Article Text

Abstract
Burn-out among US physicians has been on the rise in the past few decades. Similarly, rheumatologists in the Geisinger Health System have experienced professional dissatisfaction through significant administrative burden and in-basket work. We embedded pharmacists into our rheumatology team in 2019 with the aim of reallocating medication refills to pharmacists, trained professionals in this domain, to help reduce physician workload and burn-out and increase satisfaction. Protocol-driven medication refill parameters per the American College of Rheumatology guidelines and new refill workflows for disease-modifying antirheumatic drugs (DMARDs) and non-DMARDs were created for use by our rheumatology pharmacists. Monthly data on medication refill volume and time saved for rheumatologists were collected from 1 January 2019 to 31 March 2021. Statistical analysis was completed via Shewhart p-charts. The volume of refills by rheumatologists decreased by 73% and the time saved per month for all the rheumatologists increased to 41.5 hours within 6 months. Physicians’ feedback was obtained via anonymous electronic surveys preintervention and postintervention. The statistical difference between the presurveys and postsurveys was calculated via two-tailed unpaired t-testing. It demonstrated reduced burn-out and improved workplace satisfaction. This study showed that the integration of rheumatology pharmacists into our practice can help improve the work life of the rheumatologists. It is important for physicians’ well-being to practice at the top of their scope and achieve work–life balance.
- burnout
- professional
- clinical practice guidelines
- collaborative
- breakthrough groups
- quality improvement methodologies
- pharmacists
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- burnout
- professional
- clinical practice guidelines
- collaborative
- breakthrough groups
- quality improvement methodologies
- pharmacists
Problem
Physicians in the Department of Rheumatology at the Geisinger Health System with sites in the West, Central and Northeast Pennsylvania collectively respond to an average of over 1200 medication refill requests per month among other administrative tasks. This task takes a significant amount of administrative time and has been a source of dissatisfaction and burn-out among physicians. The aim of this project was to decrease physician burn-out and increase satisfaction by introducing a pharmacist-run protocol-driven medication refill process. Our goal was to reduce physician medication refills by 50% over the first 6 months.
Background
Increased electronic health record (EHR) workload is a great source of physician dissatisfaction. Research shows that physician burn-out drivers include inefficient work processes and clerical burdens, and increased support for clinical work has demonstrated benefits in reducing burn-out.1
In the Geisinger Health System, rheumatologists spend a significant amount of time addressing in-basket tasks using Epic Systems. This ‘Epic In-Basket’ is an electronic messaging system through which a healthcare provider receives laboratory and imaging reports, medication refill requests, patient questions, communication from other providers and allows for exchange of messages and coordination of care without the patient being in the clinic. Anonymous electronic surveys suggested that at least 88% of rheumatologists were dissatisfied with their in-basket work while 65% were dissatisfied with their medication refill work.
The refills of disease-modifying anti-rheumatic drugs (DMARDs) require careful patient counselling, as well as frequent monitoring of laboratory data, clinical efficacy and side effects. This is a clinical administrative task that is not easily replaced by other members of the healthcare team. Pharmacists, however, play a unique role with an expertise in safe and effective medication administration and patient education. Additionally, some pharmacists are trained in medication reimbursement structures, patient assistance programmes and other drug resources.
In rheumatology practice, addition of pharmacists is still novel but has shown benefits in certain areas of patient care.2–4 A study looking at a pharmacist-managed titration programme of serum uric levels in gout patients showed that pharmacist managed interventions achieved lower uric acid levels.5 Based on their pharmacological training and the above-mentioned positive experiences, we hypothesised that embedding pharmacists into our rheumatology team could improve the life of our department by fulfilling the Quadruple Aim. The Quadruple Aim expands on the Triple Aim approach developed by the Institute for Healthcare Improvement to ‘improve the patient care experience, improve the health of a population, and reduce per capita healthcare costs’ by also seeking to improve the physician experience of providing care.6 The concept of improving physician experience is widely accepted as one of the keys to optimising healthcare performance.
Measurement
At baseline, all the medication refills were being carried out by the rheumatologists from 1 January 2019 to 30 September 2019. The rheumatologists and in-training fellows were refilling an average of 1200 medications per month in the Northeast and Central regions. Postintervention in October 2019, the physician and pharmacist medication refills were measured monthly.
