Article Text

Abstract
The Welsh Transplantation and Immunogenetics Laboratory (WTAIL) is responsible for managing patient work-up for haematopoietic stem cell transplantation (HSCT), the only potentially curative option for many haematological and non-haematological conditions. Work-up requires regular communication between WTAIL and the transplanting clinicians, facilitated by weekly multidisciplinary team (MDT) meetings, to agree decisions and proceed through each work-up stage. Effective communication and minimising error are critical, as transplanting cells from a suboptimal donor could have severe or fatal consequences for the patient. We reviewed our HSCT patient management and identified issues including staff dissatisfaction with the inefficiency of the current (paper-based) system and concern about the potential for incidents caused by errors in manual transcription of patient information and tracking clinical decisions. Another driver for change was the COVID-19 pandemic, which prevented the usual face-to-face MDT meetings in which staff would show clinicians the paper records and reports; the shift to online MDT required new ways of sharing data. In this project we developed a new central reference point for our patient management data along with electronic patient summary sheets, designed with an eye to improving safety and efficiency. Over several improvement cycles we tested and refined the summary sheets with staff and clinicians and experimented with videoconferencing to facilitate data sharing. We conducted interviews with staff from which we concluded that the new process successfully reduced transcription and duplication and improved communication with the clinicians during the pandemic. Despite an increase in workload due to build-up of active patient work-up cases during the pandemic, staff reported that the new summaries enabled them to cope well. A key initiative was creation of a ‘Task and Finish’ group that helped establish continual improvement culture and identified additional areas for improvement which have been followed up in further improvement projects.
- efficiency
- organisational
- laboratory medicine
- PDSA
- quality improvement
- transplantation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The work-up process requires regular communication between our team (two to three Welsh Transplantation and Immunogenetics Laboratory (WTAIL) healthcare scientists led by a section manager) and a team of three transplant clinicians whom we assist in clinical decision making. This process is facilitated by weekly multidisciplinary team (MDT) meetings, attended by at least two clinicians and three WTAIL staff, to make decisions, identify and reserve potential donors and agree a timeline to transplant.
Each ‘active’ haematopoietic stem cell transplantation (HSCT) patient case heavily impacts the workload of the department as HSCT patients require continual review of their clinical status, compatibility tests and timely management of donor suitability/availability for transplant. In WTAIL we managed HSCT patient records predominantly using paper files, supported by a basic in-house IT programme ‘Transplant Utilities’ (TXU) to record data and generate reports. Several workarounds (eg, forms and spreadsheets) had been introduced to record additional data not captured in TXU and cope with the increasing demands and complexity of the work.
To identify issues with the current processes, I (FM) conducted semi-structured interviews with WTAIL staff and the transplant clinicians (questionnaire 1; the questionnaires used in this project are available here (online supplemental file 1—Questionnaires)). Staff felt the current system made it difficult to ‘stay on top’ of patient management and to handover work between staff, particularly when the number of active cases was high, and had inherent risk of causing clinical incidents.
Supplemental material
Patient and donor information was recorded and tracked using several paper forms and spreadsheets, each fulfilling a different purpose (eg, action log, sample tracker, etc). These required staff to transcribe the same information to several different places.
During interviews (online supplemental file 1, Questionnaire 1) the clinicians expressed a clear preference for continuing to request specific information from our healthcare scientists during the weekly MDT meetings, despite having copies of written reports. This required our staff to transport all active patients’ paper files (comprising all paper records retained in WTAIL relating to their compatibility testing and donor searches) to the MDT meeting, locate a patient’s file within this set, find the relevant information and read it out at the meeting. Patient files were occasionally difficult to locate at short notice, given that they can be used in different areas of the laboratory throughout work-up. The meetings were often interrupted so that staff could spend time locating files or finding the specific requested information within them, then reading out the required information. Key clinical decisions and rationale were documented in meeting minutes rather than in individual patient records, which made them difficult to track.
To ensure no important updates were missed, a workaround practice had been developed: all active patient cases were discussed at each week’s MDT meeting, even if there was no progress or actions required, often repeating the same information.
Our staff were also concerned that there was no data-verification process for the manual transcriptions being accurate and up to date. While there had been no recorded incidents relating to HSCT patient management in the previous year, staff felt there was material risk from reliance on these transcriptions, and also risk from misinterpretation by clinicians of information read out to them. These have the potential to impact on patient and donor safety.
