Article Text

Statistics from Altmetric.com
Introduction
Aspiration is the inhalation of oropharyngeal or gastric content into the respiratory tract.1 The consequent clinical pattern depends on the patient’s response, the quantity and frequency of aspiration, and the presence of pathogens. Two main clinical syndromes ensue. First, aspiration pneumonitis from chemical lung injury by sterile acidic gastric content, usually associated with patients with a reduced conscious level,2 and aspiration pneumonia from inhalation of colonised oropharyngeal material resulting in an inflammatory response to the bacteria. Many healthy individuals aspirate small amounts, mainly when asleep, that are cleared by ciliary transport, coughing and other lung defence systems.3 Aspiration pneumonitis or pneumonia (AP) usually occurs when those mechanisms are impaired, for example, by cerebrovascular disease, or overwhelmed by aspiration at higher volume.1 4 Optimal care of patients at risk of AP requires a multidisciplinary team approach5 involving individualised assessments and actions by doctors, nurses, speech and language therapists (SALTs), physiotherapists and others.
This Trust received an alert in 2015 from Care Quality Commission/Dr Foster system indicating that deaths in the category involving AP in 2012/2013 and 2014/2015 were higher than expected after standardisation.6 This prompted a structured retrospective mortality review (SRMR) in 2015, corrective actions, and further SRMRs in 2018 and 2020. As a subset of the Trust’s wider mortality review data were collected salient to AP. This initiated three plan–do–study–act (PDSA) cycles aimed at improving AP mortality, the processes and results of which are the topic of this paper.
Methods
Three SRMRs were performed in 2015 (2011/2012 AP data), 2018 (2016/2017 AP data) and 2020 (2018/2019 AP data). Patient data were identified through the Trust audit office and from Dr Foster. Each patient’s coding and death certificate were reviewed to determine whether they met the criteria for AP. Included cases were assessed against agreed criteria encompassing medical, nursing and other clinical care, SALT assessment and actions, and communication with the patient and family. Interventions based on extant best practice standards5 were implemented in order to reduce deaths due to AP.
Interventions
The initial PDSA (2015), in response to the first SRMR, altered nursing care, emphasising feeding in a more upright position. Other measures included training by SALTs of ward staff on feeding and mouth care, the appointment of ward mouth care champions, training in safe feeding for healthcare assistants during their induction and adherence to Trust antibiotic policies. The second PDSA (2016), focused on timely SALT input, including at weekends, through online referral enabling two times per day triage. This was achieved through a business case for weekend SALT services. A personalised feeding-at-risk (FAR) proforma was produced containing the rationale for FAR decisions and advice on optimum food and drink consistency. This reduced ambiguity of care so subsequent clinicians would be clear about the feeding plan. The third PDSA (2017) aimed to improve communication between hospital and community SALT teams through using the discharge summary as a multidisciplinary document.
