Article Text

Abstract
Postoperative X-rays are a key part of management of orthopaedic patients. These X-rays serve to check stability of orthopaedic fixation as well as to ensure that there are no peri-implant fractures and periprosthetic fractures following surgical fixation of fractures and arthroplasty procedures, respectively. Timely accurate interpretation of postoperative X-rays are crucial in guiding weight-bearing status as well as rehabilitation. Therefore, delays in X-ray acquisition may impact initiation of postoperative rehabilitation and overall length of stay negatively. The aim of this project is to optimise acquisition of postoperative X-rays in patients undergoing implant surgery and as a result increase efficiency of deployed healthcare staff. A multidisciplinary team was formed to study the efficacy of a new workflow for patients to undergo X-rays immediately after surgery while en-route to the ward. Pretrial and in-trial delays in acquiring X-rays and total man-hours spent on transport were recorded. These processes were refined and integrated to optimise the new workflow. Compared with the old workflow, delays in obtaining X-rays were significantly reduced from the longest of 20 hours and 40 min to no delays at all. Overall man-hours spent on transport of these patients were reduced by a mean of 12 and 16 min for nurses and porters, respectively. The trial workflow has since been adopted successfully by our institution and since inception has become standard practice, allowing timely review of postoperative X-rays. This has led to increased workforce efficiency as well as timely rehabilitation and discharge of patients.
- Postoperative Care
- Quality improvement
- Nurses
- Surgery
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Sengkang General Hospital is one of Singapore’s newest public hospitals. The 1000-bed hospital opened its doors on 18 August 2018 and serves mainly the population living in the North Eastern districts of Singapore. It consists of an administrative and outpatient block connected to six inpatient ward blocks via a central corridor. Within the hospital grounds is also a 3-block Community Hospital designed for slow stream rehabilitation and sub-acute care.
The Operating theatres (OTs) are located on the second and third storeys within the main blocks. These consist of emergency OTs, day surgery OTs and major OTs. The OTs are adjacent to the main elevator lobby leading to the two blocks housing the inpatient surgical wards. The radiology department is housed in the main Outpatient block also adjacent to the main elevator lobby on the second storey.
Postoperative X-rays are routinely performed in our institution after Orthopaedic surgical procedures involving metallic implants. These range from postoperative patients after open reduction and internal fixations to complex poly trauma, external fixation devices, spinal instrumentation, post corrective osteotomies and hip or knee arthroplasties.
Our team found that there were significant delays in acquiring postoperative X-rays for patients following fracture fixation as well as arthroplasty due to various factors. Some of these factors include lack of manpower and radiographers overnight to perform non-urgent x-rays, prioritisation of emergency patients, skeleton nursing staff to porter patient and patient comfort and sleep overnight after surgery. As a result, surgeons were unable to review X-rays during rounds the morning after surgery. This led to delays in physiotherapy and further rehabilitation plans.
The specific aim of this project is to reduce the delay of postoperative x-ray acquisition by 90% and have 0% delays of more than 12 hours from completion of surgery by the end of the trial period of 2 months. The broader aim was to ensure that rehabilitation could begin on the first post day without undue delay.
Background
Postoperative X-rays are often required after fracture fixation and arthroplasty surgery in the practice of orthopaedic surgery.1 Although there have been many studies that show postoperative X-rays do not affect management of patients following fracture fixation,2 especially in cases of hip fractures, a majority of surgeons still commonly request for these X-rays to assess reduction and fixation, evaluate stability of implants and to make informed decisions on postoperative rehabilitation.3
In Singapore, these X-rays are largely performed due to a number of factors such as documentation for medico-legal purposes, management of patient’s expectations and largely cultural nuances of patient care in Singapore. Similar cultural nuances are seen also prevalent in other institutions around the world. Chakravarthy et al4 conducted an audit of the clinical practices in the UK and discovered that there was a lack of national consensus in the UK on the use of postoperative check x-rays with 96% of surgeons still ordering postoperative check x-rays after surgical fixation of hip fractures but 83% ambulating patients before the reviewing the X-ray.
While the general evidence presented suggests against the need for postoperative X-rays,5–7 they are still widely used in Singapore due to cultural practice norms and medico-legal documentation of outcomes of surgery. This is in line with postoperative complications seen in other reports. Ndu et al8 reviewed 632 total hip arthroplasty cases of which 12 cases were identified with technical issues (7 cases of medial screw penetration from the acetabular cup of which one required removal, one case of acetabular component protrusion, three periprosthetic femoral fractures and one dislocated hip which was first identified clinically and subsequently taken back to theatre for revision. Similarly, Hassan et al9 reviewed 624 consecutive total knee arthroplasty cases of which 2 showed significant abnormalities (an undisplaced tibial periprosthetic fracture and an inferior pole patella avulsion fracture).
Nair et al10 examined 1319 patients in his institution who had undergone surgery involving intra-operative fluoroscopy of which 1131 had postoperative X-rays performed within the first week. Twelve patients were identified to have significant complications discovered on postoperative X-rays which required return to theatre.
