Article Text

Abstract
Introduction The need to better prepare youth with type 1 diabetes for the transition from paediatric to adult care is evident. As part of a regional quality improvement initiative, a novel Pre-Transition (Pre-T) Visit was developed and piloted at a paediatric tertiary care centre in January 2018 for patients aged 15–18 years to capture the status of their self-management skills, introduce transition tools and identify self-care goals and knowledge gaps to be addressed prior to transition.
Purpose To evaluate patient and family satisfaction, visit relevance and patient engagement with a novel Pre-T Visit.
Methods From May 2019 to March 2020 a survey was offered to all youth who attended a Pre-T Visit and their parent(s)/caregiver(s). Patient and family satisfaction with, relevance of and engagement with the Pre-T Visit were evaluated using a 5-point Likert scale. Multivariable regression was used to assess patient factors associated with patient level satisfaction.
Results Of the 63 youth who participated in a Pre-T Visit, 60 completed the survey. Mean age (SD) of participants was 16.7 (0.8) years; 47% were female. Mean (SD) haemoglobin A1C (A1C) was 8.2% (1.8). Patients reported high levels of satisfaction (95% quite or extremely satisfied) that were consistent across age, A1C, gender and disease duration. Visit relevance and engagement were also rated highly by youth. Parent participants (n=27) also reported high levels of satisfaction (89% quite or extremely satisfied) and relevance.
Conclusions Pre-T Visits were rated highly by patients and their parents. Their impact on glycaemic control and health outcomes following transition requires further study.
- transition to adult care
- patient satisfaction
- paediatrics
- diabetes mellitus
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the manuscript or uploaded as supplementary information (questionnaires). Additional data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The transition from paediatric to adult care can be challenging for emerging adults as they establish their autonomy and personal identity during this unique developmental period1 while balancing the daily demands of the disease. For individuals with type 1 diabetes (T1D), as a result of both physiological and psychological factors, this stage is associated with deterioration in glycaemic control, increased diabetes complications and hospitalisations, decreased adherence to diabetes-related management tasks, decreased clinic attendance, increased risk-taking behaviours and increased risk of psychiatric disorders.2–8 Furthermore, gaps in care during the transition period are specifically associated with an increased risk of ketoacidosis or death.4 Herein, the term ‘transition’ refers to the transition from paediatric to adult diabetes care. This transition necessitates greater personal responsibility for diabetes care at a time when there are many competing priorities and developmental challenges which can impact diabetes management and control.9
A variety of identified factors may inhibit a successful transition process, leading to poor outcomes. Many patients in the transition age group have not discussed transition with their current care provider, have not been given the name and contact information for an adult care provider and describe a lack of transition preparation.2 10–14 Worsening glycaemic control during transition suggests suboptimal self-management at a time when there is an expectation that youth will function more independently. The years leading up to transition provide an opportunity to address self-management skills.
Despite initiatives aimed at improving the process and experience for adolescents and young adults with T1D, and technological innovation to improve glycaemic control, health outcomes in this age group remain worrisome with a significant increase in mean haemoglobin A1C (A1C) over the last decade.15 Interventions to address this issue have been evaluated with varying success. These include assessments of transition preparation, young adult clinics, transition clinics and the use of transition care coordinators.16–22 Outcomes of interest for transition-related interventions often include measures of glycaemic control, diabetes-related complications, clinic attendance and patient experience measures (including satisfaction). While these interventions to support transition often initially improve patient satisfaction, glycaemic control and clinic attendance, impact wanes once the interventions are complete20–22 and indices of healthcare delivery and outcomes remain suboptimal.4 15 Insufficient focus by T1D care teams on preparation for independent management and adult care likely contribute to these findings as self-management competency is associated with readiness to transition.23 A focus on interventions that support development of and confidence in individual self-management skills for youth with T1D to help them to maintain or improve glycaemic control as their independence increases may result in more sustained impact. To do this, it is critical to understand the gaps in patient education and self-management skills so that education and support can be tailored to individual needs.