Process measures were calculated by obtaining the monthly average of volume of medication refills at baseline by physicians and postintervention by physicians versus pharmacists. Outcome measures were determined by calculating the monthly work time saved for physicians as a group and per clinical full time-equivalent (FTE) postintegration of pharmacists to the team. Total physician time saved per month was calculated by multiplying the number of pharmacist refill encounters with average physician refill time. Physician time needed per refill as determined by the American College of Rheumatology (ACR) refill parameters was derived by averaging the time per message for 40 refills across 5 physicians. This was calculated to be 1 min and 57 s (~2 min). The time saved per month was divided by the number of clinical FTEs to calculate the time saved per individual rheumatologist. Shewhart p-charts were used to measure significance for volume and time saved.
Rheumatologists’ satisfaction with EHR work was gauged via anonymous electronic surveys prepharmacist and postpharmacist addition. Satisfaction was rated from 1 (not happy) to 5 (high satisfaction). Two additional questions were asked in the post pharmacist survey related to the effect on work and burn-out.
Patient and public involvement
Patient and public were not part of the study design and research question of this project, however, were involved in the project. Patients were first involved through receiving medication refills from pharmacist through the protocolised refill process. Feedback was not measured objectively through project, but informal feedback was positive. Research questions were developed with the safety and convenience of patients in mind. Patients were not directly involved in outcomes measures or recruitment to the study.
Design
Two pharmacists were integrated into the Rheumatology department at the Geisinger Health System in the fall of 2019 and took over the medication refill process in a stepwise standardised fashion. This standardisation was felt to be important in improving the efficiency of in-basket work without compromising patient quality of care and safety. We measured volume of refills, physician work time saved and correlation with their work satisfaction at baseline and postintervention.
Our quality improvement team consisted of one in-training fellow, a rheumatologist with training in the area of quality improvement, the Geisinger Health System Director of Quality and Innovation with knowledge of the hospital system, the director of Rheumatology Department, volunteer rheumatologists who carried out tests at small scale, pharmacists and information technology.
Protocol-driven medication refill parameters for DMARDs and non-DMARDs were created per ACR guidelines.7 8 A workflow algorithm was created to direct refill requests from each region to the pharmacy pools. The general medication refill parameters pertained to all our medications and asked the following questions: Has the patient been seen in the last 12 months? Have labs been completed within the past X months (specific to drug)? Are labs within normal limits or stable at baseline? Is the medication dose correct? Are there any new drug interactions with the DMARD? Are there any care gaps that need to be addressed? Responses to these questions were linked with a corresponding action such as performing the refill, repeating labs or stopping the refill. This general refill guide was supplemented by Specific Refill Parameters for each individual drug or drug class. It included monitoring of laboratories, pregnancy status, and common contraindications/precautions. These refill parameters were part of our Rheumatology-Pharmacy Collaboration Manual and available to all departmental staff.
We had monthly department meetings where we shared the details of the project and received input from our team during the planning and rapid cycle testing. We felt it was extremely important to gain knowledge from the team who has first-hand experience in dealing with medication refills. We started our intervention of medication refills with embedded pharmacists 1 October 2019 and collected monthly data via EHR.
Our intervention was started at a small scale with only four volunteer physicians and by testing only our DMARD refills. Pharmacists sent a copy of their patient refill encounters to their respective physician with each refill for the first 4 weeks. This step was taken to assure a safe care delivery until both physician and pharmacist felt comfortable with the process. Our information technologist created a medication refill dashboard comparing the monthly volume of the refills by the physicians versus the pharmacists, respectively.
Strategy
Our project aim was to improve physician work satisfaction by reducing medication refill encounters by 50% over a 6-month period through use of a protocol-driven medication refill process by addition of two new pharmacists to our team.
PDSA cycle 1
The PDSA Cycle (Plan-Do-Study-Act) is a systematic process used for quality improvement through documenting effect of interventions. Our initial intervention was introducing protocol driven DMARD refills by pharmacists to a select group of physicians over a 4-week period. During this small-scale piloting period, the pharmacist copied their templated refill note to the respective physician to allow for a safe and efficient transition of the refill task. The pharmacists could contact the physicians with any refill questions during this period. Physicians did notify the pharmacists if they noted any refill discrepancies during the transitional period. Monthly refill volume by physicians and pharmacists and time saved by physicians were measured. Data were collected monthly from 1 October 2019 to 31 October 2019. Shewhart p-charts were used for the statistical analysis.
