Article Text

Abstract
Setting Based at a busy city hospital, the alcohol care team is a drug and alcohol specialist service, taking referrals for a wide range of patients with substance use disorders (SUD).
Objectives Patients with SUD are at high risk of vitamin D deficiency; this relates to frequent fractures and proximal myopathy. The coronavirus pandemic brought vitamin D into focus. Local guidelines advise that patients at high risk of vitamin D deficiency are offered replacement. There were no local data on vitamin D deficiency prevalence or any mention of patients with SUD in local vitamin D guidelines. The main aim of this project was to offer vitamin D checks and replacement to all appropriate patients.
Results We collected data on 207 patients, [pilot study (n=50) and two subsequent samples (n=95 and n=62)]. Our pilot study showed that no patients were offered vitamin D testing or replacement. We then offered vitamin D checks to 95 patients. Most had low vitamin D (30 patients were vitamin D deficient and 26 were vitamin D insufficient). We provided vitamin D replacement and follow-up advice. Quality improvement was demonstrated 6 months later. We collected data on a further 62 patients who were all on our current or recent caseload. Following exclusions, nearly half (48%) of patients had had a vitamin D check. Almost all of these (95%) had low vitamin D (60% being classified as deficient).
Conclusions Patients had not been offered vitamin D replacement despite often having multiple risk factors for vitamin D deficiency. Vitamin D checks (and subsequent replacement) rose in frequency since the outset of this project. Local guidelines should add SUD as a risk factor for vitamin D deficiency. Hospital admission provides a rich opportunity to offer this simple intervention to patients who are often poorly engaged with community services.
- mental health
- harm reduction
- hospital medicine
- quality improvement
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The coronavirus pandemic brought vitamin D into focus due to its potential role in reducing severity of respiratory tract infections.1–5 There is currently no conclusive evidence that vitamin D deficiency predisposes to coronavirus, however, evidence supports the role of vitamin D in prevention of acute respiratory infections.6 The alcohol care team (ACT) were alerted to a health-promotion intervention at South London and Maudsley National Health Service Foundation Trust (SLaM) at the start of the pandemic, where vitamin D replacement was provided to inpatients with schizophrenia, who are at high risk of vitamin D deficiency.7 This prompted the team to investigate whether their patient group may be similarly at risk.
We defined vitamin D status in table 1.
Vitamin D ranges21 23
We found evidence to support vitamin D deficiency being prevalent in patients with substance use disorders (SUD). Cross-sectional studies of non-cirrhotic patients with alcohol dependence in addiction services in France demonstrate that between 41% and 90% have vitamin D levels below 12 nmol/L.8–10 In those with fatty liver or liver fibrosis, the prevalence of severe deficiency is 60.4%.11 Alcohol dependence is an independent risk factor for adult respiratory distress syndrome and may worsen outcome.12 Many opioid dependent patients smoke and a large proportion (30.3%) have chronic obstructive pulmonary disease which makes them more vulnerable to COVID-19.13 US data indicate that patients with opioid dependence have high rates of deficiency (36%) and insufficiency (52%)14 with some populations reporting a mean vitamin D level of 5.2 nmol.15 We found no UK data on vitamin D deficiency prevalence in SUD.
A UK study published in October 2021 on mortality in people with mental disorders, showed elevated standardised mortality ratios (SMR) for all mental disorders (including SUD) with COVID-19.16 For all other causes of death (not due to COVID-19), the SMR increased for patients with SUD to 5.1 (95% CI 4.3 to 5.9) during the pandemic (second quarter of 2020) when compared the same quarter of 2019 (SMR 3.7, 95% CI 3.2 to 4.7).16 A US study suggests that individuals with SUD are both more at risk of becoming infected with COVID-19 (OR of 8.7 with CI of 8.4 to 9.0) and more at risk of worse outcomes after becoming infected than the general population.17
It is clear that vitamin D is vital for maintaining bones and muscle function. Complications of low vitamin D in adults result in increased risk of fractures, secondary to osteomalacia and proximal muscle weakness (an independent risk factor for frailty, falls and fractures),18 likely contributors to frequent attendances at emergency departments (ED) and hospital admissions.
In light of significant morbidity resulting from vitamin D deficiency, the addictions management group decided to evaluate how we are investigating and treating vitamin D deficiency. This was less feasible in the community where face to face contact was minimised but more actionable in the general hospital setting.