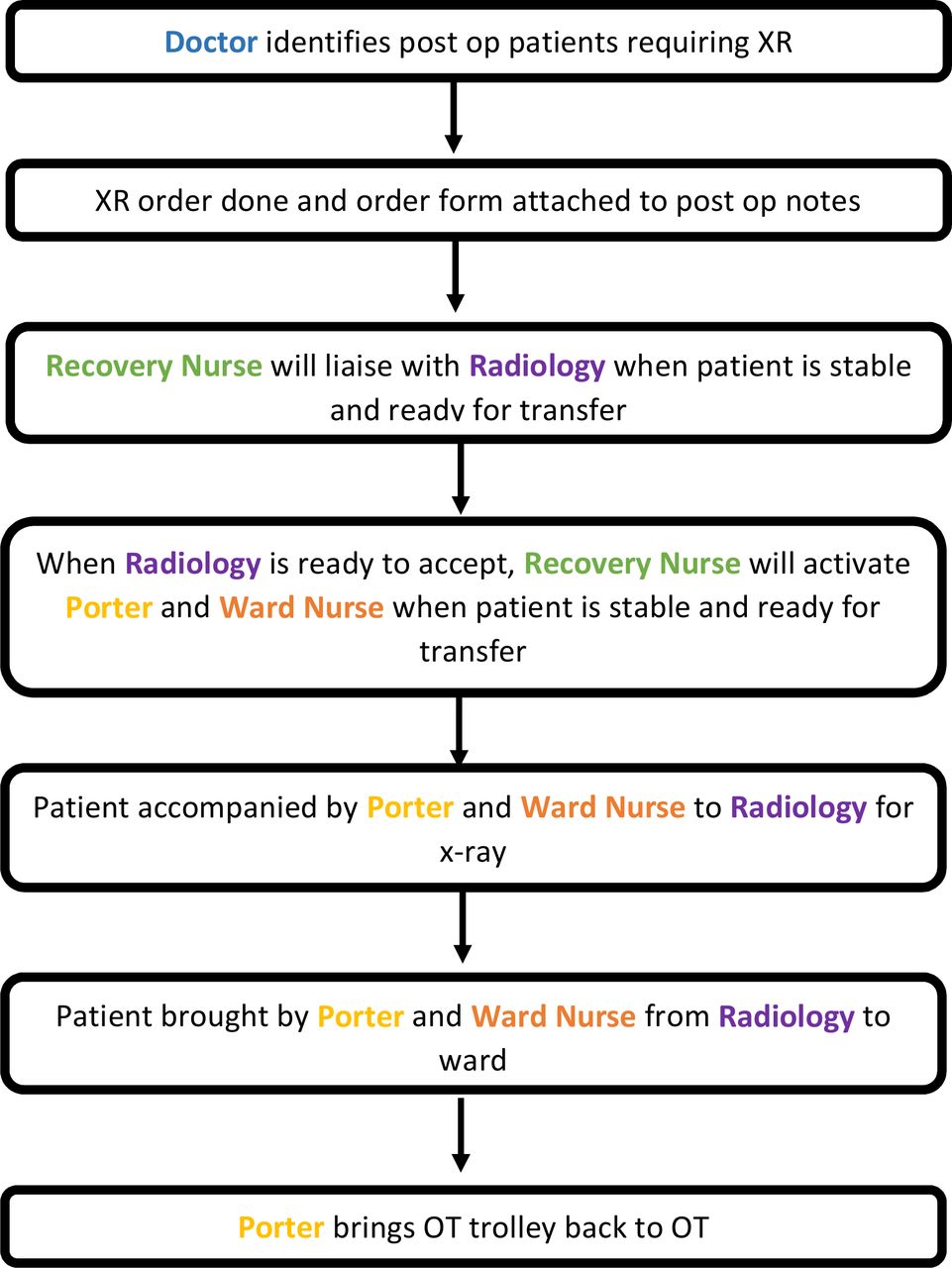
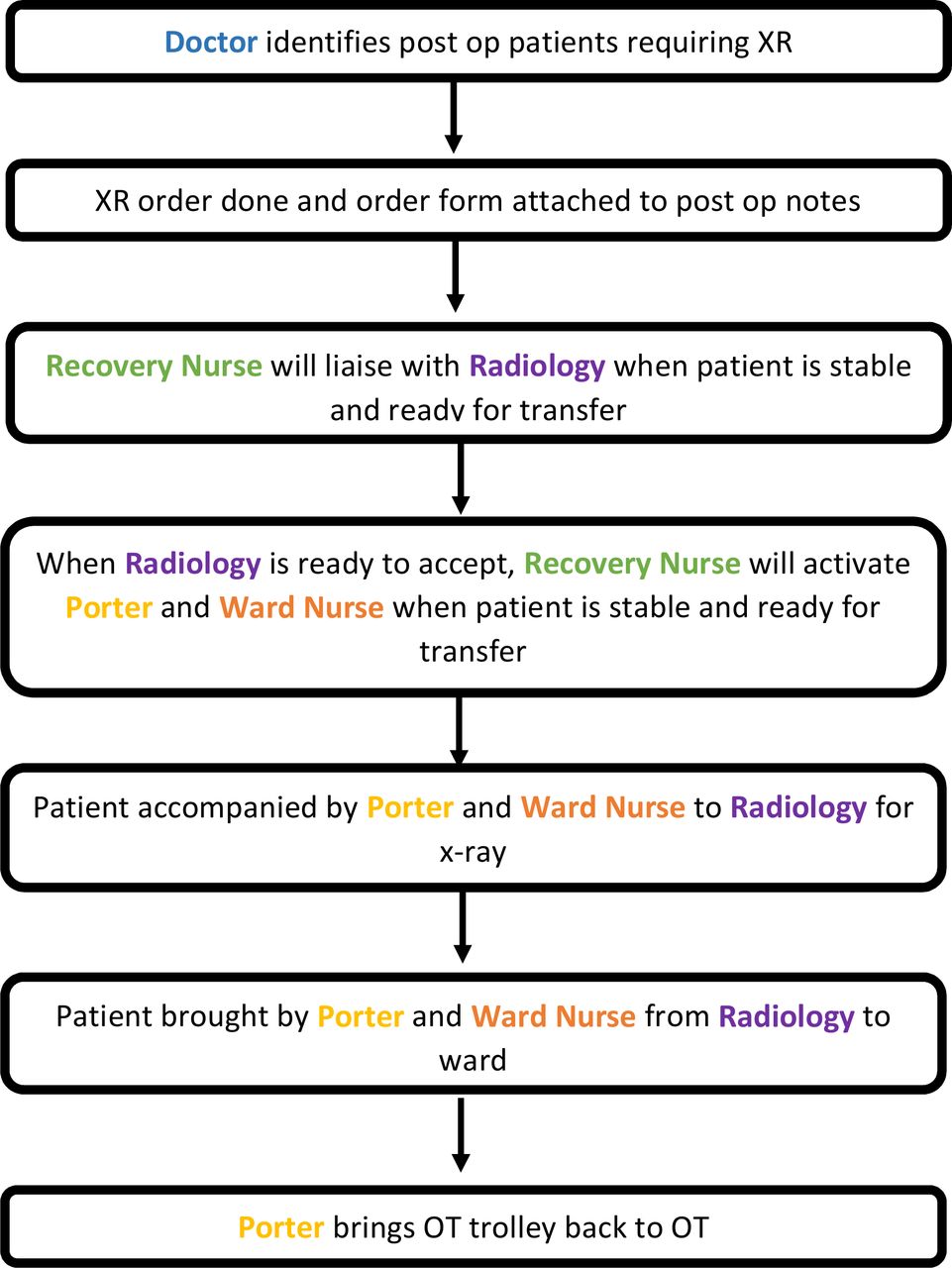
Traditionally, the postoperative patient is monitored in the post anaesthesia care unit (PACU) before transfer from the OT to the place of final disposition. This transfer is carried out by porters and nurses. Patients are reviewed by the team doctors or the duty doctors on the ward before postoperative X-rays are ordered either manually or electronically. Patients are then transported to the radiology department by porters and nurses for these X-rays to be performed (figure 1).

Current Post-operative Workflow.
Delays in the above process leads to inadvertent delays in reviewing of the X-rays, and therefore, rehabilitation of the patient. Delays in initiation of postoperative rehabilitation has been shown to delay recovery and increase patient length of stay.11
A multidisciplinary team was therefore convened to develop, pilot and subsequently implement a new workflow to optimise acquisition of postoperative X-rays in patients undergoing surgical procedures involving implants. With the optimised workflow, we hypothesised that there will be a reduction in the overall number of man-hours of nurses and porters transporting patients and a reduction in delays in acquiring postoperative X-rays.
Principle considerations
Challenges that stakeholders faced in current workflow
Prior to commencement of the project, we interviewed stakeholders to identify challenges faced in the ‘old’ workflow (figure 1). Below is a summary of the key concerns from each stakeholder group.
Doctors—Doctors required postoperative check X-rays to review outcomes of surgery and to decide on the postoperative rehabilitation plan. The primary concern of doctors was that significant delays in obtaining postoperative X-rays meant that decision on weight bearing status of patients were delayed. This in turn delayed physiotherapy for the affected patients and led to unnecessarily prolonged inpatient stay.
Ward nurses—Ward nurses were concerned with the long durations of travel out of the ward on escort duties when accompanying patients for X-ray acquisition. Nurses were required to escort patients back from the OT to the ward and again to radiology for further X-rays. The shortage of ward nursing manpower also meant that the longer durations spent transporting patients reduced the number of remaining nurses available to care for patients in the ward.
OT staff—OT staff coordinate the assignment of porters who assist with transport of patients to and from the OT. With limited numbers of porters and a longer turn-around time for each patient, usage of their resource is scarce. Delays in the transport of one patient may cause subsequent delays in other patients’ transport which can interrupt the OT schedule.
