analysis further supports the use of ondansetron in paediatric AGE, reinforcing ondansetron’s benefits of decreasing use of intravenous rehydration, duration of nausea/emesis, and need for hospitalisation.13 Rutman et al4 implemented a clinical pathway emphasising oral rehydration and ondansetron for paediatric AGE and showed sustained decrease in intravenous fluid use and length of emergency room stay.4 Additionally, an economic analysis estimated an annual savings of US$65 000 000 in the USA based on routine administration of oral ondansetron to eligible paediatric patients with gastroenteritis-associated vomiting or dehydration.5
Measurement
Population
The target population included paediatric patients (age 1–18 years old) seen at an outpatient clinic for AGE. The study population was paediatric patients with AGE who were treated at our acute care clinic during the study period (1 August 2018–30 June 2019). Diagnoses of AGE were based on International Classification of Disease, 10th Edition code,14 and were confirmed by manual chart review. Patients below 1 year of age, or with congenital cardiac diseases, history of arrhythmias, chronic diarrhoea, chronic nausea, ondansetron allergies or comorbid conditions that make a definitive diagnosis of AGE difficult were excluded.
Data collection
Paediatric residents (n=4) collected the data. Prior to starting data collection, these residents received a 1-hour training on the diagnosis and treatment of paediatric AGE to ensure a shared baseline knowledge base. Data were collected monthly from the electronic health record system (EHR).
Every month, a medical record analyst extracted a list of patients seen at the clinic for an International Classification of Disease, 10th Edition coded diagnosis of gastroenteritis, nausea, emesis or diarrhoea. To maximise sensitivity of this initial screen, we used a variety of codes associated with gastroenteritis symptoms. Residents then manually reviewed each encounter to determine whether the case was consistent with AGE. For each visit, we extracted: patient age, gender, date of service, provider name, ondansetron prescription (yes/no) and type of after-visit instructions used (standardised gastroenteritis after-visit instructions, free text or other prepopulated instructions). For the patient outcome measure, residents collected data on representation to care within 7 days for continued or worsening symptoms. These data included the site of representation (primary care clinic, acute care clinic, emergency room) and whether it led to hospitalisation for dehydration from AGE. Residents used a standardised data-capture form that was stored on the university’s secure Research Electronic Data Capture server.15
Data analysis
To establish a preintervention baseline, a retrospective chart review from January 2016 to July 2018 was conducted to evaluate the proportion of paediatric patients with AGE who were prescribed ondansetron by physicians at our acute care clinic. During the intervention period, ondansetron prescription rates, the proportion of patients who received appropriate oral rehydration instructions and representation rates were calculated monthly. We opted to report the representation rate over the entire academic year due to limited sample size.
Baseline assessment
Our preintervention retrospective chart review revealed that the baseline rate of ondansetron prescription for eligible patients with AGE was 1.5% (n=426) over the two-and-a-half years prior to our project. We conducted a preliminary gap analysis to identify primary drivers for change and used an A3 template to describe the problem. The initial gap analysis involved a meeting with seven General Paediatricians at the clinic, where five of them reported rarely using ondansetron. Identified areas of change included: lack of provider awareness of the treatment recommendations, parental and provider concerns about ondansetron safety, and after-visit instructions with insufficient guidance. Preliminary key drivers included: (1) physician knowledge and (2) parent understanding and acceptance of medical intervention. The obstacles identified in this opening meeting were used to develop a follow-up anonymous survey to assess whether the original provider concerns persisted.
Through a multi-layered approach—attending physician education, peer-led resident education, standardised after-visit instructions and provider surveys—we involved stakeholders and integrated their feedback to facilitate practice change.16 17
Design
The core project team consisted of paediatric gastroenterology physicians who oversaw the development of the educational interventions, Quality Improvement Leadership from the Department of Paediatrics who provided a framework for trainees to lead QI work,18 and Paediatric Gastroenterology fellows and Paediatric residents who spearheaded project implementation. We partnered with general Paediatricians at the acute care clinic to better understand workflow and barriers to implementing change. Patients were not involved in the design of this project.
We implemented quarterly Plan-Do-Study-Act cycles to address each barrier identified in our initial gap analysis. The interventions focused on an education-based approach, incorporating plants to modify interventions based on feedback from stakeholders. We anticipated that a singular attending-level educational session would be insufficient to achieve sustained impact. Therefore, monthly teaching responsibilities were transitioned to senior residents as a structured component of their acute care rotation. To further a systems redesign, we also developed standardised after-visit instructions that underwent iterative improvement through user feedback. Table 1 shows the timing of our interventions.