PDSA cycle 2
Once the physicians and the pharmacists felt comfortable with the new workflow process, the decision was then made to expand the DMARD refill process by pharmacist to the whole Rheumatology department in the Central and Northeast PA regions from 1 November 2019 to 30 November 2019. The process and data measurement were carried out in a similar fashion as above. Regular monthly team meetings were held give updates and receive team’s input. During the process, some questions were raised about the refill parameters, such as clarification of certain criteria or their flexibility. There was concern that the stringent parameters may lead to more unnecessary in-basket work when routed back and forth to physician. Per this feedback, edits to the Refill Parameters were made to either further clarify the refill criteria or allow for safe but less stringent parameters. For example, DMARDs were originally approved for refill if they had monitoring labs within 3 months but this was increased to 4 months to accommodate patients that were marginally out of the time frame. No safety concerns were reported during this process. After cycle 2, physician refill encounters had been reduced by over 50%. Monthly time saved by physicians was marked at 11.3 hours per the group and 1.5 hours per physician FTE. After the first 4 weeks of the pharmacists copying the physician to their DMARD refill note, a refill note was no longer sent to the physician unless their attention was needed to address an issue.
PDSA cycle 3
The goal for this cycle was to introduce the non-DMARD refills per refill criteria protocols by the pharmacists to the same initial select group of physicians as in PDSA 1 over a 4- week period in December 2019. A list of the non-DMARDS included but was not limited to prescription NSAIDs, osteoporosis medications, xanthine oxidase inhibitors, calcium channel blockers, etc. This list was made available in our rheumatology-pharmacy manual shared with all staff. The general process of refills for the non-DMARDs remained the same as for the DMARDs with the exception that the non-DMARD criteria were followed. The pharmacist carried out the non-DMARD refills and copied a template of the refill note to each respective physician for the first 4 weeks and only if the physician attention was needed after that time frame. During this cycle, a workflow was established and a level of trust was created. We continued to measure data monthly. At our monthly meeting, feedback included adding antipsychotropic medications commonly used to the non-DMARD list as well. Refill parameters were created for the additional non-DMARDs and the manual was updated. By the end of December 2019, data collection revealed that 55% of combined refills for DMARDs and non-DMARDs were being carried out by pharmacists and 44% by physicians. Time saved by physicians was 23 hours for the group and 3 hours per physician FTE, respectively, reaching statistical significance per p-chart analysis.
PDSA cycle 4
In this cycle, we extended the non-DMARD refills process across all physicians in January 2020. We continued to collect monthly data on combined volume of refills for DMARDs and non-DMARDs for physicians and for pharmacists separately and time saved by physicians. At our monthly meeting, we received feedback that it was difficult for physicians to clearly and quickly understand from the pharmacist note when their attention was needed to address an issue. The note was redesigned to include a bold coloured clinical question at the top to quickly grasp physician’s attention and efficiently address it. By the end of January 2020, data collection revealed that 68% of combined DMARDs/non-DMARDs refills were being carried out by pharmacists and 32% by physicians. Time saved by physicians was, respectively, about 31 hours for the group and 4 hours per physician FTE, a sustained improvement.
PDSA cycle 5
The aim of this cycle was to assure that the refill improvement was sustained and to gauge the physician satisfaction with the process in our central and northeast PA rheumatology sites. In both February and March 2020, pharmacy refills continued to trend up to 73% of refills which translated to approximately 42 hours per month saved per physicians as a group and 5.4 hours per physician FTE, both sustaining significance in p-chart analysis. In addition, we gauged physician satisfaction anonymously via postintervention electronic surveys in early Spring 2020. Informally, feedback regarding the addition of pharmacists was very positive and well received. Similarly, pharmacists were also surveyed and felt the work was within their scope of training and they were satisfied with both their new clinical specialised roles within rheumatology and the medication refill process.
