Article Text

Abstract
Background Unmet social needs in early childhood create risk of lifelong physical/mental health challenges. Pediatricians can intervene by routinely assessing child development including child and family social emotional wellbeing. Many providers report barriers to interventions that meet families’ social needs and lack reimbursement.
Objectives Test a national strategy to increase social needs assessment, family-centered discussion, referral/linkage, and follow-up with families at 90% of 0–5 years well child checks (WCC).
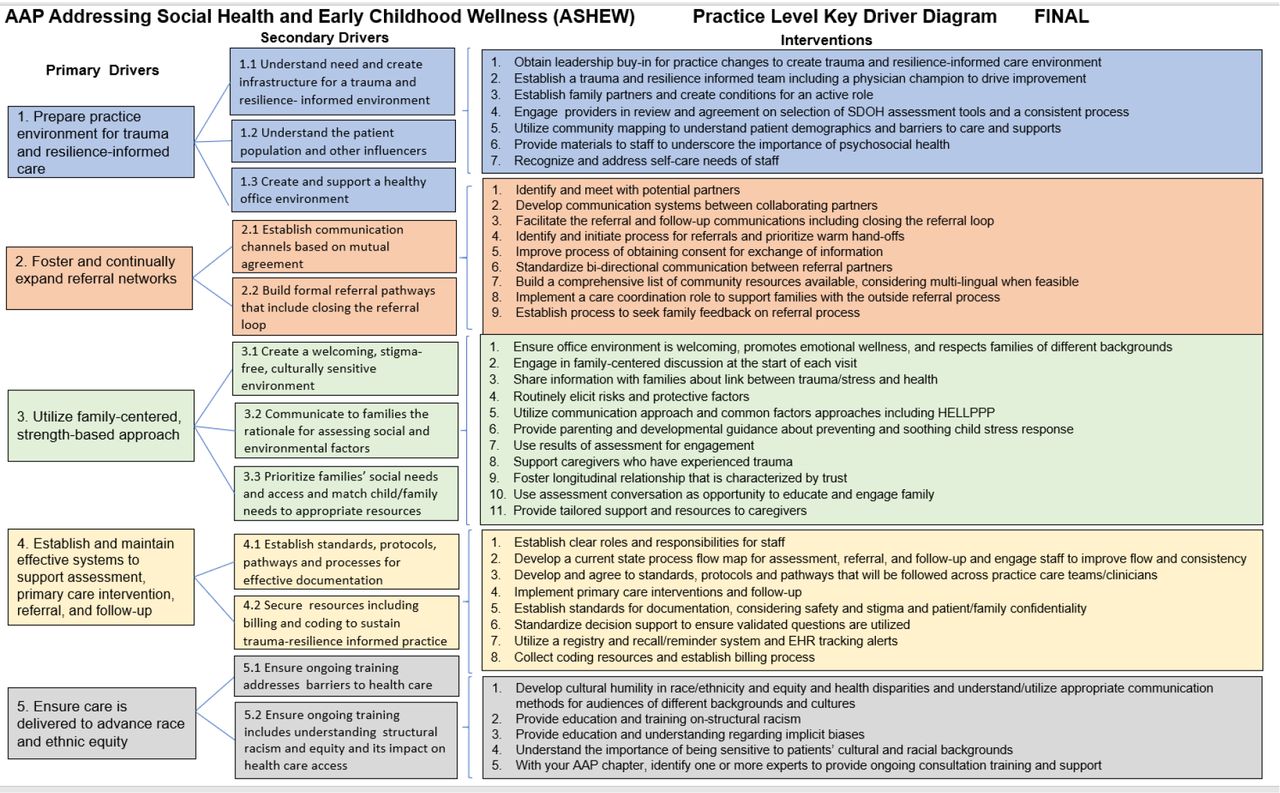
Methods The American Academy of Pediatrics (AAP) conducted an 11-month quality improvement (QI) virtual learning collaborative using the Model for Improvement to address social needs (figure 1). Seven AAP chapters, supported by AAP, provided 66 primary care practices monthly education/collaboration, data review, and coaching. Practice teams included a physician leader, staff, administrative support, and family advisor. Practices conducted monthly chart reviews (N=40) following 6-month WCC for perinatal depression (PD), and following 6, 15, 24, and 48-month WCC for social drivers of health (SDOH) and social emotional development (SED). Chart reviews assessed (yes/no) documentation of screening, discussion, and referral/linkage. Improvements from baseline were examined using run charts. Practice transformation strategies included family engagement during WCCs, embedded family advisors on practice QI teams, strengthened community partnership, and enhanced support from AAP chapter family advisors. Quarterly qualitative surveys further assessed practice transformation on trauma and resilience informed care, family-centered approaches, and care to advance race and ethnic equity.