Intervention timeline
Strategy
Intervention 1
An hour-long education session for attending paediatricians was developed and delivered by a paediatric gastroenterology Fellow. Information presented included an outline of AGE treatment guidelines and data on the efficacy and safety of ondansetron. We hypothesised that improving provider guideline acceptance and comfort with counselling parents would increase ondansetron use. We had planned to repeat the faculty education session quarterly, but due to scheduling constraints from stakeholders, the providers were only able to repeat it once at the 8 month time point.
Intervention 2
Based on a hypothesis that engaging residents would promote further improvement and sustainability, we created a teaching role for fellows and senior residents to better align the clinic’s practice with AGE treatment guidelines. This second intervention involved monthly 1 hour resident education sessions that shared guideline knowledge with residents rotating through the clinic. This intervention had fewer scheduling conflicts as trainee schedules were well synchronised with scheduled lecture times, allowing for monthly education sessions. The monthly format enabled rotating residents to participate in an education session during their 4 weeks acute care rotation. Paediatric gastroenterology fellows initially led these sessions and subsequently trained clinic-based paediatrics residents (n=6) to take ownership of the peer-lead education. Elevating the role of the senior resident functioned as a systems redesign that we hypothesised would promote sustainable outcomes. Peer teaching re-enforces the teacher’s medical knowledge, which lends itself to improved adherence of best practices.19 20
Intervention 3
We created standardised evidence-based patient instructions for home ondansetron use and oral rehydration therapy (ORT) recommendations to ease the burden of documentation and support caregivers in following treatment guidelines. Previous literature highlights the benefit of these instructions in increasing medication compliance.21 The instructions underwent multiple revisions throughout the intervention period, guided by user feedback. Revisions made the instructions shorter and easier to reference for families, particularly those with lower health literacy. The instructions included: appropriate fluid choices for ORT, recommended amounts and rates of fluid intake, instructions on ondansetron use, and return precautions. The instructions were disseminated to all front-line providers via our EHR, and it was the physician’s responsibility to select and use the new instruction set. Notably, these instructions were only available in English.
Intervention 4
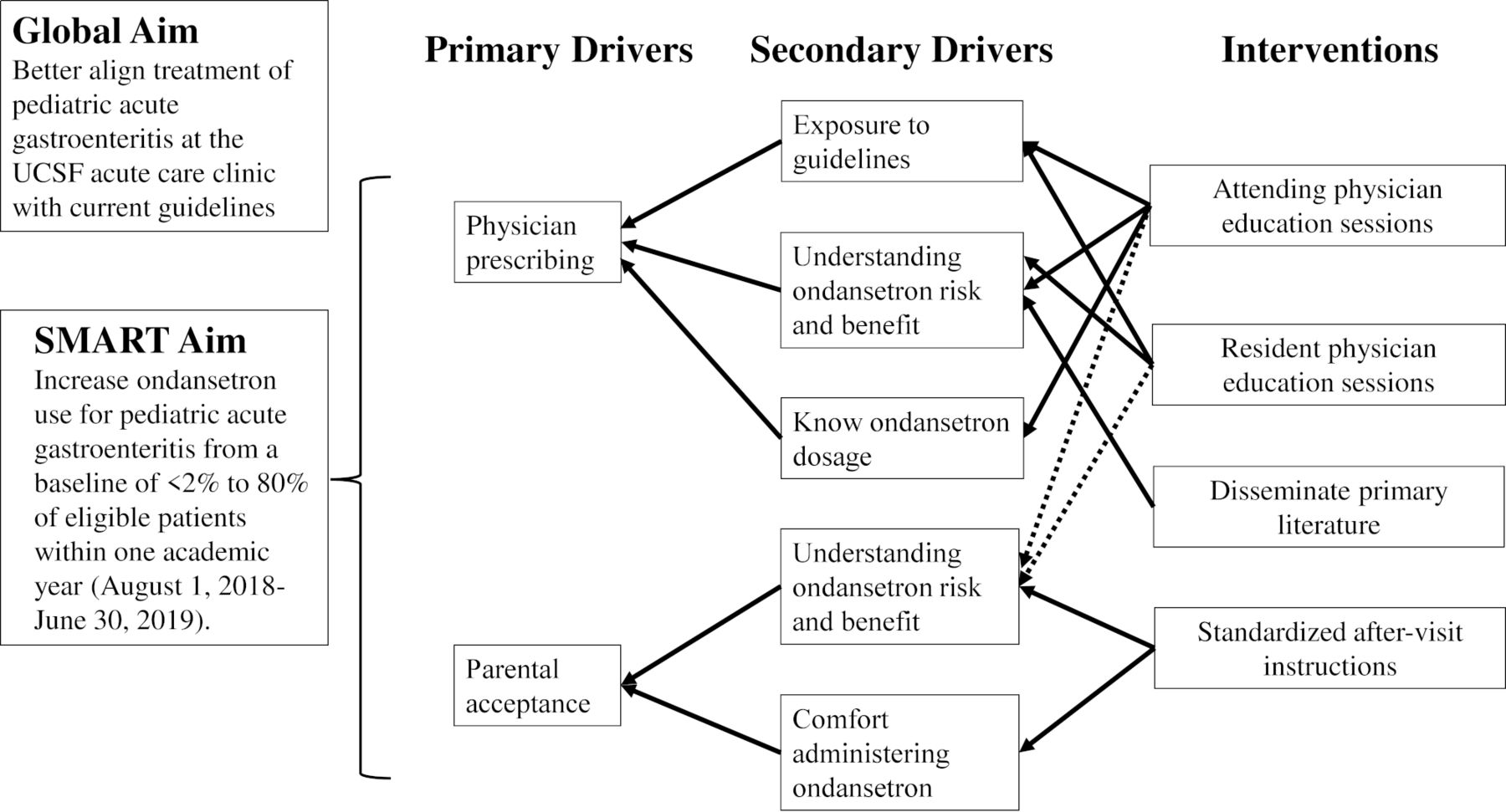