Results
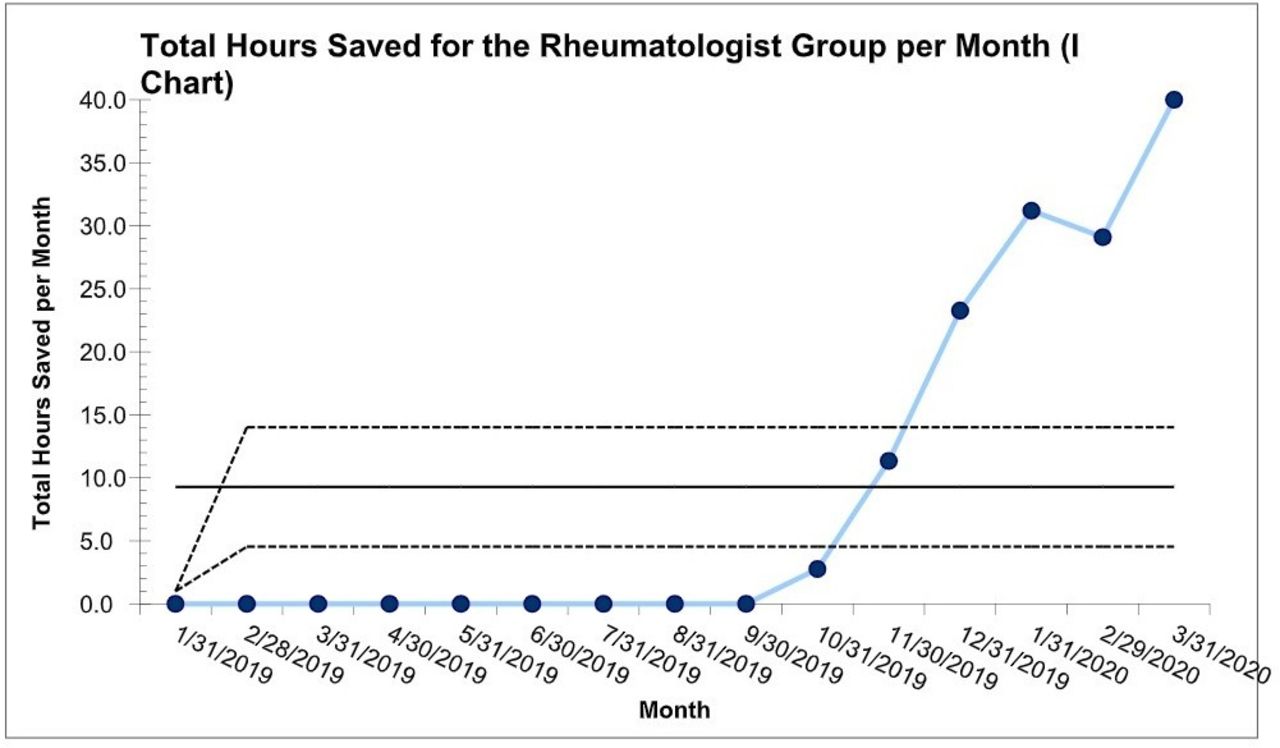
Our pharmacist intervention achieved over 70% reduction of physician refill encounters over a 6-month period. The volume of medication refills by physicians decreased from 1201 out of 1201 refills per month (or 100% of all refills) prepharmacist at baseline in September 2019 to 464 out of 1742 (26.3%) post-pharmacist intervention in March 2020 (figure 1). The total monthly time saved for all the Geisinger Rheumatologists in the east and central regions (15 physicians, 7.75 FTEs) increased from 0 hours in September 2019 to 41.5 hours postpharmacist in March 2020 (figure 2). Respectively, the monthly time saved per physician FTE increased from 0 hours at baseline in September 2019 to 5.4 hours 6 months postintervention in March 2020 (figure 3). Shewhart p-chart analysis met statistical significance for time saved per the individual and group of rheumatologists respectively with the implementation of pharmacists into our team. This significance was reached within 2 months of intervention and sustained throughout it. Though there was a slight drop in refills and times saved in February 2020, the data rebounded March 2020 suggesting sustained improvement with usual cause variation between these last 2 months.