Improving transition care has been identified as a critical element of optimising healthcare delivery internationally.24 25 The transition process should begin in early adolescence and provide healthcare that is coordinated, uninterrupted and developmentally appropriate with a focus on self-management.26–28 In keeping with these recommendations, in 2016 a comprehensive set of recommendations for a more structured and consistent provincial approach to transition was published.29 Subsequent implementation of these recommendations at our centre included the creation of the Pre-Transition Visit (Pre-T Visit). The purpose of the Pre-T Visit is to capture the status of the youth’s self-management skills (an element of transition readiness) and introduce tools for transition so that specific goals and gaps in knowledge can be identified and addressed during the pre-transition/transition period.
Transition for youth with T1D remains a concern and likely requires multiple interventions and adjustments to the structure of care. No single intervention has proved to be universally helpful with benefits maintained beyond the immediate intervention period. The novel Pre-T Visit was designed to address care delivery recommendations in affiliation with the Diabetes Learning Center (DLC), our longitudinal diabetes education programme, within existing clinic resources. The Pre-T Visit is a step towards personalised transition preparation, allowing for identification of knowledge gaps and goals for optimising self-management skills which should result in more sustained health benefits. The primary objective of the study was to evaluate patient satisfaction with the Pre-T Visit in order to inform improvements of this novel programme.
Methods
Setting and context
In our paediatric diabetes clinic, individuals with T1D transition once they are 18 years old, which aligns with local and regional care policies. The novel Pre-T Visit was an outcome of a transition implementation plan designed to address the prioritised provincial recommendations.29 The implementation plan was developed by a working group consisting of multidisciplinary paediatric and adult care providers (physicians, educators, social workers), administrators and patient/family representatives. The Pre-T Visit primarily aims to capture the status of a set of standardised skills in each youth in order to help guide future self-management education and self-efficacy support within our diabetes programme. Importantly, no extra funding or resources were allocated for the development or implementation of this intervention which required restructuring of existing clinic flow and staff responsibilities. No care provision resources were eliminated to allow for this intervention.
Pre-T Visits were implemented in January 2018 in our clinic and were ongoing until diabetes care became almost entirely virtual in March 2020 due to the COVID-19 pandemic. The Pre-T Visit is a 45 min scheduled appointment with a diabetes educator on the same day as a routine clinic appointment for youth aged 15–18 years. The educators evaluate self-management skills using a templated documentation tool embedded in the electronic health record as well as a guide to help ensure skills are evaluated systematically (online supplemental file 2). Patients are encouraged to independently participate in the visit, and, with youth consent, parents/caregivers are invited to join the youth and educator at the end for a visit summary (ensuring exclusion of any sensitive topics that youth prefers not to share). The visit summary is a verbal synthesis of the youth’s transition readiness including three personalised transition-related goals. The visit is offered to as many eligible patients as possible within resource restrictions (one youth per half-day clinic). Youth at the younger end of the targeted age range (closest to 16.0 years) are preferentially selected if multiple patients are eligible in the same clinic to allow for more time to address the gaps while in the paediatric setting. Identified knowledge gaps are then addressed through focused education within the DLC.
Supplemental material
Study design
From May 2019 to March 2020, all patients and their parents attending a Pre-T Visit were invited to participate in the study. Patients were eligible if they had a diagnosis of T1D, were followed in the diabetes clinic, and were 15–18 years of age. Patients were excluded if they were unable to consent due to lack of capacity or unable or uncomfortable completing the survey questions in English or French. There was no requirement for minimum duration of diabetes. At the end of the Pre-T Visit, the educator who led the visit introduced the study to the youth and if the youth agreed to learn more, an electronic survey was administered using a clinic iPad provided to the youth. The first screen was an explanation of the quality improvement initiative and (voluntary) option to participate. Once the youth survey was complete, the educator administered the survey to the parent/caregiver in the same way. Participants completed the surveys independently.
Study outcomes
The primary outcome was patient satisfaction with the Pre-T Visit. This was evaluated with one question about overall satisfaction with the visit as well as a combined outcome aggregated across six questions about satisfaction with specific components of the visit. Secondary outcomes included: (a) patient-reported self-engagement with the visit, which was evaluated with two questions, (b) patient-reported relevance of the visit to their own care which was evaluated as a combined outcome aggregated from the answers to six questions about relevance and (c) family-reported satisfaction and relevance with the Pre-T Visit after-visit summary.