Interviews with WTAIL staff (online supplemental file 1, Questionnaire 1) revealed a high level of dissatisfaction with the current process for HSCT patient data management and communication, and strong motivation to introduce improvements, particularly given the MDT meetings’ transition to a remote format during the pandemic. It was apparent that some written reports served limited purposes and may increase risk, despite generating a significant administrative workload for WTAIL. However, we found that the clinicians expressed concerns about any radical change in the way of working and departure from their preferred format.
The aim of this service improvement was to improve the safety and efficiency of the HSCT patient work-up process over a 3 to 4-month period, improve staff morale and strengthen partnerships with the clinical team.
Background
The COVID-19 pandemic has led to significant changes in how NHS are organised and delivered, with organisations under intense pressure to adapt.1 At WTAIL, the pandemic presented us with new challenges such as altered ways of working (remote MDT meetings) and increased workload, creating strong drivers for service improvement.
Initially, the local response to the pandemic was to postpone many transplants. Transplants then gradually resumed, based on clinical urgency and hospital capacity. At WTAIL we continued work-up activity, with each patient’s progress ‘paused’ at various stages of the process depending on their clinical status. We anticipated increased workload as patients continued to be activated, and so adding to the management list, but fewer were being transplanted and closed out. MDT meetings had to be conducted remotely instead of face-to-face, preventing the usual practice of presenting clinicians with paper documents to communicate complex results and data during meetings.
The initial interviews (online supplemental file 1, Questionnaire 1) revealed a high level of staff motivation in WTAIL to improve practices but initial reluctance from the clinicians to change their preferred ways of working. Other anticipated obstacles included staff time required to transfer existing patient data to a new system, the potential for staff to forget to update such a system or enter data incorrectly and there being no systems in place for verifying data to ensure accuracy. The pandemic introduced further obstacles by exacerbating communication problems with the requirement for remote MDT meetings.
Measurement
To understand the existing process, we (the authors) developed a detailed process map and identified delays and waste (non-value adding steps) (see figure 1, left side). We revised the maps after each change to assess the potential to remove further waste.
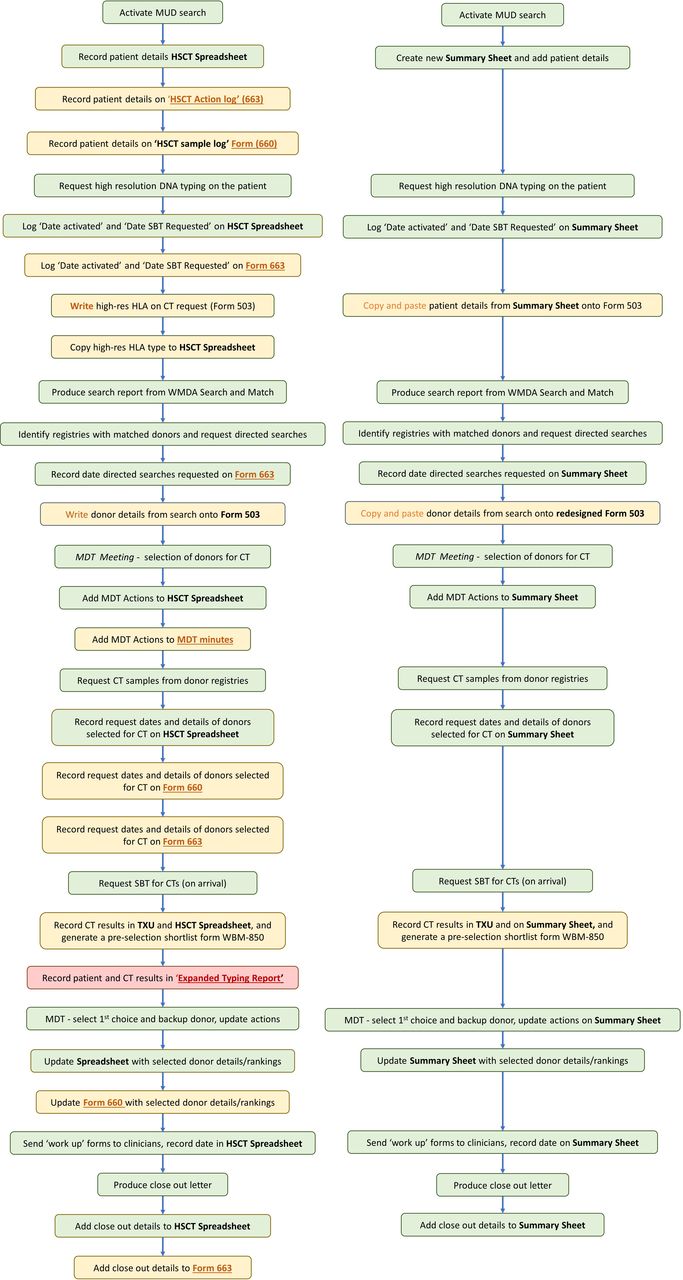
Process maps for HSCT patient work-up before project implementation (left) and after (right). Value adding steps are shown in green. Steps involving duplication (recording of patient/donor details on multiple forms) are shown in orange. These steps were deemed ‘necessary waste’ prior to the introduction of the new summaries because different staff used/recorded the information in different locations (ie, the forms could not simply be removed without a replacement system in place). Non-value adding steps are shown in red. We classified the ‘Expanded Typing Report’ as non-value adding when we established that the clinicians did not refer to the report, even though the information contained within it was reported to the clinicians at the MDT meeting and in the final ‘close out’ letter. This figure emphasises the removal of waste steps and forms. Some necessary waste remains with the required procedures for potential donors (Form 503 and the TXU software component), though we have made the population of 503 much easier. With new LIMS software we hope to remove these remaining waste steps through automation. HLA, human leukocyte antigen; HSCT, haematopoietic stem cell transplantation; LIMS, Laboratory Information Management System; MDT, multidisciplinary team; MUD, matched unrelated donor; SBT, sequence-based typing; TXU, Transplant Utilities; WMDA, World Marrow Donor Association.