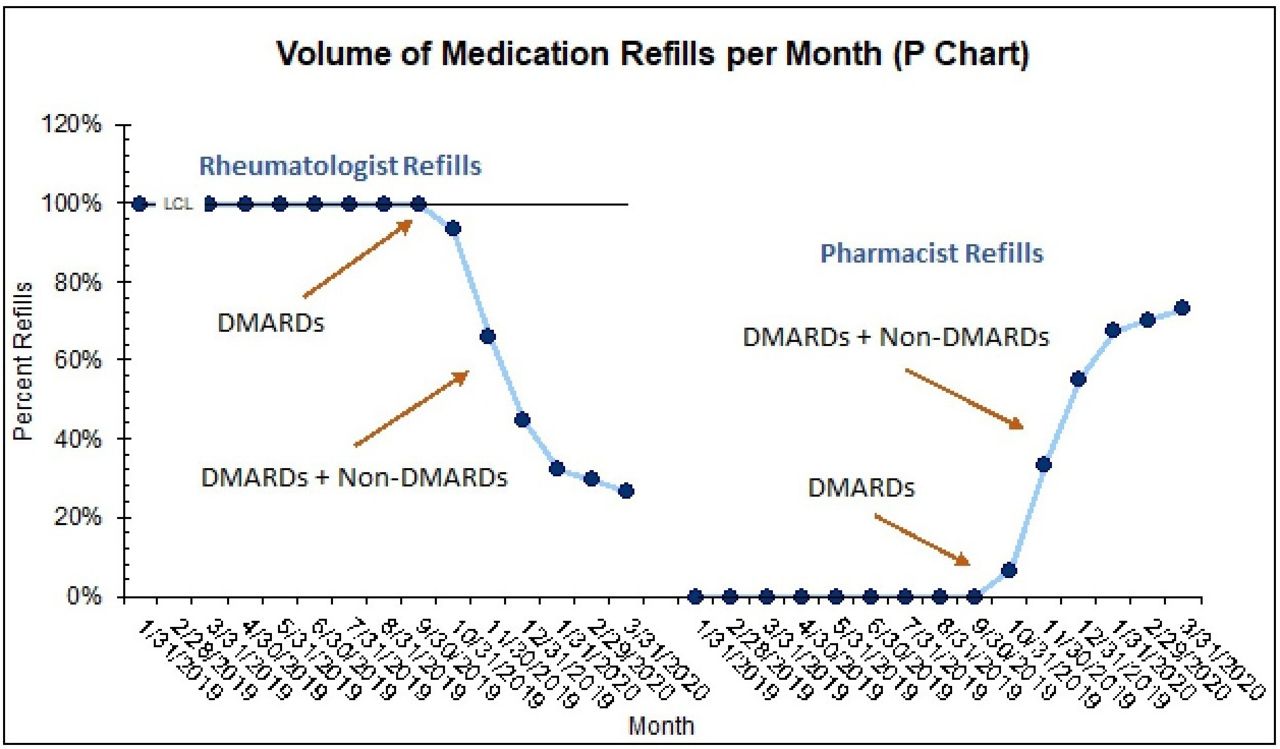
Rheumatologists versus rheumatology pharmacists monthly refil volume. DMARDs, disease-modifying anti-rheumatic drugs.
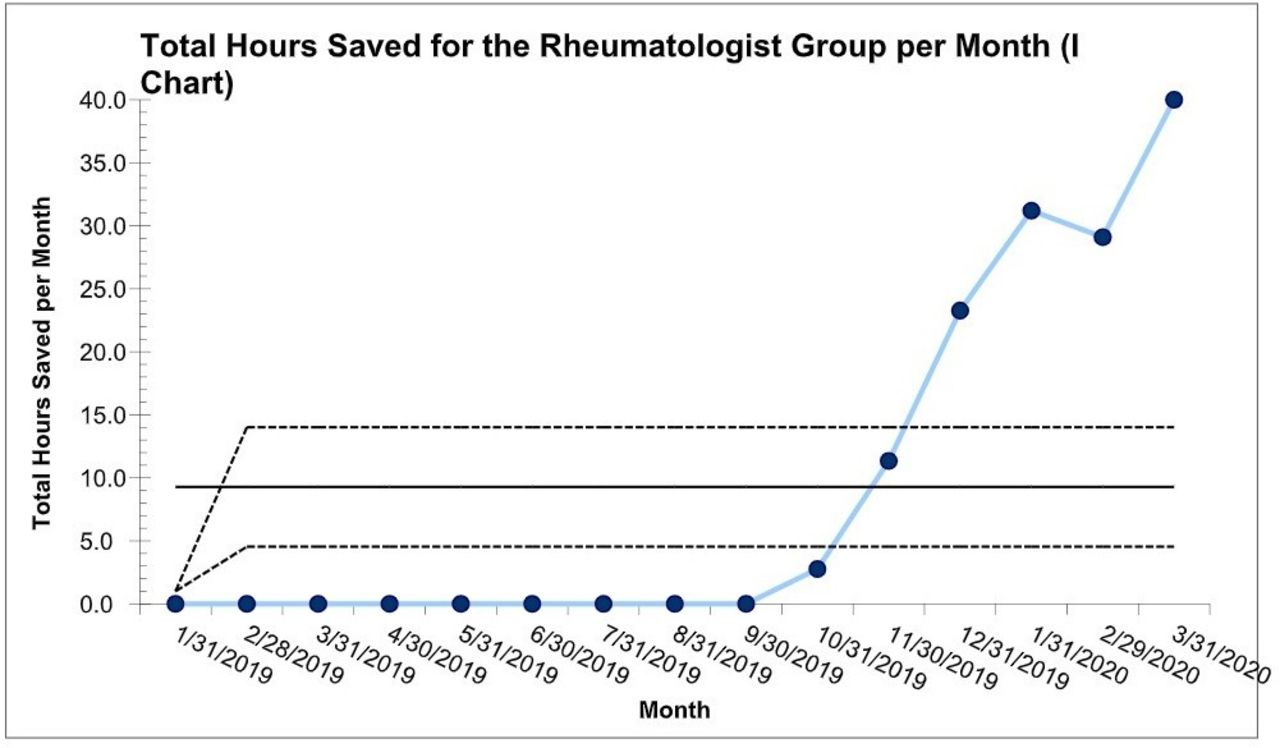
Time saved for the rheumatolgist group by the introduction of pharmacists.