Instrument development
Two surveys were developed—one for patients and one for parents/caregivers. Existing literature and study objectives informed the development of the surveys. Surveys were drafted by authors AM and EBG using the New World Kirkpatrick Model,30 revised based on feedback from a survey methodologist, a statistician and two diabetes educators, then piloted with two patients and two parents who participated in Pre-T Visits prior to recruitment. Final versions (online supplemental file 1) incorporated their feedback. Data from these individuals were not included in the analysis.
Supplemental material
The patient survey consisted of 20 items assessing satisfaction with, engagement in, and relevance of the Pre-T Visit. There were seven questions pertaining to patient satisfaction where participants were asked to rate their satisfaction with the overall visit, the format of the session, the review of self-management skills, the materials received, the process of identifying self-management goals, the follow-up arranged to review goals and the introduction to transition evening (an interactive event for youth and families to learn about regional adult diabetes programmes and transition services), using a 5-point Likert scale ranging from ‘not at all satisfied’ to ‘completely satisfied’. There were six questions pertaining to patient-reported visit relevance where patients were asked to report relevance of components of the visit to the review of self-management skills, the materials received, the process of identifying self-management goals, the follow-up arranged to review goals and the introduction to transition evening, using a 5-point Likert scale. They were also asked about ideal timing of the Pre-T Visit with respect to patient age.
The parent survey consisted of six questions about their satisfaction with, and relevance of, the Pre-T Visit summary that was shared with them.
Data collection was managed using Research Electronic Data Capture Database.31 32
Data analysis
Baseline characteristics of the study participants were summarised using descriptive statistics, where mean and SD or median and IQR were used for continuous variables as appropriate. Categorical variables were summarised using frequencies and percentages. To demonstrate the range of overall satisfaction across multiple items and for each of the items separately, a Likert plot was used. A composite outcome score was defined by aggregating satisfaction scores from participants who responded to all six questions (not including the overall satisfaction question). This score may provide a better estimate of satisfaction since it is constructed from individual items and allows for identification of potential factors associated with satisfaction. It can be more reliable than answering a Likert score question about overall satisfaction. Multivariable linear regression, with the composite outcome as a dependent variable, was performed with the aim of identifying potential factors associated with favourable outcome. The independent variables considered in the regression analysis were age, disease duration, gender and A1C on day of visit. The distribution of secondary outcome, relevance score, was illustrated using a Likert plot. Patient-reported engagement, and parent/caregiver satisfaction were described in the form of frequencies and percentages. In order to examine internal validity, consistency among the seven items within patient satisfaction and the six items within patient relevance were evaluated using Cronbach’s α coefficient.33 34 All analyses were performed using the R statistical software.35
Patient involvement
There was patient and parent representation within the transition working group that designed the Pre-T Visit as a way to address transition recommendations. Patients and families were also involved during the survey design phase. They were asked to pilot the survey and provide feedback with respect to how to make the survey more user friendly and whether the time required to complete it was acceptable.
Results
Survey completion
Sixty-three youth with T1D completed a Pre-T Visit during the study period and 60 (95%) completed the survey (59 in English, 1 in French). Of those who chose not to complete the survey, reasons provided were: ‘running out of time’ (1), no comment (1), and unclear response (1). The mean age of those who completed a visit was 16.7 years (SD 0.8), 28 (47%) were female and the mean A1C was 8.2% (SD 1.7, range 4.2%–14%). Patient characteristics are displayed in table 1 and did not appear to differ from the clinic population within that age range.
Patient characteristics of Pre-T Visit survey participants (who completed survey) and diabetes clinic patients aged 15–18 years (from clinic report February 2019)
Of the 41 parents/caregivers approached, 27 consented to complete the survey. Of those, 19 (70%) were mothers and 8 (30%) were fathers. Reasons for parents/caregivers not completing the survey were not systematically collected but based on recall of diabetes educators, the physician being ready to see the patient may have interfered with survey completion.