Radiology staff—Being a new institution, our radiology department had a limited number of radiographers to assist with inpatient, outpatient, emergency and intraoperative X-ray orders. Due to lean manpower, inpatient and outpatient X-ray services are only scheduled from 09:00 to 18:00 hour daily. After 18:00, the radiographers based in the Emergency department (ED) will then manage both urgent inpatient and emergency x-ray requests from the radiology suite in the emergency department
Measurement
This quality improvement project was performed with an aim to optimise acquisition of postoperative X-rays in patients undergoing implant surgery and as a result increase efficiency of deployed healthcare staff.
Two data collection forms were created for both phases of the project: pretrial phase and trial phase. The pretrial phase involved collecting data on the ‘old’ workflow to identify areas of delay. The in-trial phase was used to evaluate the ‘new’ proposed workflow and evaluate its success.
All patients undergoing implant procedures were included. Patients requiring transfer to the high-dependency or intensive care units (ICUs) were excluded due to the unstable nature of their condition. Due to the operating hours of inpatient radiology services, patients who had completed surgery after 16:00 hour were also excluded from this project.
Forms were designed to record travel times back from OT to the ward and to and from the radiology department for X-rays. The forms measured total nurse and porter transport duration for both pretrial and in-trial periods. Forms were clipped to each patient’s file folder postoperatively. All departments were briefed to fill forms on seeing them attached to case notes. These forms did not contain any patient identifiers to ensure patient confidentiality.
All individual stakeholders were asked to submit subjective feedback at the end of the trial period This was also collated and analysed by the study team.
Design
The ‘new’ Workflow
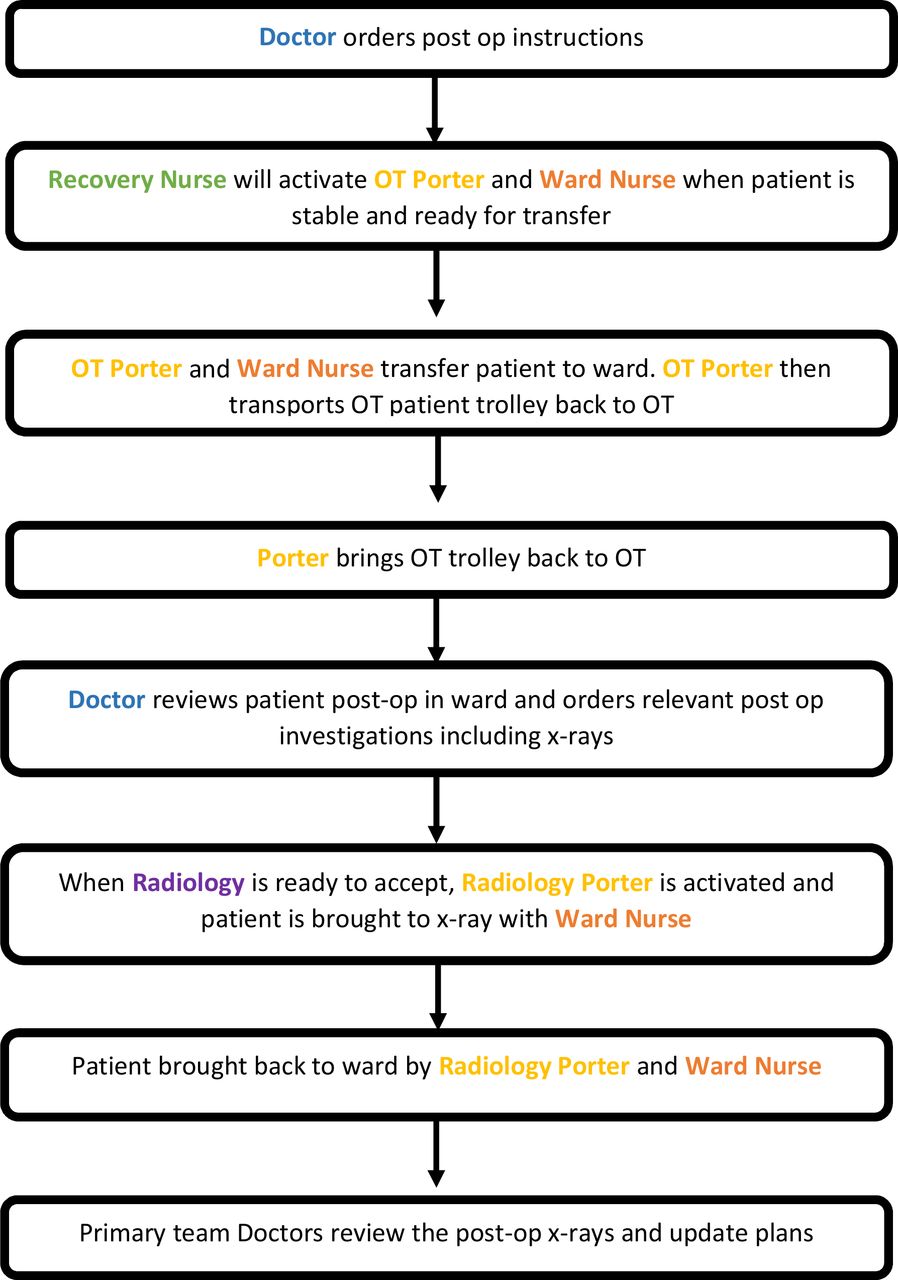
The ‘new’ workflow was designed with the aim to minimise staff movement and to maximise each travel journey. In the new workflow, postoperative X-rays will be ordered by the surgical team immediately after completion of surgery. Once patients are deemed stable in PACU, they will be transported with a nurse and porter to the radiology department where postoperative X-rays will be taken. This will be done en-route to the ward after which they will be assessed by the ward doctors (figure 2).