{kind=link}
{kind=link}
{kind=link}
Time saved per rheumatologist FTE by the introduction of pharmacists. FTE, full time-equivalent.
T-testing was used to compare physician satisfaction preintervention and postintervention. Sixteen out of 17 physicians (94%) responded to the preintervention survey. Fourteen out of 15 physicians (93%) responded to the postintervention survey. One hundred per cent of physicians that responded, reported that the pharmacist addition to the team helped them leave work on time. Additionally, physicians reported that their workload interfered less with life outside of work (n=14), and 79% of them reported less burn-out. The mean satisfaction with EHR refill work improved from 1.4±0.2 at baseline to 4.3±0.2 (p<0.001) postpharmacist introduction.
Lessons and limitations
Our study has a few limitations. The data presented are limited to only 6 monthly data points post implementation of pharmacists. Perhaps more data points may be helpful to show continued sustainability of improvement for a year prior to spreading changes to our west rheumatology site. However, present data have given us a high level of confidence that these trends will continue in a positive direction.
We did not reach a level where 100% of refills were being carried out by pharmacists. Only 73% refills were carried out by the pharmacists by March 2020, while the other 27% were still being carried out by the rheumatologists. This may be explained by the fact that some of the medication refills were being carried out by the rheumatologists at the point of care with patients. The COVID-19 pandemic in early 2020 may have also played a role in increased physician refills because of high refill demand by patients due to fear of medication shortages. Additionally, COVID-19-related illnesses later led to pharmacy staff shortages.
There may have also been initial personal bias among some physicians about trusting someone else with their patients’ care. It took a standardised approach to care, development of a manual with refill criteria, workflows and multiple PDSAs to build a trusting and collaborative multidisciplinary team working towards providing a safe, timely and effective patient care.
We were limited to surveys gauging physician satisfaction. Physician burn out is a well-recognised phenomenon but presented a challenge as it was difficult to measure. We could have included use of validated burn-out measures such as the Maslach Burn-out Inventory which would create a more reproducible method for other healthcare systems to implement. More frequent survey points during the intervention could also be used to demonstrate an evolving change but would be at risk of burdening physicians with more administrative tasks and defeating the intervention. Due to the voluntary nature of our surveys, we also did not capture the same number of survey responses before and after intervention. One physician was on extended personal leave, and one physician did not respond. This could reflect an isolated physician’s disinterest or simply having no time to reply. Most physicians, including the initially reluctant ones have embraced our pharmacy collaboration and have inquired about expanding pharmacists’ roles within their area of expertise in patient co-management. Furthermore, the two-tailed t-test of physician satisfaction per their survey reports revealed statistical significance.
Another limitation of this study is that we did not include balance measures. However, neither the patients nor their physicians reported any significant adverse side effects related to inappropriate medication refills during the study period. Future balancing measures may include surveying patient satisfaction, measuring number of medication side effects and time to refill preintervention and postintervention.