Patient satisfaction
Among those participants who answered the survey a small percentage answered questions with the response ‘I don’t know’ (selected a maximum of four times for a particular question (6.7%) or ‘not applicable’ (selected a maximum of nine times (15%) for a particular question (‘How satisfied are you with the process of identifying your top three self-management goals?’)). Results provided are for those who answered with a satisfaction level (figure 1). On a 5-point Likert scale from ‘not at all satisfied’ to ‘extremely satisfied’, the median (IQR) level of satisfaction with the overall visit was 4.0 (4.0, 5.0). Twenty-one (36%) patients were ‘extremely satisfied’, 34 (59%) patients were ‘quite satisfied’, 1 (1.7%) was ‘moderately satisfied’ and 2 (3.4%) were ‘slightly satisfied’. The results from Cronbach’s α coefficient show a strong internal consistency among the seven items related to satisfaction (α=0.79, 95% CI 0.71 to 0.86), hence suggesting internal validity of the satisfaction measurements.
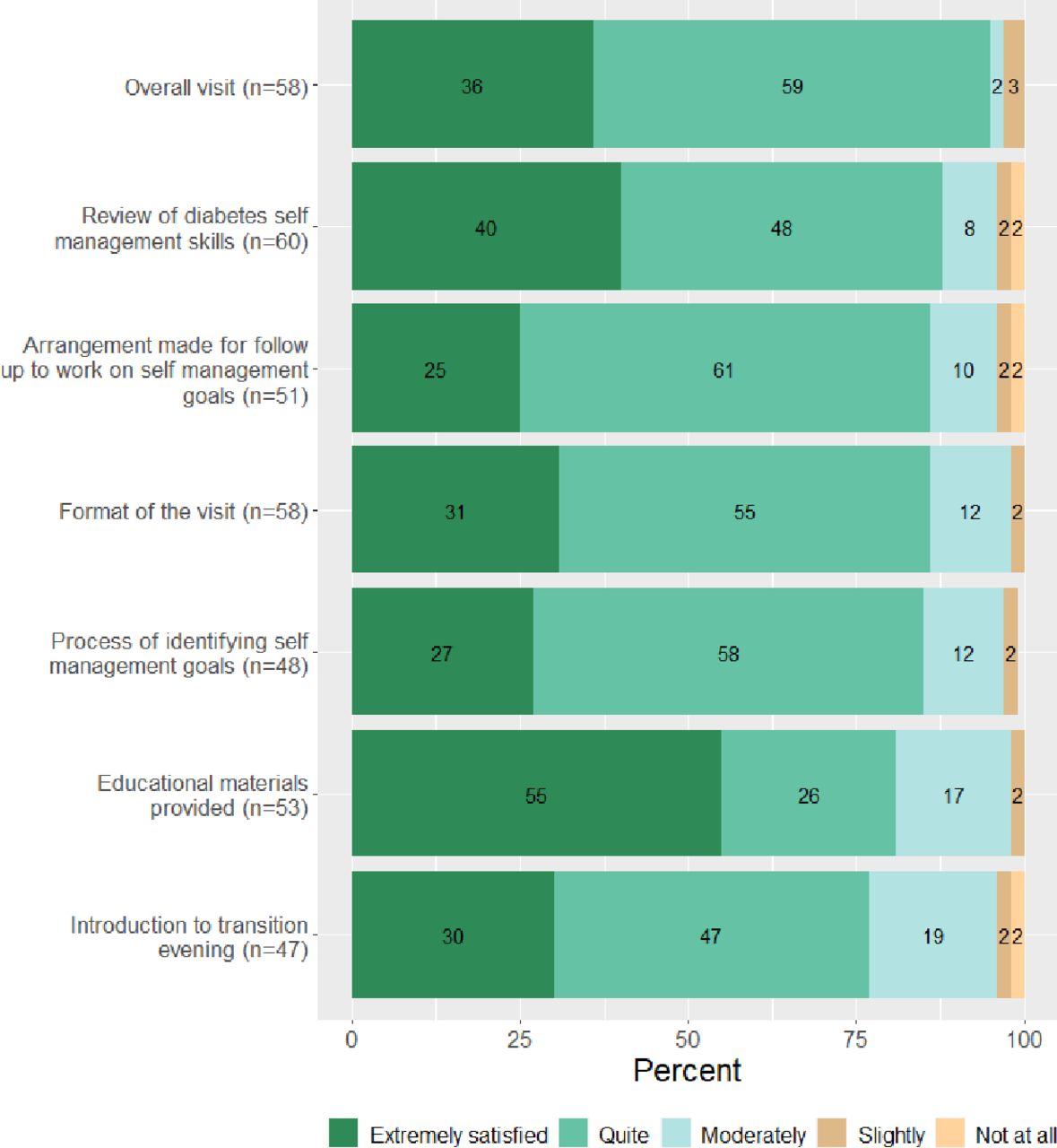
Patient satisfaction with aspects of the Pre-Transition Visit.