“New” Proposed Post-operative workflow.
Assumptions and reasons (why we expected the ‘new’ workflow to work)
A similar workflow to the one being designed has been known to be successfully employed in two other hospitals in Singapore with good effect. Patients of the Orthopaedic departments of these hospitals are able to effectively obtain postoperative X-rays early with minimal delay. Members of our department have also had experience working in these other institutions and understood the proposed workflow.
Being a newly established institution, study members assumed that it will be easier to implement changes that will optimise manpower utilisation in the clinical care of patients. Furthermore, in introducing a system that has been previously known to members of the department, it was assumed that the uptake of the new workflow will be faster with minimal disruption to daily clinical practice.
We assumed that the radiology department would be able to effectively prioritise these postoperative X-rays. We also assumed that there will be minimal disruption to patient transport as well as patient waiting time at the radiology department. These concerns were discussed by the study team with contingencies weaved into the ‘new’ workflow.
Consultation and engagement
During the planning phase, the various stakeholders who would be involved in the execution of this workflow were identified. Each stakeholder was called individually to meet with the study team to discuss the proposal and any concerns they may have. Limitations of each stakeholder were assessed and compiled.
Inputs were obtained from surgeons, nurses from the ward team and the OT, radiology department and radiographers and managers of the general services team who assist in deployment of hospital porters.
Project team
The project team was consisted of members from each of the stakeholder groups. Before the implementation of the project, a meeting was called to discuss the concept, plan, limitations and the proposed workflow. Team leads were assigned per stakeholder group. They were tasked with briefing team members on updates and the longitudinal changes to the workflow. They also attended weekly meetings to coordinate and explore various issues and areas for improvement.
Problems anticipated
One of the main areas in the new workflow which seemed be most likely to fail was the phase in which patients were to be transported from the OT recovery to the radiology department for X-rays to be done. This was the major step in the workflow with the greatest number of possible problems anticipated. Availability of radiology services on demand was the biggest anticipated problem as demands for radiology services extend to inpatient and outpatient settings. Furthermore, patients could not be lodged in the PACU for long durations as they would stagnate manpower resources and space. To address this, radiology agreed to prioritise all postoperative X-rays to facilitate patient transfer and disposition.
Another anticipated problem was the time taken for performing X-rays. It is assumed that our patients will be stable postoperatively for a period of time before they are reviewed by the doctors on the ward in the ‘old workflow’. In the ‘new workflow’ there was a risk of patients not being stable enough to wait for a long time before the X-rays are taken. To circumvent this, we placed strict criteria for ordering en route postoperative X-rays. Any patient deemed to have labile parameters by the anaesthetist and/or needing high dependency or ICU treatment in the immediate postoperative setting will not be sent for en-route postoperative X-rays under this ‘new’ workflow.
Sustainability plan
The plan for this project was to be scaled up as a permanent workflow in our institution. The approval of this workflow would involve presenting the results of the project to the medical board of the hospital for further evaluation. On approval from the medical board, the workflow processes will be instituted as a new protocol within the hospital.
Further expansion plans for this project were to be able to include patients who are transferred to PACU following surgery after 16:00 hour and eventually round the clock.
Strategy
Before the start of the project, all stakeholders were briefed on the action plan and were delegated to brief their respective departments. Doctors were informed 1 week prior and on the day of commencement of the pretrial and trial phases to order the X-rays via forms and to ensure that nurses from the OT and wards were briefed at the start of each shift.
Pretrial phase
PDSA cycle 1: Our initial aims were to ensure forms were filled. Doctors were tasked with printing and attaching forms to case files. Nurses and ward doctors were in-charge of ensuring their section of the forms were completed and forms were returned to the designated collection point. Most surgical teams did not comply for the first few days and compliance rate was poor.
PDSA cycle 2: OT nurses were then tasked to ensure all forms were attached to postoperative patients’ case notes. Ward doctors were reminded on a daily basis to ensure forms were filled correctly and to ensure nursing teams also completed the relevant section of the forms. Nurses were encouraged to add a reminder regarding this project at the start of each shift. There was significant improvement in form completion although 60% were still incomplete. Not all forms were received at collection point and some remained clipped to case notes or lost in pneumatic tube delivery systems.