Our study did have strengths. Initially physician engagement was slow, but confidence grew after seeing that their patients’ refills were safely done, and they were getting to leave work earlier when the pharmacists joined the team. Physicians were pleased to see that the pharmacists were providing additional services to their patients, including but not limited to providing medication and injection education, checking pre-screening and monitoring follow-up laboratories, facilitating preauthorisation processes and performing follow-up phone calls for medication side effects. Physicians reported positive feedback from their patients and became personally engaged in the collaborative work with the pharmacist.
The standardised refill approach per our Rheumatology-Pharmacy Manual created by our team is an available resource for all the physicians in the department. In addition, it is being used as a training resource for the new incoming rheumatology fellows.
We were able to do rapid cycling tests in real time and dynamically analyse our results via Shewhart p-charts to see when a change occurred and if it resulted in decreased refills (improved Epic in-basket work) by physicians. The two-tailed t-tests gave us a meaningful way to show statistically significant improvement in physician satisfaction with the process. Though descriptive analysis could be used to report the outcome measures like the physician time saved, we believe that our statistical analysis summary described this group with complete certainty without leaving room for questions in the readers’ mind outside of measurement error.
The intervention was tested and implemented successfully at two different Geisinger Rheumatology locations—our central site in Danville, Pennsylvania, USA and our Northeast site in Wilkes Barre, Pennsylvania, USA. The positive experience at the above two sites, motivated us to continue to spread this improvement process to our West site in State College, Pennsylvania, USA.
An important strength of this study is our medication refill dashboard which reliably pulls information in real time from our EHR on a monthly basis. It has allowed us to collect data preintervention and postintervention and follow it longitudinally to assure sustainability within the process.
Furthermore, our Geisinger Health System is committed to providing quality and innovative healthcare delivery to our patients and has been fully engaged and supportive of the multidisciplinary team approach in rheumatology as well as system wide.
Conclusion
In early 2020, 51% of rheumatologists reported burn-out in the workplace.9 This negatively impacts physician work effort, patient outcomes and healthcare costs. Harvard Gazette reported that burn-out among physicians is costing the healthcare system in the United States approximately US$4.6 billion per year because of reduced hours, physician turnover and expenses associated with physician finding and hiring replacements according to an analysis of the economic impact of the problem.10
Similar to the national report, our rheumatology team felt burdened with administrative tasks, particularly the Epic in-basket work and refills which led to lack of engagement. The intervention of pharmacists to our team introduced collaborative teamwork and shared responsibility in a safe expert driven patient management setting. The project achieved its aim of improving physician work satisfaction and reducing burn-out through implementation of a protocol-driven refill process by pharmacists and decreased medication refills and in-basket work for physicians. The intervention created a medication refill process that was embedded in the system and shown to last throughout our study period. Additionally, pharmacists in the department expanded their services to include roles in patient medication education, prior authorisation for biological therapies and medication comanagement with physicians.
While the physicians are not privy to the health system economics and decisions for financial allocation of pharmacists to our department, we can infer that there is value added through increased physician time saved, satisfaction and decreased burn-out. Physician satisfaction at work allows for their ability to continue to work their regular hours at their present healthcare system, and therefore, decreasing the inquiry of reduced work hours or turnover physician costs to the health system.
We are one of the first rheumatology programmes in the country to incorporate rheumatology pharmacists to our team. This novel approach to our patient care has proven successful and has great potential for reproducibility and spread of pharmacist integration through different institutions and medicine teams facing similar challenges. Members of the healthcare team individually bring a unique blend of different educational backgrounds, experiences and skill sets to patient care. Reallocating medication refills to pharmacists who are trained masters in this domain allows both pharmacists and physicians to work at the top of their license. This does not only provide high-quality care and enhanced patient experiences but allows professional satisfaction in doing what we were trained to do. Implementing a pharmacist into practice has brought us closer to achieving the fourth Aim of Quadruple Aim-improving the physician experience.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by our institutional review board.
Acknowledgments
The authors thank the Department of Rheumatology at Geisinger Medical Center for their role in participating in the protocol-driven medication refill process and kind feedback.
Footnotes
Contributors EIR, JC and EN created original project conception and design. JC, EN, ST and DMG created project workflow for refills, general and specific medication refill parameters, and designed refill process. JCh created computational framework and analysed the data. All authors contributed significantly to collection of data and interpretation of data. All authors contributed to drafting, revising and confirming final version of manuscript. EIR is responsible for overall content as guarantor.
Funding Project is funded by Graduate Medical Education at Geisinger Medical Center.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.