Only patients who answered all six of these satisfaction items using a satisfaction level were included (39/60). Those who responded ‘I don’t know’ to any of the six items were removed from this specific analysis. The median (IQR) of the composite score was 25.0/30 (24.0, 26.5).
There was a negligible decrease in satisfaction level associated with higher A1C level and longer disease duration. A small increase in satisfaction was also observed for older patients and for females. These differences were not statistically significant nor felt to be clinically significant (table 2).
Multivariable modelling of overall patient satisfaction with the Pre-Transition Visit
Patient-reported relevance of the visit
For questions in the relevance section of the survey, the answer ‘I don’t know’ was selected a maximum of seven times for a particular question (13%), and the answer ‘Not applicable’ was selected a maximum of nine times (15%) for a particular question. Results are provided for those who answered with a relevance level on a 5-point Likert scale ranging from ‘not at all relevant’ to ‘extremely relevant’, for various components of the Pre-T Visit (figure 2). In terms of internal validity related to relevance items, the estimated α coefficient shows a moderate to good level of internal consistency (α=0.57, 95% CI 0.40 to 0.74).

{kind=link}
{kind=link}
Patient-reported relevance of aspects of the Pre-Transition Visit to their needs.
Patient engagement
Patients were asked how much they participated during the Pre-T Visit on a scale from ‘I did not participate at all’ to ‘I participated a tremendous amount’. The majority (92%) reported participating ‘quite a bit’ or ‘a tremendous amount’, and 6.7% reported participating ‘a little bit’ or ‘some’. Patients were also asked at which age they thought the Pre-T Visit would be most relevant. Fifty-five (92%) selected 16 years and over, of which 43% answered 16 years exactly. Five (8.3%) answered 15 years and under.
Caregiver responses
Twenty-seven caregivers/parents completed the survey following the visit summary, of which 93% were ‘extremely satisfied’ or ‘quite satisfied’ with the Pre-T Visit, and 7.4% were ‘moderately satisfied’. The majority of caregivers (89%) found the Pre-T Visit summary to be ‘extremely relevant’ or ‘quite relevant’ to the patient’s needs and 78% found it ‘extremely relevant’ or ‘quite relevant’ to the family’s needs, while 11% and 22% of caregivers found it ‘moderately relevant’ or ‘slightly relevant’ to the patient and family’s needs respectively.
Discussion
Overall, we found that both patients and their families had high levels of satisfaction with the Pre-T Visit which reinforced this as a good use of resources (ie, patient, administrative and educator time) in our clinic, with respect to the patient experience. These findings were consistent across patients despite differences in age, gender, diabetes duration and A1C. Furthermore, patients reported high levels of engagement/participation in the visit. The preferred age to conduct this visit was 16 years or older. Importantly, the sample of patients who underwent and evaluated the Pre-T Visit was representative of our overall clinic population as seen in table 1.
Our findings of high levels of satisfaction are consistent with results of other studies evaluating transition-related initiatives but direct comparisons are difficult due to small sample size20 and heterogeneity in type of intervention.21 In larger studies, patient satisfaction was rarely the primary outcome21 22 and when it was evaluated, it was usually satisfaction with overall care rather than with the specific study intervention/tool.22 We evaluated patient-reported satisfaction with a specific transition-related intervention as our primary outcome using a comprehensive survey. Patient experience and satisfaction are critical components of any sustained quality improvement interventions.36 37 Moreover, they are increasingly recognised as important outcomes since they have been shown to be linked to patient outcomes and patient safety.37 Our findings support the acceptability of the Pre-T Visit, though further patient follow-up would be required to conclude that it resulted in improved health outcomes, such as improvement in glycaemic control.