I (FM) conducted interviews (online supplemental file 1, Questionnaire 1) with three WTAIL healthcare scientists involved in HSCT patient work-up, the WTAIL section manager and three transplant clinicians. The interviews were recorded and transcribed. I extracted themes, which I then categorised and shared using a 4N Chart2 (figure 2). They also informed value analysis of each step on the process map (figure 1).

4N Chart from Welsh Transplantation and Immunogenetics Laboratory staff interviews.
To study whether staff considered that a change was an improvement, whether any unexpected outcomes or new obstacles had been revealed and to identify the next steps to be taken, after each change I either requested verbal feedback during meetings, completion of written feedback forms (online supplemental file 1, Questionnaire 2) or repeated semi-structured interviews (online supplemental file 1, Questionnaires 3 and 4). This also allowed us to monitor impact on the risk of data communication errors and on staff morale.
To establish the uptake of the new system, we monitored the number of patient cases managed using the new summary sheets versus the old system. As a ‘balancing metric’ we also monitored the number of active HSCT patient cases. A total of 131 patient workups were in progress in WTAIL between January 2019 and March 2020, with an average of 26 ‘active’ workups at any one time (range 15–32 active cases).
Design
We generated initial ideas for improvement from the ‘Nice Ifs’ established during compilation of the 4N Chart based on interview data. Staff expressed the desire to record information in one central place: to have one information system containing all data needed and to ensure that only verified, written results were used to communicate clinical data during MDT meetings.
To help us think about designs, we contacted two Histocompatibility and Immunogenetics laboratories. Both had developed processes for compiling patient summary forms from a central source, to display relevant information for clinicians and track actions. Our initial template design was based on an Excel form provided by one of these other laboratories.
To identify essential data to record in the summary, we reviewed the existing WTAIL paper forms and spreadsheets in consultation with staff and clinicians. Essential data fields included tracking progress (sample receipt, test completion, results interpretation) and logging actions. We were able to exclude data being recorded or transcribed but which was not required or not helpful (eg, uninterpreted test results).
The final version of the summary forms is available here (online supplemental file 2—Summary Forms).
Supplemental material
Strategy
Applying the Model for Improvement (MfI),3 we used Plan-Do-Study-Act (PDSA) cycles4 to test and refine the summary sheet. Initial cycles tested the suitability of the summaries for WTAIL and clinicians’ use. Later cycles experimented with better use of videoconferencing to facilitate data sharing. New information management system designs were guided by 6S thinking (the standard 5S from continual improvement4 plus the 6th ‘S’: Safety5 (figure 3).