PDSA cycle 3: The ward clerk was engaged to be the person receiving all tubed forms from all wards and collating them into a file folder. Senior nursing managers volunteered to ensure forms were collated at the end of each day. The QI team lead would verify that all forms were received from each postoperative patient and checked through all files at the end of the day. Duration of data collection was extended from 1 to 3 weeks to ensure enough viable data was collected.
Trial phase
PDSA cycle 4: Follow-up from the pretrial phase, all existing protocols were kept. The major change in workflow was for surgeons to place postoperative orders immediately after surgery so that they may be completed as per the workflow. Despite reminders and briefing before commencement, a large proportion of patients did not have order forms completed. Surgeons were not used to ordering the required investigations postoperatively and found it inconvenient.
PDSA cycle 5: Notices were printed and pasted above the computers in all orthopaedic surgery theatres to remind surgeons to print out order forms. OT Nurses were tasked with checking and reminding surgeons both immediately after surgery as well as while verifying clinical documents while patient was in recovery. This ensured that all required orders were placed appropriately before patient was transported. Trial phase was extended to 3 weeks to match the pretrial phase.
Results
Objective data
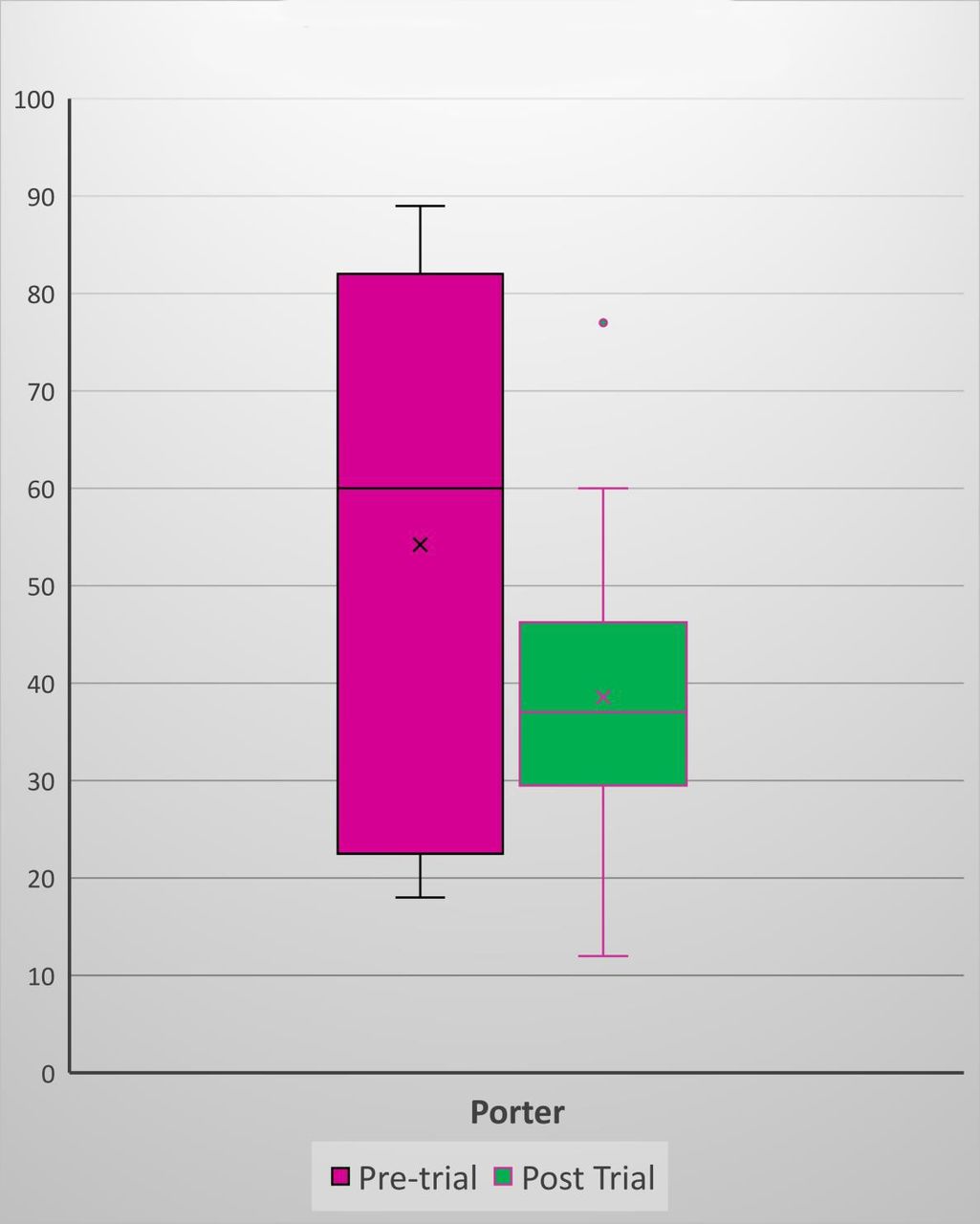
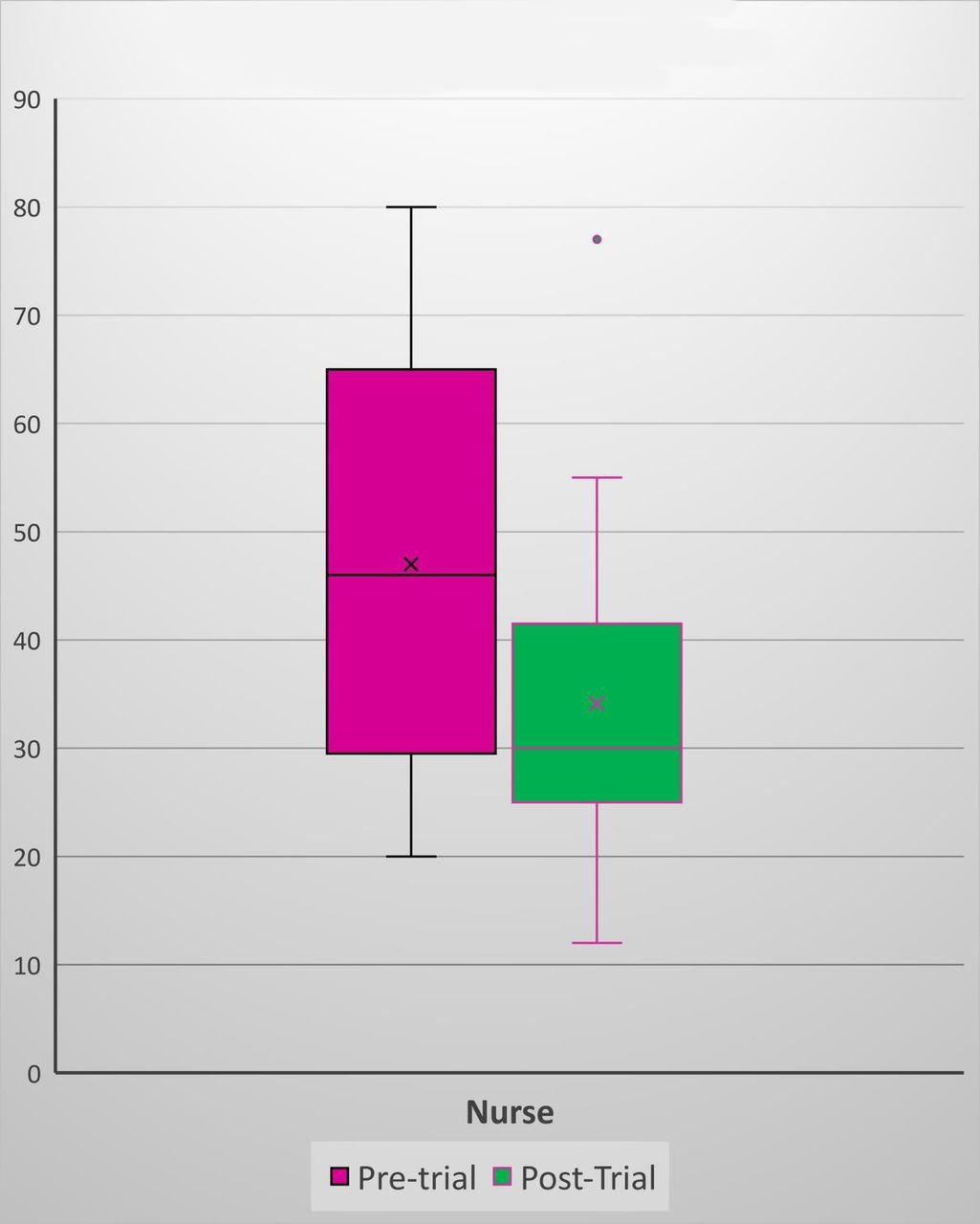
The mean number of man-hours spent by nurses to transport patients was 47 min (20–80 min) in the pretrial period as compared with 34 min (15–77 min) with a mean reduction of 13 min (p<0.05) (figure 3). The mean man-hours spent by porters to transport patients was 54 (18–89) min in the pretrial period compared with 39 (15–77) min with a mean reduction of 16 min (p<0.05) (figure 4).

Total nurse transport time.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Total porter transport time.
In the pretrial period, the longest delay recorded for obtaining postoperative X-rays was 20 hours and 40 min. A further analysis of this case identified a few reasons for this. Delays in postoperative patient review by ward doctors and subsequent late submission of X-ray requests, delays and number of pending cases in radiology department and availability of nurses to escort patient for the X-ray were cited as some of the reasons.
Subjective feedback
Doctors reported increased satisfaction with obtaining most postoperative X-rays on the same day. They were able to review radiographic outcomes of surgery and prescribe the appropriate physiotherapy and weight-bearing exercises for patients. Doctors were also able to explain outcomes of surgery on the same postoperative day to patients.