While the Pre-T Visit provides an opportunity to systematically introduce the concept of transition and identify gaps in knowledge and management skills, it does not, in itself, address these gaps. Therefore, other interventions must be incorporated into routine diabetes care to accomplish this. In our clinic, we recently implemented a separate quality improvement initiative aimed at increasing confidence and competence in diabetes self-management skills; a partner to the Pre-T Visit. Youth with T1D who are age 13 years or older attend the DLC immediately prior to their physician visit where they work on various self-management skills with customised worksheets to support this learning. Once gaps in management are identified at the Pre-T Visit, DLC visits can be used to address these gaps. A separate evaluation of the DLC including the assessment of patient-reported change in confidence in diabetes-related knowledge and visit satisfaction is underway. The DLC was implemented after the Pre-T Visit, however, now that the infrastructure is in place to address self-management skill gaps, the importance of delivering the Pre-T Visit by age 16 years is greater to allow time to systematically address the gaps.
There are limitations to this study. First, our study has a smaller sample size than originally intended due to the suspension of Pre-T Visits at the start of the COVID-19 pandemic. However, we were still able to conduct a complete analysis and draw important conclusions from our data. Based on collected clinical information, participants were representative of our overall clinic population, but important demographics related to social determinants of health were not collected and could limit internal and external generalisability. While the response rate of youth who participated in the programme was high, significantly fewer parents and caregivers completed the survey. Our impression is that clinic time constraints impacted parent/caregiver survey completion. By the time they were asked to complete the survey, their youth had already spent time with educator, time completing the survey and the visit with physician was still upcoming. The validity and reliability of conclusions drawn from parent/caregiver perspectives are therefore limited due to small sample size and possible selection bias. Since this visit was introduced as a quality improvement initiative embedded in standard diabetes care aligned with international guidelines in providing ‘comprehensive expert-structured education’ that is continuous and repeated, easily accessible, adaptable and able to be personalised, to all patients within our diabetes clinics,38 we did not have a control group consisting of patients who did not attend a Pre-T Visit. While patient satisfaction with the Pre-T Visit was high in our study, without a control group, we cannot draw conclusions about the impact of the Pre-T Visit on overall satisfaction with care. Finally, while a comparison of A1C pre-Pre-T Visit and post-Pre-T Visit was planned, this was not possible due to the COVID-19 pandemic. During the pandemic, most participants did not have A1Cs measured due to limited visits to the hospital and/or laboratories. Furthermore, the impact of the pandemic on glycaemic control would have been a confounder.
Given the high levels of patient and family satisfaction and relevance of the Pre-T Visit, we plan to continue to offer Pre-T Visits as part of routine care, ideally at age 16 based on the respondents stated age preference. This timing also allows the subsequent 2 years in paediatric care to be focused on closing gaps in diabetes knowledge and self-management skills and addressing transition-related issues. Given that in our study the average age at Pre-T Visit was 16.7 years, we will adjust our clinic procedures to try and achieve the target age of 16 years. Furthermore, now that the DLC is implemented, several elements of transition preparation can be addressed prior to the Pre-T Visit which may allow for more personalisation, consolidation and focus in the 2 years leading to transition.
During the COVID-19 pandemic, our clinic converted all of our routine T1D-related visits to virtual and we plan to continue to deliver the majority of diabetes follow-up care this way. Due to necessary pandemic-related restructuring (eg, to address staff shortages due to redeployment), certain diabetes care services, including Pre-T and DLC Visits, were temporarily put on hold. We are currently in the process of reinstating these visits in a primarily virtual format (with in-person alternatives for patients unable to access virtual technology). Virtual Pre-T Visits will allow for greater flexibility in scheduling as they would not need to be tied to an in-person clinic visit. While telemedicine delivery of care for adolescents with T1D has been shown to be effective,39 40 we need to evaluate its use for the delivery of Pre-T Visits to ensure patient satisfaction or relevance is not compromised. Since we were able to sustain the Pre-T Visit in our clinic for over 2 years prior to the pandemic, we feel confident that, once re-established as part of our virtual diabetes care programme, it will be sustainable long-term. Similar to our initial Pre-T Visit design, the implementation of virtual Pre-T Visits will be integrated within our restructured diabetes programme. We acknowledge that Pre-T Visits require educator time that draws from time otherwise used toward other facets of our programme, however, through routine, focused evaluation of our patients’ transition readiness, we anticipate time saving by reducing need for urgent and last-minute education. Duration adequacy of Pre-T Visit was not formally evaluated but diabetes educators reported that 45 min was sufficient.