At the 8-month mark, we conducted an anonymous survey of attending paediatricians regarding their initial concerns, including their perspectives on the risks of using ondansetron, their comfort with prescribing the medication, and any additional barriers to use. Our goal was to identify whether their initial concerns persisted and to use the results to develop future interventions that specifically address provider concerns. Through this survey, we identified concerns regarding the potential for ondansetron to mask alternative diagnoses, specifically appendicitis. In response, we disseminated paediatric literature showing that ondansetron use for suspected gastroenteritis does not mask serious diagnoses.22 Additionally, our training materials were adjusted to address this concern. We revised our key driver diagram (figure 1) to include this intervention.
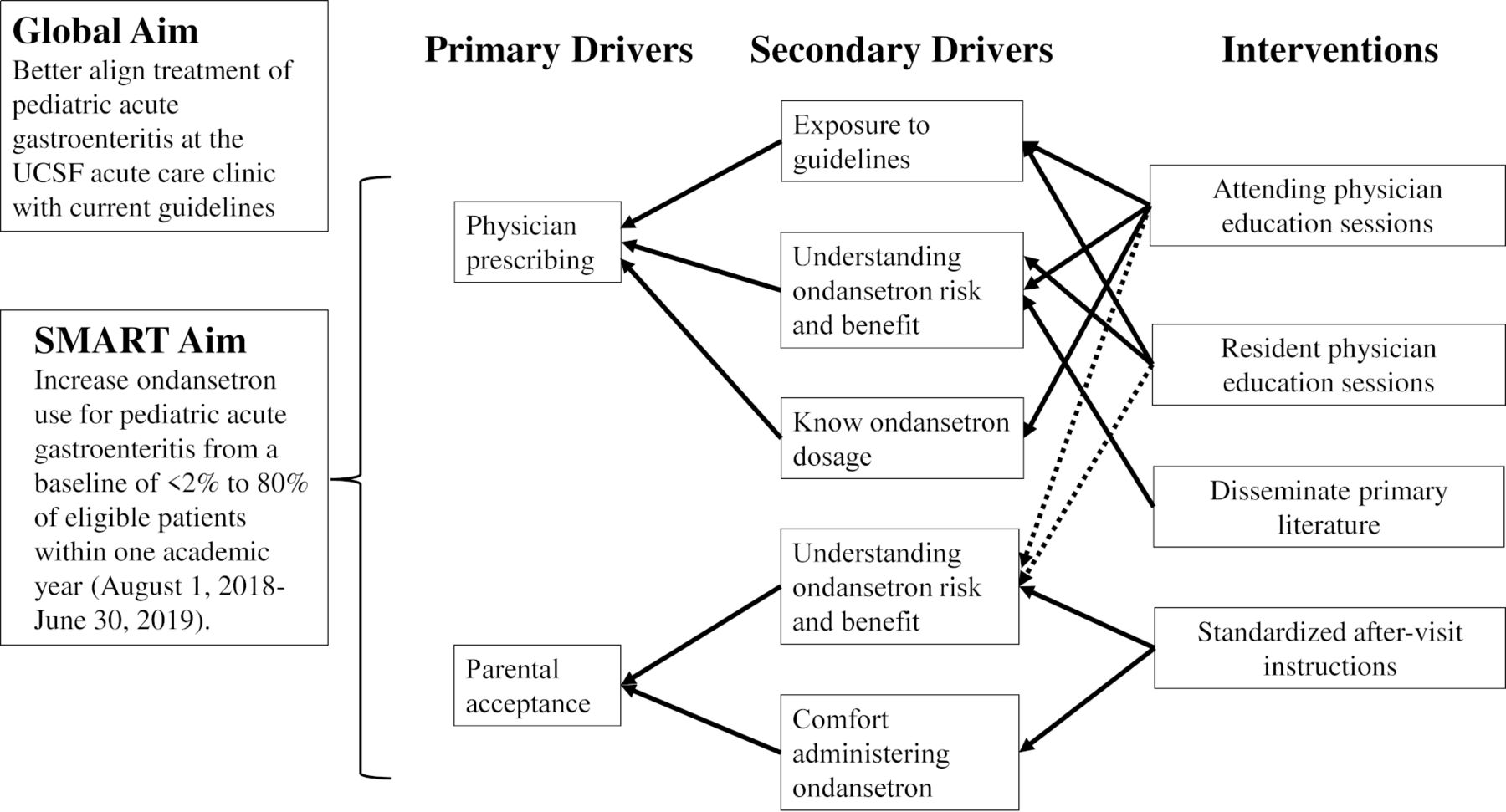
Key driver diagram. UCSF, University of California San Francisco.
Results
Ondansetron use
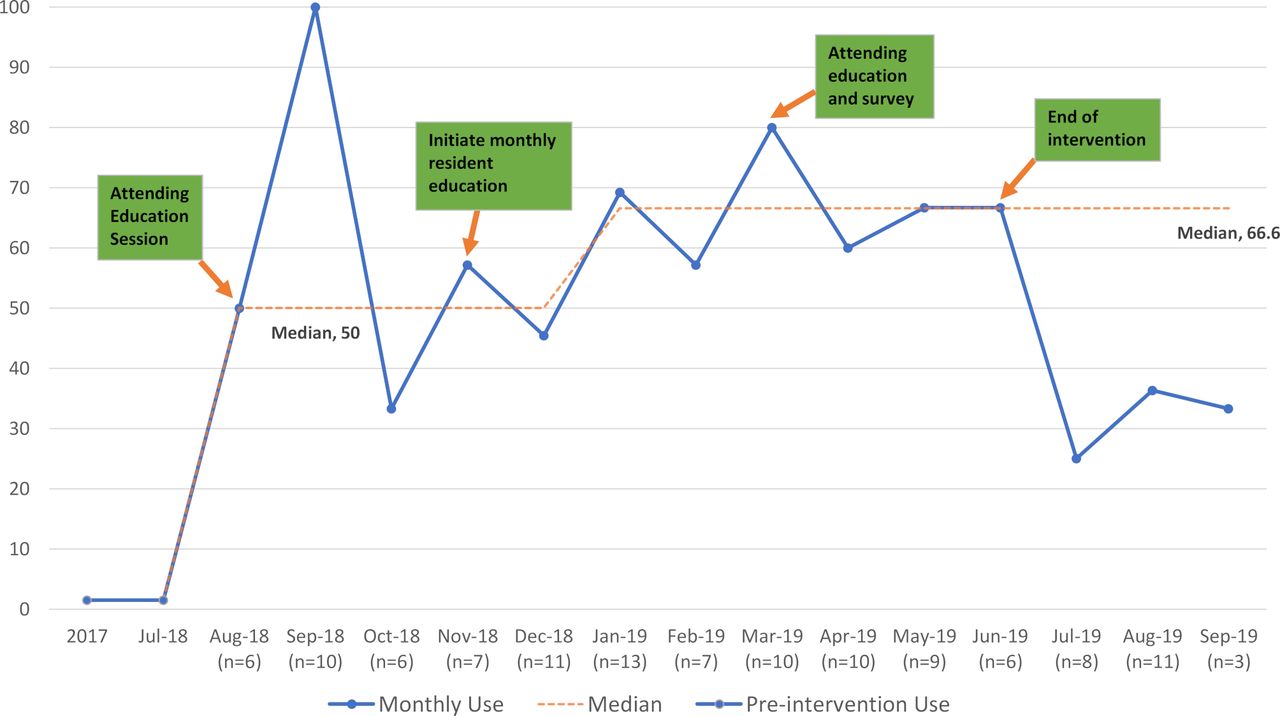
During the intervention period, 63 of 103 total patients with AGE received an ondansetron prescription. Overall, we improved adherence to treatment guidelines for paediatric AGE by increasing ondansetron prescription rates from 1.5% to a median of 66.6% sustained through the final 6 months of the study (p=0.001). Following the initial attending education session, the median increased from 1.5% to 50% (IQR: 39.3%–78.6%) and then further rose to 66.6% (IQR: 60.0%–69.6%) after the start of monthly resident-led education sessions. While a few months exceeded our 80% goal, the dramatic improvement represents a stark change in clinical practice.