{kind=link}
{kind=link}
{kind=link}
Application of 6S (anticlockwise from top image). (A) The 6S tool was applied as a first step to help formulate the project plan and design a summary sheet template. Existing paper forms and spreadsheets were reviewed in consultation with WTAIL staff and clinicians to identify essential data to record in the summary and data currently recorded on existing forms that was not helpful/required. (B) Prior to the QI project, patient files were kept on desks to prompt action from WTAIL staff, moved between different departments depending on actions being taken, or on a trolley for transport from the laboratory to the weekly MDT meetings. Staff often struggled to locate files and often had to search several areas to find them. (C) Following introduction of the summary sheets, files no longer needed to be transported to the MDT meeting and so we could organise them into a filing cabinet in alphabetical order. (D) Files no longer needed to be kept out on desks, or transferred between departments, to prompt actions; this was now achieved using the summary sheets. HSCT, haematopoietic stem cell transplantation; MDT, multidisciplinary team; QI, quality improvement; WTAIL, Welsh Transplantation and Immunogenetics Laboratory.
PDSA cycle 1
To test whether the summary sheets were suitable for display and use at MDT, and whether the clinicians would accept them, we added data for three active HSCT patients to the summary template. The three completed summaries were displayed via video conferencing software in an MDT meeting. We observed the outcome and asked the clinicians for verbal feedback.
We found that the clinicians engaged with the summary sheets and read the displayed information. Their feedback was positive, and they asked for immediate transition to the new system. One minor change was requested. However, some of the WTAIL staff raised concerns about the time and staffing resource required to transfer all existing active patients to the new system and how we would ensure critical data was verified and protected. We also noticed that the clinicians needed to stand directly in front of their display screen to see the information on the summary sheets.
We decided to continue with feasibility testing, incorporating the change, adding protection to agreed fields to prevent accidental change and implementing a process for verification of each change/addition of data to the summaries (addition of an ‘update log’ to the summaries to record the date and details of each change and sign off by a second staff member to verify that the data added has been checked against the original source).
PDSA cycle 2
We next tested the transition process, in particular how closely staff would follow the process for transferring data to the summary sheets. We updated the process map to help them visualise the overview and provided three WTAIL staff with active patient files and asked them to transfer the required information to a summary template over the course of 4 days. Following completion of their summaries, each staff member was asked to return a written feedback form (online supplemental file 1, Questionnaire 2).
All three of these staff members returned questionnaires and responded favourably to using the summary template, finding it relatively simple to complete. They appreciated having all the information in one place and felt it would help reduce duplication, transcription errors and enable the MDT meetings to run more smoothly. However, they expressed uncertainty about the logistics of a real-life situation where data is added gradually by different individuals and concern over how the verification process would work in practice (eg, at which stages would the verification happen, how would staff know which data needed to be verified and when, etc). One staff member found it unclear where some information should go and requested help.
We decided to make the summary template clearer and provide more formal support. By this stage only six of the active patient cases had been transferred to the new summaries (=20% at that time).
PDSA cycle 3
To gather and respond to issues with the transition to the new process, help staff gain confidence in using the summaries and promptly address issues arising, we initiated ‘Task and Finish’ (T&F) group meetings. These involved all WTAIL staff directly involved in HSCT patient management (FM, JP, ED and SD) and had a remit to cover transition issues, spreadsheet protection and verification processes, general logistics and project implementation progress. I (FM) chaired the meetings and the team actively participated, contributed to key decisions and suggested improvements.
Although the meetings were lengthy (~2 hours) and were a heavy workload to organise, this was offset by the benefits of involving the whole team in decision-making and ensuring changes were fit for purpose. The outcome was that the transition to the new process was seen as a priority and so the project gained momentum. Less than 1 month after the first T&F meeting, the proportion of active patient cases transferred to summary sheets reached 94% (n=32 at the time). We noted that introduction of the new summaries had created a ‘hybrid’ system with some patients still managed using the old system, which caused confusion for some staff. The T&F meetings also proved a useful forum to identify additional improvement ideas beyond the project scope and so noted for future work.
In the Act phase we decided to push to 100% of active patients on the new system and to continue with T&F meetings. The verification system was improved on by the T&F group. We agreed the appropriate stages in the process for verification to be performed at and updated the process map accordingly. A system was implemented for colour coding unverified information and moving patient files to a separate folder while awaiting verification, to flag verification required and prevent unverified data being shared in the MDT meetings.