Although optimal patient experience is integral to high-quality diabetes care, it is also important to measure the impact of quality improvement interventions on quantitative health outcomes including measures of glycaemic control (A1C and glucose time in range) and diabetes complications. Transition-related interventions with high levels of satisfaction with care do not always translate into improved glycaemic measures.22 Once Pre-T visits are restarted following the hold due to the pandemic, we aim to evaluate their impact on glycaemic control and the patient experience using qualitative methods, such as a patient focus group. Other important outcomes to quantify include timely attendance at adult diabetes visits and diabetes-related emergency visits and hospital admissions. Finally, our diabetes care delivery model is undergoing restructuring to ensure that the Pre-T Visit can work synergistically with other quality improvement initiatives, such as the DLC described above, to better prepare youth with T1D for their transition.
Conclusion
A novel Pre-T Visit was rated highly by youth and their parents with regards to visit satisfaction and relevance. This new type of visit is a feasible first step to implementing a programme to address existing recommendations to improve transition care without added costs or resources and has potential to impact short and long-term health outcomes. We expect the impact of this improvement to be greatest when combined with other quality improvement initiatives focused on preparing youth for transition—many of which can be delivered virtually as the current pandemic necessitates.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the manuscript or uploaded as supplementary information (questionnaires). Additional data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but CHEO Research Ethics Board exempted the study from requiring REB approval as it was deemed quality improvement. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank Alicia Klassen for her support as a research assistant, Kaylee Eady, PhD, for support with the methodology and survey development, and Dr Marie-Eve Robinson for critically reviewing our manuscript. We would also like to thank the diabetes educators who led the Pre-Transition Visits, as well as the patients and families who participated in the study. Finally, we would like to thank the CHEO Research Institute for the Resident Research Grant awarded to AM, which funded the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AM designed the study with EBG, contributed to patient recruitment, led the data acquisition, drafted the initial manuscript, interpreted the data, revised the manuscript and produced the final version of the manuscript with EBG. AT led the data analysis with JSH, helped interpret the results, revised the manuscript and approved the final version for publication. JC contributed to development of the study protocol, revised the manuscript and approved the final version for publication. JSH contributed to development of the study protocol and developed statistical analysis plan, led the data analysis with AT, helped interpret the results, revised the manuscript and approved the final version for publication. JS-D-M and LS contributed to development of the study protocol, led participant recruitment and contributed to data acquisition. They revised the manuscript and approved the final version for publication. AA provided input into the implementation of the Pre-Transition Visit, revised the manuscript and approved the final version for publication. EBG led the development and implementation of the Pre-Transition Visit with JS-D-M and LS with input from the CHEO diabetes team, designed the study with AM, interpreted the data, revised the manuscript critically for important intellectual content and produced the final version of the manuscript with AM. EBG is responsible for overall content as the guarantor.
Funding AM received a Resident Research Grant through the Children’s Hospital of Eastern Ontario (CHEO) Research Institute.
Competing interests The authors declare that the following financial interests/personal relationship which may be considered as potential competing interests: AA and EBG are coinvestigators for the Medtronic study entitled 'Multi-center, Randomized, Parallel, Adaptive, Controlled trial in Adult and Pediatric Patients with Type 1 Diabetes Using Hybrid Closed Loop System and Control (CSII, MDI, SAP) at Home'. Medtronic provided funds to cover the cost of supplies and research staff time for this study, but investigators did not receive payment. LS is receiving payment as research staff for the Medtronic study entitled 'Multi-center, Randomized, Parallel, Adaptive, Controlled trial in Adult and Pediatric Patients with Type 1 Diabetes Using Hybrid Closed Loop System and Control (CSII, MDI, SAP) at Home'. JS-D-M is receiving payment from Tandem and Medtronic for her role as an insulin pump educator.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.