Clinical innovation
Our team is multidisciplinary and based in a busy London teaching hospital and receives referrals for inpatients with concerns around substance use, for example, alcohol withdrawal, delirium tremens, opioid withdrawal and gamma-hydroxybutyrate-induced psychosis. Its position in a general hospital means that the barriers to accessing vitamin D testing and initiation are low. Contact with the ACT is thus a premium opportunity for screening and harm minimisation and can pave the way for wider service implementation.
Aims
To establish a method for offering vitamin D level checks to all appropriate patients on our caseload.
To use patients’ general hospital admission as an opportunity to intervene, that is, to offer vitamin D replacement and follow-up to appropriate patients.
Background
A recent review of evidence assessing vitamin D status and vulnerability to coronavirus infection found no direct evidence related to vitamin D deficiency predisposing to coronavirus.11 However, it did state that current advice is that the whole population of the UK should take vitamin D supplements to prevent vitamin D deficiency, irrespective of any possible link with respiratory infection. The review concluded that clinicians should treat patients with vitamin D deficiency regardless of any link with respiratory infection.11
Our hospital guidelines state that individuals at particular risk of vitamin D deficiency should be offered routine replacement treatment. They also advise that patients with the combination of one or more risk factors for vitamin D deficiency as well as symptoms/signs of vitamin D deficiency should be offered a vitamin D level check. Local and national guidelines suggest that everyone living the UK should take daily over-the-counter vitamin D supplements of 10 µg/400 IU between October and March.19 20
Risk factors for vitamin D deficiency listed in the local guidelines are numerous, including deranged liver function and ‘mental health conditions’. Nevertheless, they do not explicitly mention SUD. This omission is contrary to evidence already referenced, in that being a patient in addictions services is itself a risk factor for vitamin D deficiency.
Symptoms and signs of vitamin D deficiency are non-specific and can be easily missed. Vitamin D levels are easy to check with a simple blood test. Replacement of vitamin D is straightforward, safe and inexpensive.
Measurement
To establish a baseline measurement of current practice around vitamin D level checks and replacement, we carried out a pilot project of 50 patients. This sample of 50 patients was taken from our team’s current handover list and recent patient discharge list, in the order in which they were referred to us. A spreadsheet was kept with patient details and hospital clinical records were reviewed. It allowed us to ascertain whether patients were already being offered vitamin D checks or replacement in line with local hospital guidelines.
The results of our baseline measurement showed that none of the 50 patients in the pilot study were offered vitamin D level checks or replacement during their inpatient admission, despite often meeting criteria on local guidelines for vitamin D replacement and/or level checks.
We started our first cycle of quality improvement (QI) by raising awareness of vitamin D testing within our own team and on hospital wards, as well as actively requesting vitamin D levels checks by immunoassay. We extracted patient data and recorded vitamin D level results on a spreadsheet. We used the patient total number of 95 as an arbitrary cut-off point to analyse our results.
Six months later, in our second cycle of QI, we collected data on 62 patients. This final sample of 62 patients was selected as a representative sample of patients on our current handover list and list of recently discharged patients, again in the order which they were referred to us. The risk of bias in selection of patients was reduced by taking patients directly from team patient lists sequentially.
We listened to feedback and decided not to include patients who were in the acute phase of illness for vitamin D testing. We also noted that it was not practical to include patients who were in the ED and not admitted to hospital wards. The following inclusion and exclusion criteria were established after learning from our pilot study:
Inclusion criteria
Patients admitted to hospital.
Referred to, and accepted by the ACT.
On ACT current caseload or recent discharge list.
Exclusion criteria
ED patients.
Acute phase of illness (eg, alcoholic hepatitis).
Intubated patients.
Intensive care or high-dependency units.
End-of-life/palliative care.
We prescribed vitamin D replacement, including a high loading dose for patients that were deficient and a replacement dose for those that were insufficient in vitamin D status. For aftercare, we devised a letter template to send to the patients’ general practitioner (GP) with requests for follow-up blood tests at 4 weeks and 3 months (as per local guidelines).
Design
We undertook data collection in conjunction with patients referred to our team between June–August 2020 and November 2020–January 2021. We initially planned to advocate universal prescription of a loading dose of vitamin D in a similar manner to that advocated by our partnering mental health trust. Significant differences existed between the two trusts however, for example, the acute hospital had experienced recent incidences of hypervitaminosis, had a more physically acutely unwell patient population and had easy access to vitamin D testing. In contrast, the mental health trust had patients who were generally more physically well, frequently declined blood tests on admission and had no laboratory on site to carry out vitamin D tests. We agreed that all patients admitted to our acute hospital site could have a vitamin D level check, with vitamin D replacement, if required.