Ward nursing staff reported significantly less disruption in their ward work with only a single trip required to ferry patients in the new workflow. Furthermore, they reported less time spent out of the ward thereby increasing contact time with their other inpatients. This new workflow was supported by the OT staff who were able to support the extended duration of single porter travel with minimal disruption and delays.
Our radiology colleagues reported significantly increased ease with postoperative X-rays as patients were still under the effects from analgesia from their surgery. This resulted in increased ease of positioning and obtaining X-rays with reduced time taken to obtain them. Radiographers reported a subjective decrease in time taken to perform X-rays.
Lessons and limitations
One of the biggest limitations of the study was the coordination of the various departments and elements. Multiple departments involved required briefing and coordination. The advent of group text messaging services greatly improved communication.
Coordination of key services along the pathway was also essential. Delays by radiology to receive patients postoperatively would mean longer patient waiting time in OT recovery. Factors such as heavier patient load with long queues catering to both inpatient and outpatient services would be a factor. This would lead to further delays in transferring patients out of OT recovery, which would also lead to a strain on OT nursing manpower available to care for postoperative patients. To negate this, OT nurses were to inform the radiology suite 30 min before patient is stable enough to be transferred. This would allow time for the radiology suite to ensure an open slot is available to receive the postoperative patient and to allow for arrival of ward nurses and porters to take over care and patient transport.
Delays in postoperative review by ward doctors also was a limitation to both the study and overall patient care. These delays were largely attributed to the requirement of doctors to attend to more sick patients at the time. The original workflow required doctors to review patients postoperatively first before ordering postoperative check X-rays. This was identified as one of the main limitations of the original workflow.
Apart from the administrative challenges, the new protocol heavily relied on the assumption that postoperative patients that are not going the high-dependency unit or ICUs were going to be stable for the entire postoperative duration from leaving OT recovery to obtaining postoperative X-ray and subsequently returning to the ward. The multidisciplinary team debated this and after assessment deemed the total duration for postoperative X-rays to be within safe limits for patient transfer.
Another limitation was quality of completed forms. While the project lasted for 3 weeks at each phase, a lot of the collected forms were not completed adequately. More than 60% of completed forms were unusable for data collection as a result.
Postoperative X-rays are an integral part of a holistic assessment for Orthopaedic patients following surgery. The speed and ease at which these can be obtained affects their rehabilitation and overall length of stay in hospital.
Infrastructural factors that supported this newly implemented workflow include location of OT, inpatient radiology suites and wards. In our institution, the convenience of having the radiology suites en-route to the orthopaedic wards make it ideal for this workflow to be implemented. Other hospitals in Singapore have similar workflows as well and in one instance, the hospital has satellite radiology stations situated within the ward blocks to cater to early requests and a similar workflow. These satellite stations are also used for other urgent radiology requests such as chest and abdominal X-rays.
The subjective feedback we had received after implementing the new workflow reinforces its efficacy and its effect on optimising resources and time. It has greatly changed normal departmental processes to better accommodate needs of our patients. Although we understand that similar workflows may not be easily adoptable in most institutions, it can act as a template to assist other institutions when considering expansion or building of new infrastructure.
Conclusion
Our new workflow of acquiring postoperative X-rays for patients following orthopaedic surgery procedures has shown to be easily administered with tangible benefits of earlier assessment and rehabilitation for patients as well as better utilisation of resources with good end-user experience. It was presented to the hospital’s medical board for evaluation post trial and was found to be satisfactory. It has since been adopted to good effect and is now the standard workflow for all postoperative orthopaedic patients.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
In accordance with policy guidelines in Sengkang General Hospital, the study presented is intended to improve the care of patients and expedite recovery. It focused on delays in obtaining x-rays only and did not alter clinical practice. Patients were informed prior to surgery of the requirement for post-operative x-rays. Patients were also appropriately triaged as part of the study to avoid placing patients at high risk. The processes of this study were also scrutinised by the Medical Board of Sengkang General Hospital to ensure safety to patients during the study and subsequently in its subsequent implementation.
Acknowledgments
Medical Board, Sengkang General Hospital, Department of Radiology, Sengkang General Hospital, Operating Theatre Management Unit, Sengkang General Hospital, Operating Theatre Nurses, Sengkang General Hospital, General Services, Sengkang General Hospital, Hospital Porter Team, Sengkang General Hospital.
Footnotes
Twitter @supertrouper01
Correction notice This article has been corrected since it first published. Author name 'Hamid Rahmatullah Bin Abd Razak' has been updated.
Contributors The project idea was conceived by SSS and HRbAR with support and approval from MKW. The project was planned and executed by SSS in association with LCAT. Execution was also supported by MTbMS, HRbAR and MKW. Data collection and analysis was performed by SSS and LZDK. SSS and HRbAR wrote the manuscript and the overall project was supervised by MKW. SSS will act as the guarantor for this project.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.