PDSA cycle 4
To test our ability to operate meetings without referring back to patient files, and to identify any additional information required by clinicians but missing from the summaries, we trialled the summary sheets in an MDT meeting. To overcome the obstacle identified in the first cycle where the clinicians had difficulty viewing the forms using video conferencing, we also tested a switch to Microsoft Teams.
We found we did still need to retrieve patient files for two cases to find information not recorded in the summaries, and the clinicians requested that such additional information should be included.
The T&F group facilitated swift refinement of the template for us to re-test.
PDSA cycle 5
To test the refined sheets, we trialled them in the next six MDT meetings. After the sixth meeting, semi-structured interviews were conducted with three WTAIL staff (online supplemental file 1, Questionnaire 3) and two clinicians (online supplemental file 1, Questionnaire 4) to gather observations on the impact of the changes.
The WTAIL interviewees observed an improvement in efficiency in the MDT meetings (as they were now able to proceed without referring to the patient files) and felt that the summaries gave them more control. The clinicians agreed that WTAIL could chair the meetings going forward.
WTAIL staff found updating the summaries during the meetings (so in real-time) was challenging but worthwhile since it replaced the requirement to write up and circulate minutes after the meeting and enabled us to track decisions/actions within each patient record.
We now considered the new process and summary formats fit for purpose.
Results
We were successful in transitioning to reliance on the new summary sheets, which made the meetings more efficient:
‘I’ve definitely seen an improvement in the meetings. They’re much less stressful and I have more confidence in what we’re saying. Plus, it looks much more professional when we’re viewing it on the screen’. (Clinical Scientist A 2020, personal communication, 19 August)
‘We used to be scrabbling around, trying to find the information people want, having to search for it in the file and sometimes it just wasn’t there. Whereas now the information is all in one place, on the screen in front of them’ (Clinical Scientist B 2020, personal communication, 19 August)
‘It was challenging when we had to sit with our noses up against the screen but it’s much better in this setting where we can see it in front of us. With the summaries you get the information to us up front, which is much better than before. We just have to get used to looking at it’. (Consultant Haematologist B 2020, personal communication, 20 August)
Post-transition, the T&F group reviewed the new HSCT patient data management process. We had been able to remove ten waste steps and discontinue two forms and a spreadsheet (see figure 1 left vs right sides). For two of the three remaining necessary waste steps, I had been able to redesign the Form 503 significantly so that staff can directly copy and paste information from the summary sheet and TXU to here and vice versa (previously this was a paper form and everything was hand written/transcribed). This reduced the waste time and was very well received by staff.
However, we realised that colleagues outside the immediate staff team (eg, laboratory staff responsible for sample processing) also used the old paper forms but did not have access to the new summaries or receive any training about them. Effective communication of the changes had been impacted by social distancing measures introduced during the COVID-19 pandemic. We set follow-up actions, including arranging for all other staff involved to have IT access to the summaries and virtual training sessions.
Since we no longer require patient files in the MDT meetings, we have also reorganised the filing system (figure 3).
Reducing the number of steps and forms and amount of physical file handling reduced our workload in WTAIL significantly and freed up time to focus on more value-adding activities. In July 2020, the number of active patient cases reached the highest ever seen in the department (n=36). Despite this, staff reported in the final interviews that they were coping well and credited the new process and summary reports as a major contribution to this.
As shown in figure 1 (right side), the new process still retains three ‘necessary waste’ steps (the duplication involved in populating the required Form 503 and the TXU part of our current IT system which we cannot easily access in MDT meetings and does not have capacity for us to add all the details we need).
Lessons and limitations
Staff feedback was that this quality improvement (QI) project was well organised and ran smoothly. We believe use of the MfI helped us bring this structure and organisation to the QI process and the creation of a T&F group was central to engaging the whole team in the problem-solving process:
‘We’ve just come together as a nice team and the task and finish group are a huge part of that. I felt involved because we’ve had regular meetings to take time out from our routine work and think things through’. (Clinical Scientist B 2020, personal communication, 19 August).
‘I think we’ve moved it along smoothly and very quickly. Each time we’ve come across a problem we’ve talked about it, come up with a solution and implemented it’ (Clinical Scientist A 2020, personal communication, 19 August).