Advice was sought from junior doctors on the logistics of requesting routine vitamin D level checks. Vitamin D status was added to our team’s handover list, which involved all team members in requesting and chasing results of vitamin D levels.
Medical colleagues from a range of specialties were involved in discussions about this QI project. We took into account their views that vitamin D intervention was more appropriate for general practice rather than acute hospital admission. However, patients with SUD often struggle to attend generic services, to the extent that screening for other health conditions, for example, Hepatitis C is conducted in addictions services and at needle exchanges.
We did not include patients who had a low chance of surviving the admission. We also excluded patients who were referred to our team for review in ED only, as patients had often left ED by the time vitamin D level results were ready. The opportunity to issue outpatient prescriptions from the ED is limited.
Strategy
Our stages for improvement began with assessing current clinical practice with respect to vitamin D checks and replacement. We found that 0 out of 50 patients had a vitamin D level check and no patients were offered routine vitamin D replacement. This was not concordant with our local guidelines, which advise vitamin D level checks be offered to all patients with risk factors for low vitamin D and symptoms or signs of low vitamin D. Routine maintenance dose vitamin D replacement, without vitamin D level checks was also not being offered to patients with risk factors for low vitamin D, which was also not in keeping with local guidelines.
We adapted our handover list to include a column on vitamin D, stating if a level had been requested, when the level was due and if replacement was needed.
We reflected on the issues of patients being discharged before the vitamin D level could be checked. We decided to omit patients who only attended ED who were not admitted to wards.
In order to increase awareness of vitamin D testing and start further discussion, we ran teaching sessions within our team. We discussed vitamin D levels regularly at our team handover meetings and team members began requesting vitamin D levels and raising awareness of vitamin D deficiency and its consequences with ward teams.
Six months after the outset of this project, we collected another round of data from 62 patients. This was to assess if QI had been sustained and gauge whether vitamin D level checks and replacement had been embedded into routine clinical practice by both our own team and, more broadly, to acute hospital ward teams.
Results
SUD was not listed as a risk factor for vitamin D deficiency on our hospital protocol.
Our pilot study of 50 patients referred to the ACT showed that none of these patients were offered vitamin D testing, despite sometimes having other documented risks for vitamin D deficiency.
In our first QI cycle, we attempted to check vitamin D levels in 95 patients (in summer).
In our second QI cycle, we reassessed vitamin D level checks (in winter) for 62 patients. Patients were selected in the order they appeared on the team’s handover lists. An overview of our data collections rounds is summarised in table 2.
Data collection rounds overview
In our second round of data collection, we found vitamin D levels were abnormal in the majority of patients checked: 60% of patients (57/95) had a vitamin D level outside normal limits, almost all (56/57) having low vitamin D: 26 patients with vitamin D insufficiency and 30 patients with vitamin D deficiency.
Twenty-two patients (23% of the sample) had a ‘normal’ vitamin D result, and only one patient (1% of the sample) had a high vitamin D level (and, at 181 nmol/L, still well below the range for vitamin D toxicity). Sixteen patients (17% of sample) were discharged before their requested vitamin D check could be carried out (figure 1).

Vitamin D results breakdown for round 2 (blue) and 3 (red). Pilot data (n=50) and patients discharged without results omitted for clarity.
The majority (95%) of patients in our third round had low vitamin D, (60% of patients were vitamin D deficient and 30% insufficient). Only one patient had vitamin D within normal limits and no patients had a high vitamin D level (figure 1).
These results enabled us to offer vitamin D replacement at a loading dose of 20 000 units (500 µg), two times per day for 7 days, to vitamin D deficient patients.
Once vitamin D results came back as deficient, often medics or pharmacists on the patient’s ward intervened and prescribed appropriate vitamin D replacement without prompting.