Our 3-month postintervention period data (1 July 2019–30 September 2019) showed decreased to a monthly range of 25%–36.3% (figure 2).

{kind=link}
{kind=link}
Monthly ondansetron use.
ORT instructions
Seventeen patients (16.5%) received appropriate oral rehydration instructions, with sixteen of those encounters using our standardised instruction set.
Representation to care
Overall, 7.5% (3/40) of patients without an ondansetron prescription represented compared with 3.2% (2/63) of patients given a prescription (p=0.32). The representations included: two emergency room visits, two acute care visits and one hospitalisation. The only hospitalisation for dehydration occurred in a patient without an ondansetron prescription and inadequate oral rehydration instructions. No patient (0/17) who received both an ondansetron prescription and appropriate oral rehydration instructions returned for care.
Education session attendance
Seven (58.3%) of the 12 general paediatricians working in the clinic attended the initial education session. Ten (83.3%) of the general paediatricians attended the follow-up education session. We did not track attendance at resident education sessions, but we estimate that >50% of residents attended each session.
Survey results
The follow-up survey response rate was 58.3% (7/12). All respondents agreed that ondansetron is safe and well tolerated, but only 71.4% felt comfortable prescribing ondansetron. Those who did not feel comfortable expressed concern that it may mask an underlying diagnosis, particularly appendicitis. Additional barriers to use included parental preference and prior practice habits. Three of seven (3/7) respondents (42.9%) reported preferring the standardised after-visit instructions compared with free text instructions or other prepackaged materials.
Lessons and limitations
Our project design was effective in its integration of front-line residents as educators. Prior research delineates the need for residency QI curricula to promote active trainee participation,16 23 and our project offers a model of hands-on, gradually increasing trainee responsibility. Residents assumed charge of educating their peers, spearheaded data collection and analysis, and assisted in the iterative process of improving ongoing interventions by reviewing and editing the standardised after-visit instructions. The immediate increase in ondansetron prescription rates following the initial intervention reinforces the effectiveness of academic detailing in improving provider knowledge.24 Resident-led education helped improve the lower prescription rate in October 2018; we speculated this drop was due to extinguishing effect of the initial intervention, practice variations as not all attendings attended the initial education session, and random variation from limited sample sizes. By formalising the senior resident’s teaching role, we implemented a system redesign that prioritises trainee education. Peer-based education strongly influences physician practice, and interns learn day-to-day patient management through their senior residents.25–27 The sustained increase in ondansetron use following the implementation of peer-led seminars likely represents special cause variation.28 29
We implemented a process of continuous improvement with each of our interventions. Our physician education material underwent iterative improvements through feedback from attending physicians and residents. Their suggestions helped create a shorter educational module that focused primarily on management steps for paediatric AGE. Our 8-month provider survey also acted as a pathway for change as we were able to tailor future education sessions based on provider needs. The standardised after-visit instructions similarly underwent iterative amendments to eliminate medical jargon, provide patient-specific dosing instructions, and increase readability for families. Through peer-led education and follow-up surveys, we integrated stakeholder feedback to drive programmatic change in our QI curricula and systems-level change with standardised ORT instructions.17 30
The project highlighted the difficulty in changing pre-existing workflows despite education efforts to showcase the benefit of the novel system. We revised the standardised oral rehydration therapy instructions with clinic providers, but utilisation of this standardised after-visit instruction set remained low. Our experience parallels previous work that illustrates the challenges of establishing oral rehydration in high-income compared with low-income countries, possibly related to the ease of access to intravenous fluids.31–33 Difficulties in changing practice habits related to patient instructions may be amplified by our electronic medical record, which contains prepackaged after-visit materials that better align with established workflow. It is also possible that physicians appropriately used prepackaged materials for non-English speakers because our instructions were only available in English.