Such involvement is important in developing a QI culture.6
The interviews enabled me to engage with staff one-to-one, gave them a voice and directly involved them in the change process. The initial interviews (online supplemental file 1, Questionnaire 1) helped populate the 4Ns chart (figure 2) and identify ideas for improvement that were important to the team. Subsequent interviews (online supplemental file 1, Questionnaire 3) helped re-engage the staff in the change process, identify how the change was impacting them and generated further improvement ideas.
Contrary to our expectation that clinician approval would be the main obstacle, instead this turned out to be establishing and embedding the new work process with our fellow WTAIL staff: learning new procedures and changing habits/routines. Other QI work has also reported that it can be hard for staff to incorporate new practices into routine work and that it takes sustained effort and encouragement to embed new practices and habits.7 8 The T&F group helped navigate the obstacles and sustain the new process after the PDSA cycles.
Once the team became committed to applying problem solving in the department, we started generating many new change ideas (eg, adopting paper-free communication with other departments, creating electronic patient records, discontinuing written reports, etc). The T&F group was useful for capturing these, and prioritising and facilitating further QI projects (with MfI and PDSA cycles). Subsequently, these projects introduced and refined these new change ideas, with great success, demonstrating we had developed a culture of sustained improvement in the department.
The QI literature emphasises that establishing outcome metrics is important for studying and demonstrating the impact of changes.9 10 In this project, defining quantitative outcome and process measures was challenging. Our workflow is made up of a relatively small number of very complex patient case, with a long cycle time influenced by many external factors (eg, the pandemic, evolving patient clinical status) and with a very small error rate. We could have tried timing staff completing particular tasks. However, the new summary templates impacted on multiple aspects of a highly complex process and staff reflected that while some tasks were now much quicker (such as finding information), some took them longer but were necessary (such as verification). We focused therefore on qualitative data: noting issues occurring in the MDT meetings and repeated semi-structured interviews. These proved adequate to steer the project and to engage everyone involved.
Prior to this project, the weekly MDT meetings tended to run for 2.5–3 hours. Under current practice (the final process we developed) they now tend to run for 1.5–2 hours. We no longer need to consider every patient ‘on the books’ and the summary forms focus discussion. In retrospect, meeting duration might have been a useful quantitative outcome metric. The duration of individual meetings can vary a lot (depending on how many clinicians attend, how complex the patients are that week and whether there is a teaching/training element); but we could have kept records of start and end times, and deducted teaching/training to estimate the time required from this group of busy staff to complete the core business. A series of timings before and after our changes might have provided some evidence of change distinguishable from the variation expected. Another possibility might have been to attempt to measure meeting-time per patient on the books and/or per patient discussed.
Conclusion
We achieved the dual successes of specific improvements to the target process (HSCT patient data management process and the associated MDT meetings) and development of a continuous improvement culture in our department.
The new process improved efficiency, communication and reduced patient safety risks in both MDT meetings (swift access to verified information and reduced verbal reporting) and the enfolding administrative processes (fewer forms, better electronic and physical file management). These raised staff morale and contributed to handling high workload during the difficult working conditions of the pandemic.
The project sparked a culture of continuous improvement within WTAIL, leading to further MfI-driven experimentation and improvement. Other clinical MDTs in the Department have now also developed summary sheets similar to ours (eg, transfusion patient management) and others will follow. An important future project is to inform development of a new Laboratory Information Management system (LIMS). The project we have described in this paper sets us up to help develop the specification for this new LIMS, since it has led us to specify the datasets and formats that we need in workup meetings. The new LIMS should enable us to populate the patient summaries automatically and allow us to address the remaining currently necessary waste (generated by the TXU subsystem).
Ethics statements
Patient consent for publication
Acknowledgments
FM conducted this work as part of the Quality Improvement unit of the Higher Specialist Scientist Training Programme, run by Alliance Manchester Business School of the University of Manchester and the Manchester Academy for Healthcare Scientist Education (MAHSE), on behalf of the National School of Healthcare Science, part of NHS Health Education England.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @FelicityNJMay
Contributors FM, JP, ED and SD made substantial contributions to the design of the work. FM performed the collection, analysis and interpretation of data. FM drafted the work with the help of NP and MTR. All authors reviewed the draft. FM is the guarantor of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.