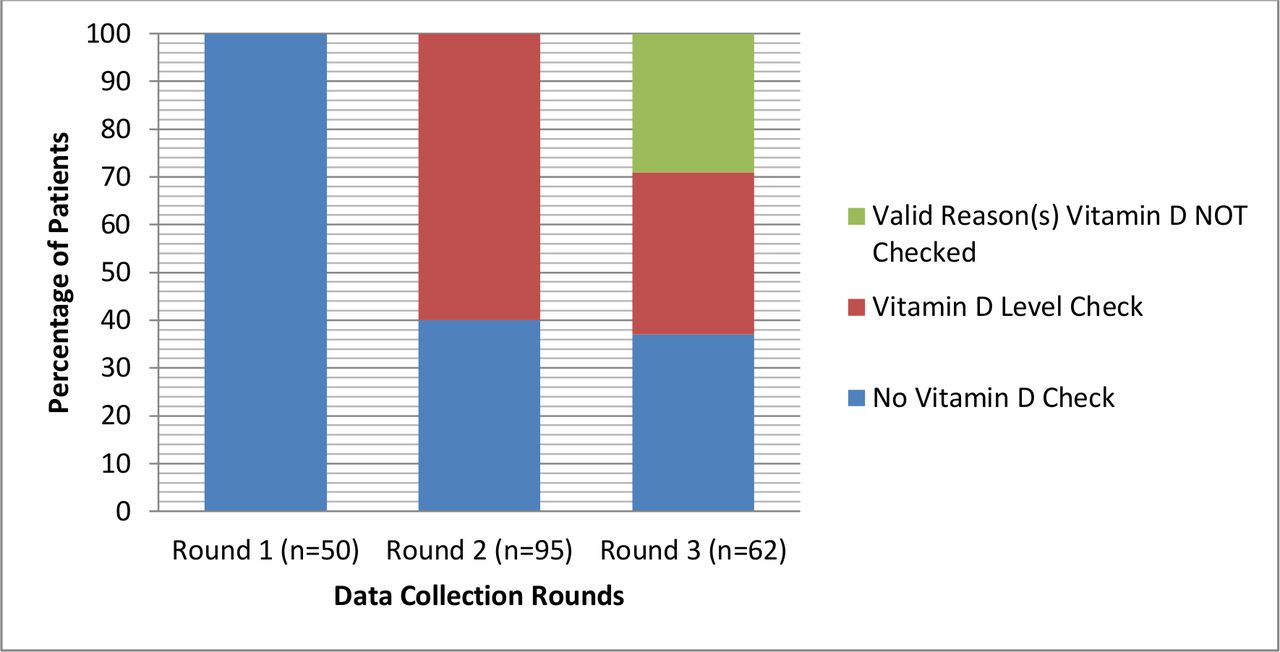
We compared our three data collection rounds (figure 2). No patients were found to have been offered a vitamin D level check in our pilot study. This significantly improved in round 2, when we began actively requesting vitamin D level tests and raising awareness.
{kind=link}
{kind=link}
Comparison of vitamin D level checks between data collection rounds (round 1 = pilot study).
The purpose of our final round of data collection (round 3, 6 months after round 2) was to assess whether vitamin D monitoring had been embedded into the clinical practice.
In round 3, we found 21 patients had vitamin D level checks. Eighteen patients were not eligible for vitamin D level checks due to being only seen in the ED or being in acute phase of illness (eg, being treated in intensive care). The remaining 23 patients did not have a vitamin D level check.
With exclusions removed, this most recent sample (round 3) showed that almost half of patients (48%) were offered a vitamin D level check. This in an improvement, compared with our pilot study, which showed that 0/50 patients were offered a vitamin D level check (figure 2).
Lessons and limitations
A limitation of this project was the lack of linking our discharge template to the patient’s GP requesting appropriate follow-up blood tests at 4 weeks (patients who received vitamin D loading)21 and 3–6 months21 22 with each patient’s hospital discharge letters. This did not happen routinely within our team due to time constraints and fast patient turnover. A lesson learnt, and which should form the basis of a follow-up project is the need to audit discharge letters of patients prescribed vitamin D during inpatient stays and assess if the information in our template is present on hospital discharge summaries. Patients not admitted for the duration of vitamin D loading doses should have been discharged with vitamin D ‘to take away’. We do not have any data on how many of our patients attended for follow-up blood tests.
The research published to date on vitamin D deficiency and substance use has mainly focused on people with alcohol23,8 9 or opioid dependence.13 We accept that our patient sample is heterogeneous, incorporating a range of SUD, including polysubstance use.
The initial approach of blanket checks of vitamin D levels for all of our patients with hindsight was not the correct approach. It emerged during the project that some patients were not appropriate for vitamin D levels checks. We addressed these issues by reviewing case notes briefly prior to requesting vitamin D level check (to rule out hyperacute phase of illness) and excluded patients in ED, as there was not enough time to test and prescribe for these patients.