Results
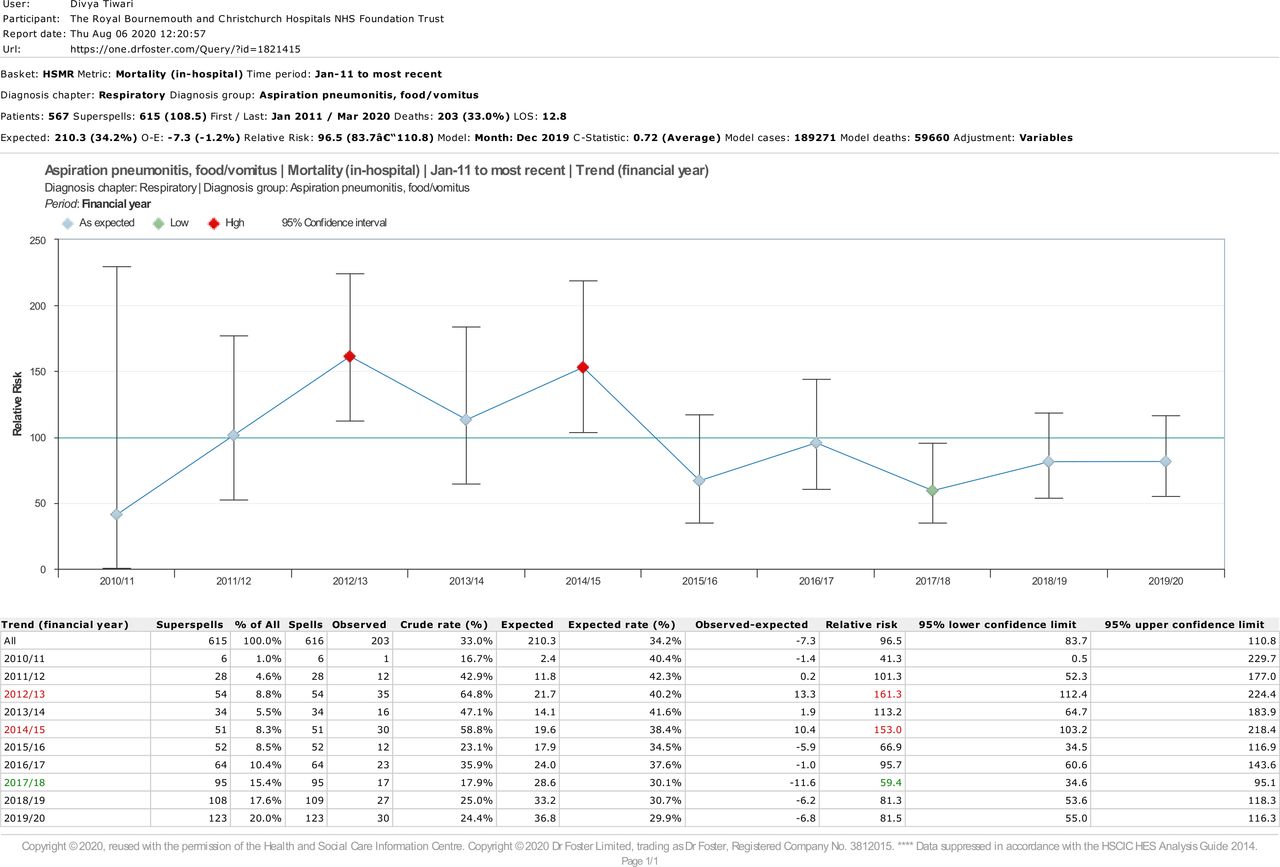
The Dr Foster mortality data for AP from 2011 to 2020 are shown in figure 1. Alerts were triggered in 2012/2013 and 2014/2015, with a relative risk of mortality of 161 (95% CI 112 to 224) and 153 (95% CI 103 to 218), respectively. The Trust’s AP mortality fell after the initial interventions to 67 (95% CI 35 to 117) in 2015/2016 and has remained below the national average for 5 consecutive years.

{kind=link}
Graph depicting Dr Foster mortality data for this hospital from 2011 to 2020. Diagnosis group: aspiration pneumonitis, food/vomitus. Copyright Dr Foster Limited, registered company number 3 812 015.
SRMR findings
In 2015, 15 AP deaths met the inclusion criteria. Eleven had conditions predisposing to dysphagia. Of these, two patients had documented community feeding plans. Data were scanty with regard to SALT review, but of the five patients in which this was intended, only one was referred. No FAR conversations were documented.
In 2018, 10 deaths were confirmed in the AP category. Eight had conditions predisposing to dysphagia, all of whom were reviewed by SALT within 24 hours of referral. One was not referred, and one was too drowsy for assessment. All but one were referred on day 1 or 2 of admission. FAR discussions were held in all but one.
In 2020, nine AP deaths met the criteria. All were reviewed by SALT within 24 hours except one who died soon after admission. Five had pre-existing dietary modifications. Of the patients reviewed by SALT, only two did not have a documented FAR conversation.
Discussion
Aspiration increases morbidity and mortality. The early assessment and active Multidisciplinary Team management we initiated at the first SRMR-guided PDSA were associated with a reduction in mortality from AP with sustained improvement associated with the further two PDSA cycles. The critical success factor appeared to be the collaborative MDT approach, focusing on nursing care, communication, early referral and early decision making. Though the number of patients was low, the clear temporal relationship between the interventions and the sustained improvement suggests a real effect and illustrates the utility of SRMR to generate information and PDSA to achieve change. Many of the patients had comorbidities associated with dysphagia, so perhaps a further PDSA could test the benefit of formal swallow assessments for all such patients, resources allowing, even if they present with no apparent aspiration.
Limitations
Mortality ratios were monitored to evaluate the improvements. Therefore, direct attribution is not possible, although plausible.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Footnotes
Contributors DT: lead investigator and Trust mortality lead. RK, SR-T: coinvestigators and specialist registrars. MW: coinvestigator and speech and language therapist. SA: professor and senior investigator.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.