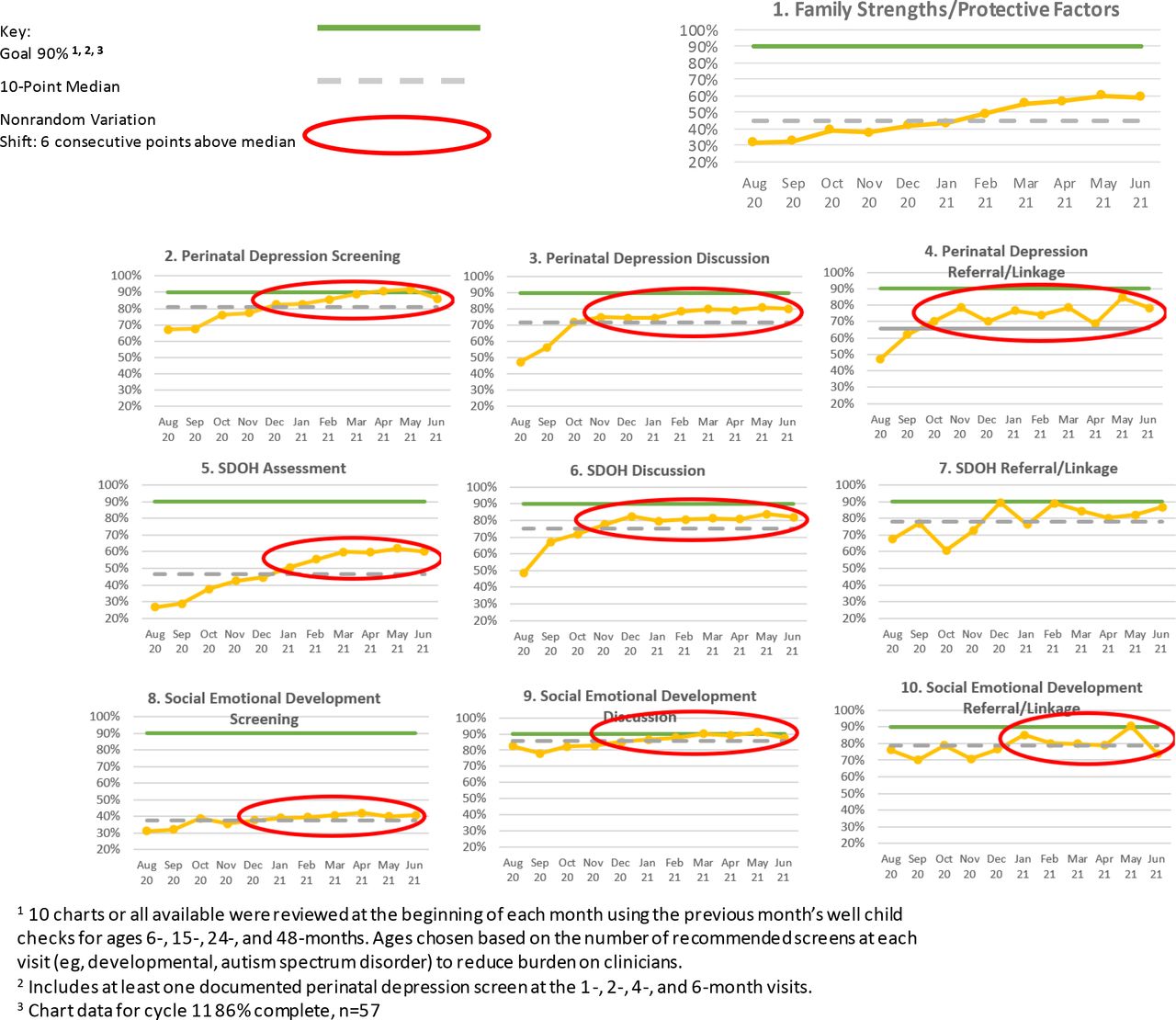
Results Chart review data shows nonrandom variation in 8 of 10 measures or a shift of 6 consecutive points above the median (figure 2).