Initially, some vitamin D results were not pursued due to different team members being present on different days. A lesson learnt was to add a column to our team handover list which allowed all team members to be aware if there were outstanding vitamin D level checks to be followed up on.
The cost of vitamin D checks (≈£25 each) is significant. When the test is more expensive than the treatment, it must be questioned whether blind prescription of vitamin D is a better course of action. If we had adopted an initial strategy of prescribing and dispensing a loading regimen at first contact without testing, it is likely that our coverage would have been wider. The workload was undoubtedly higher because of the need to request testing and check the results.
Knowing a patient’s exact vitamin D level is useful as it informs clinicians on the optimum vitamin D dose for each individual patient. There is a stark contrast between the high dose needed to comprehensively treat very low vitamin D levels and the more modest supplementation for patients with milder vitamin D insufficiency.
The risk of overtreating patients is slim, but still must be considered in light of the potentially serious and irreversible cardiovascular and renal toxicity that can result from hypervitaminosis. One patient was found to have a high level of vitamin D and it later emerged that he had been taking over-the-counter supplements prior to admission. We cannot be sure that harm (damage from hypercalcaemia) would not have resulted from blindly loading this one patient with vitamin D. Safety could be improved by asking patients directly if they are taking over-the-counter vitamin supplements.
This QI project was carried out prior to the current UK national blood specimen bottle shortage. In August 2021, NHS England issued advice on reducing non-clinically urgent blood tests and specifically recommended that vitamin D testing is temporarily stopped, except in ‘very exceptional circumstances’.24
There was some disagreement between colleagues whether inpatient general hospital was the appropriate setting to address vitamin D deficiency, proposing that the responsibility for this should instead lie with general practice. A lesson learnt is for us all to recognise that, for this disadvantaged patient population who frequently have poor relationships with healthcare, hospital admission provides a rare opportunity to address these common physical health issues. Indeed, the patients we see are often poorly engaged with community services.
Conclusion
This project considered international evidence and examined local data, identifying that vitamin D is indeed low in our patient group. A large number of our patients are severely low in vitamin D, which can have serious implications for health and quality of life.
Vitamin D deficiency is straightforward to treat. The potential for lowering patients’ risk of serious medical complications and prolonged hospital stays is likely to outweigh the low cost of offering testing and replacement of vitamin D routinely to our patients.
Our project highlights that patients are not being offered vitamin D level checks or replacement, even when they do meet local criteria for this test and important treatment. There was an improvement in vitamin D level checks (and subsequent vitamin D replacement) in our first and second cycle of QI.
It is of note that patients with SUD are not mentioned in our local guidelines on vitamin D, despite significant evidence to suggest this population is particularly at risk. We are currently negotiating with local prescribing governance structures to change this.
Testing for and treating vitamin D deficiency is frequently overlooked as it is not considered an acute medical problem. However, one of the key functions of an ACT is to prevent repeated admissions. As falls, fractures, and respiratory infections are common precipitants of hospital admission in this patient group, we perceive identifying and treating vitamin D deficiency as an important part of this endeavour.
We conclude that acute hospital admission provides an important opportunity to provide holistic care, identify and offer treatment to our patient population, who are very often vitamin D deficient and poorly engaged with non-acute services. Addressing vitamin D deficiency and initiation of prophylaxis need to be recognised as essential element of good clinical care. We advocate for this simple intervention to be incorporated into clinical practice.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
We would like to thank Mr. Alexander J. Horn, Ms. Becci Connolly and Ms. Margarita Bela for their support.
References
Footnotes
Twitter @KalkNicola
Contributors All authors listed have contributed to this submission. Project initiation (NJK), preliminary discussions (NJK, JS, DT, FG, EF and SG), planning (all authors), data collection (ENS and GO'B), test requests (ENS, GO'B, P-AV, RG and NJK), data management (GO'B, P-AV, RG and ENS), data analyses (NJK and ENS), write-up (ENS and NJK), review of manuscript (all authors listed), final preparations for submission (ENS, SG and NJK), initial submission (ENS), responses to reviewers comments (ENS and NJK), review of revised manuscript (all authors) and resubmission (ENS). Guarantor (ENS).
Funding The authors have declared a specific grant "IoPPN, King’s College London" for this research.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.