Our interventions had limitations that may have diminished their impact. The education sessions did not reach all providers due to scheduling conflicts, and our standardised oral rehydration instructions were not translated into multiple languages. On retrospective review, we delivered certain interventions at times of higher compliance. However, the overall data trend supported multiple intervention cycles, as we had not reached 80% use. We also did not track adverse events and were unable to identify patients who may have represented at an institution outside of our EHR. With regards to our measures, we acknowledge that prescribing ondansetron does not equate with its use. With regards to data collection, we anticipated possible inter-rater variability between residents may lead to imprecision or bias in data. To combat this limitation, we conducted a final data analysis at the conclusion of the project in which a single physician re-evaluated all patient encounters in both intervention and postintervention phases, with supervision from a Paediatric Gastroenterology fellow. Lastly, we conducted the study at a single-centre academic teaching clinic, and results may not be generalisable across clinical settings.
To build on preliminary findings and engender sustainable impact, we anticipate the need for larger studies, ongoing interventions, and further systems-level change to combat the decreased compliance in the postintervention period. Our current project serves as an initial step in changing prescriber habits, and the improvements triggered by our educational model may be better sustained through developing order-sets that include preselected ondansetron prescriptions and rehydration instructions for the documented chief complaint. Institutionalising such decision-support tools will serve as sustainable drivers of practice change. We hypothesise that limited sample sizes made it difficult to achieve statistical significance in representation rates, but we postulate that it is clinically relevant that no patient who received both interventions—an ondansetron prescription and appropriate oral rehydration instructions—represented to care. Future studies may consider evaluating whether the reassurance of having an available prescription, rather than actual administration of the medication, is sufficient to decrease return to care. A study examining safety-net antibiotic prescriptions for acute otitis media showed no difference in representation rates between patients started antibiotics versus those given a prescription, despite a significant difference in number of families who filled their prescriptions.34 To incorporate continuous improvement in the distribution of the standardised oral rehydration instructions, we could have considered posting visual reminders at charting stations or empowering nurses to print and review rehydration instructions with patients, a strategy proven effective in other QI processes.33 Instituting reminders at weekly preclinic check-in meetings and allowing for real-time feedback could have further improved our processes.
Conclusion
We achieved a significant increase in appropriate medication usage in our clinic, showing that a trainee-driven, education-based intervention can change prescriber behaviour in the treatment of paediatric AGE. Although we did not meet our initial 80% goal for ondansetron prescriptions, we nonetheless achieved meaningful improvements. The project’s design also offers a unique structure through which medical trainees can incrementally increase their responsibilities to gain hands-on experience with different aspects of QI work. This work served as an initial step in changing workflow and improving adherence to treatment guidelines. Although we anticipated that the programmatic shift created through formalising the teaching role of the senior resident would continue to promote guideline-congruent care to new trainees, sustainability proved difficult to achieve during the transition to a new academic year and a new cohort of residents. Since interns tend to model the behaviour of their supervising residents, institutions considering these types of interventions may need to schedule education sessions for multiple years until all graduating cohorts have gained clinical practice with updated guidelines. Coordinating such a project across academic years may benefit from the support of a QI site director.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
The Committee on Human Research at UCSF determined that this quality improvement project was exempt from Institutional Review Board review.
Acknowledgments
Anne Lyon, Vivek Shenoy, Matthew Nordstrom, Addison Cuneo, Sindhura Batchu, Chatruckan Rajendra.
References
Footnotes
Contributors PVP contributed to the conception and design of the project. He is the primary author of the manuscript. He also contributed to extraction, analysis and interpretation of the data. TW contributed to the conception and design of the project. He was an editor for the manuscript and was essential in extraction, analysis, and interpretation of the data. GR was an editor for the manuscript and contributed to the analysis and interpretation of the data. MH was an editor for the manuscript. SV contributed to the design of the project. She was also an editor for the manuscript and contributed to the analysis and interpretation of the data. SV is the guarantor for this study.
Funding This study was funded in part by NIH T-32 grant #DK007762 (Perseus Patel and Thomas Wallach), and UCSF Dean’s Diversity Award (Sofia Verstraete).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.