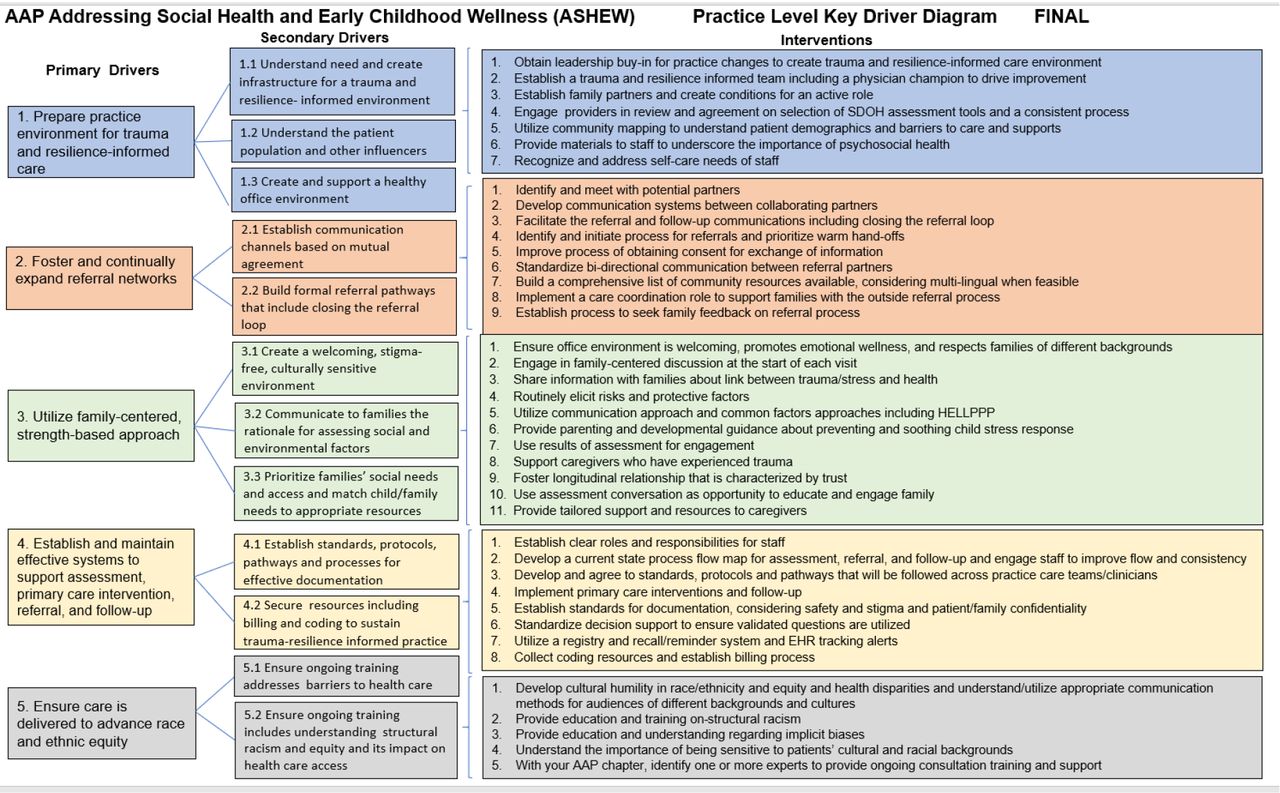
AAP Addressing Social Health and Early Childhood Wellness (ASHEW) key driver diagram
{kind=link}
{kind=link}
ASHEW run charts. 110 charts or all available were reviewed at the beginning of each month using the previous month’s well child checks for ages 6-, 15-, 24-, and 48-months. Ages chosen based on the number of recommended screens at each visit (e.g., developmental, autism spectrum disorder) to reduce burden on clinicians. 2Includes at least one documented perinatal depression screen at the 1-, 2-, 4-, and 6-month visits. 3Chart data for cycle 11 86% complete, n=57; 2Includes at least one documented perinatal depression screen at the 1-, 2-, 4-, and 6-month visits; 3Chart data for cycle 11 86% complete, n=57
Conclusions Pediatric providers can make quality improvements to address unmet social needs using early relational health to foster family resilience. Next steps include continued progress toward goals during a second phase and enhanced training resources shared with all pediatric providers to increase rates of screening, discussion, referral/linkage, and ascertaining outcomes from families.