Article Text

Abstract
Introduction A well-designed ambulatory emergency care (AEC) can alleviate demand for inpatient beds by reducing admissions or supporting early discharges. Increasing service demands and workforce gaps present major challenges to surgical departments. Physician’s associates (PAs) have been suggested as one way to address this, but previous barriers include lack of job role clarity, and inability to prescribe or request ionising radiation. An AEC clinic using PAs supported by senior decision-makers could improve patient care and provide workforce stability alongside a new capacity for successful PA positions.
Methods An emergency surgery AEC pathway was introduced to a single centre in anticipation of a second COVID-19 wave. All emergency surgical referrals were prospectively collected over 3 months (November 2020 to February 2021) with minimum 30-day follow-up. The primary aims were to evaluate clinical outcomes and success of a new AEC PA role.
Results A total of 175 patients were entered into the study. The median time from request for senior review to treatment decision was 26 min (IQR 9–62 min). The primary discharge rate was 38.3% (n=67), while the overall discharge rate without needing admission was 84% (n=147). Of the total 28 (16.0%) patients requiring admission, 18 (10.3%) were clinically appropriate. Four patients represented with Clavien-Dindo Grade II complications and above: two grade II (1.1%) and two grade IIIb respectively (1.1%). The role of the PA was well defined with no team discord. No patient complaints were received.
Conclusion During the COVID-19 pandemic, an emergency surgery AEC pathway was implemented by combining a PA with a senior decision-maker, enabling fewer emergency admissions and significantly reduced time-to-reach-treatment decisions. This in turn facilitates bed-flow and minimises delays in patient treatment. The use of a well-defined PA role in this setting shows initial success and should be considered as a long-term role.
- ambulatory emergency care
- surgical acute clinic
- physician’s associate
- early facilitated discharge
- COVID-19
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- ambulatory emergency care
- surgical acute clinic
- physician’s associate
- early facilitated discharge
- COVID-19
Introduction
The concept of ambulatory emergency care (AEC) was introduced over 10 years ago by the National Health Service Institute for Innovation and Improvement (NHSI), with its major objective to reduce the need for emergency admissions. The NHSI has previously estimated that one in six emergency admissions could be avoided if referred to an AEC pathway.1
In general, surgery many conditions are acute but not immediately life-threatening, and <10% require major surgical intervention.2 More recently, acute surgical clinics have been recommended in a joint document by the Association of Coloproctology of Great Britain and Ireland, Association of Upper Gastro-intestinal Surgeons and Association of Surgeons of Great Britain and Ireland after evidence suggests that, when front-loaded with a senior clinical decision maker, parallel AEC clinics can reduce emergency admissions by 20%–30%.2
The Surgical Emergency Care Network has laid out a 12-principle guide for AEC construction and integration into departments.3 These clinics can not only improve patient flow, but provide patients with both sound assessment and rapid access to imaging and further investigative results.4 Moreover, the COVID-19 pandemic has necessitated re-evaluation of admission criteria, both to facilitate inpatient beds but also to reduce the risk of harm to patient’s from COVID-19 contraction within hospital.
In emergency surgery services, common acute presentations can create high service demands on already stretched services. The NHS Five Year Forward View laid out a goal to deliver new models of care ‘breaking out of the artificial boundaries between hospitals and primary care, between health and social care, between generalists and specialists’.5 However, to continue to safely and adequately meet this demand, reshaping of current workforce models is required. It has been suggested that one way to meet these challenges is by implementation of physicians’ associates (PAs) to departments.
Physicians’ associates are medically trained ‘dependant’ healthcare professionals who work with supervision of doctors or surgeons6 7 but are able to work autonomously with appropriate support. They were launched on the basis of the consistency in cover and stability they could provide to medical or surgical teams. If employed long term, they offer an opportunity for stability to surgical teams in the face of frequent trainee rotations, as well as a point of continuity that could benefit patient-centred care.7 There is evidence that support workers such as PAs can not only provide high-quality patient-centred care, but reduce workload pressures on specialist qualified staff.7 However, trusts employing PAs have consistently voiced frustration at their inability to prescribe and request ionising radiation, and this has been a factor in discontinuing temporary postings.6 7 Furthermore, there is a lack of role clarity which can cause uncertainty around job responsibilities and cause team discord.8
An emergency general surgery AEC pathway was introduced to a central London hospital in anticipation of a second wave in the COVID-19 pandemic. The primary aims of this project were to evaluate its clinical outcomes and to evaluate the success of a new AEC physician’s associate (PA) role supported by senior clinical decision-makers.
Methods
Study design and participants
A surgical AEC pathway was introduced to a single central London centre in anticipation of the second wave of the COVID-19 pandemic and was adherent to the Surgical Emergency Care Network’s 12-principle toolkit.3 Prospective data was collected from all surgical AEC referrals made within a 3-month study period, from the pathway’s commencement 10 November 2020 to 10 February 2021. A minimum 30-day follow-up period was set to ensure adequate data capture for patient complications. Working age was defined as 16–65 years old.
Patients were referred to AEC following first attendance at Accident & Emergency (A&E) Department, Urgent Care Centre (UCC) or their general practitioner (GP), or as part of early facilitated discharge (EFD) from an inpatient admission. Referrals were made in real time using an electronic referral form, filled in by the relevant clinician via the trust’s electronic healthcare records (EHR) platform (Cerner, Missouri, USA). Referring clinicians could access the AEC pathway guidelines at the point of referral, via the institutional intranet. These guidelines outlined the AEC admission criteria, as well necessary safety-netting advice to be given to patients. Patients were required to provide an accessible telephone number. The complete AEC pathway and referral criteria can be seen in figure 1.

Summary of AEC pathway and referral criteria. AEC, ambulatory emergency care; A&E, Accident & Emergency Department; UCC, Urgent Care Centre; GP, general practitioner.
Patients referred to AEC were advised to attend at a specific appointment time between 8:00 and 16:00 hours Monday to Friday. On arrival, referrals were reviewed by a surgical PA, including being clerked with a full history and review of appropriate blood tests and imaging. Subsequently, referrals then had a senior clinical review by a consultant or specialty registrar emergency general surgeon. All AEC encounters were documented on the patient’s EHR, with a letter documenting the consultation sent to the patient and their general practitioner (GP). Patients who did not attend (DNA) despite a minimum of three attempted contacts on the telephone number provided were recorded as DNA and discharged.
An AEC consultation had the following potential outcomes: discharge, further AEC clinic appointment and discharge, surgical intervention (either under local or general anaesthetic), referral to another specialty (including multidisciplinary team (MDT) referrals) or admission. Surgical operations took place in either the ‘Same Day Emergency Care’ (SDEC) day case list or in the emergency National Confidential Enquiry into Patient Outcome and Death (NCEPOD) theatre. Cases were deemed suitable to take place in SDEC based on availability and in line with NHS guidelines.9
Clinical outcome analysis
Clinical presentations appropriate for AEC referral were categorised under; right upper quadrant (RUQ) pain, right iliac fossa (RIF) pain, left iliac fossa (LIF) pain, abscess (perianal), abscess (non-perianal), hernia (if no signs of obstruction or compromised blood supply), wound review and EFD or ‘other’.
Admissions were deemed clinically necessary if the patient was showing signs of clinical deterioration, or required an emergency surgical, interventional radiological or endoscopic intervention.
Data collection and statistical analysis
All collected data points were analysed using Microsoft Excel V.16.47.1.
Results
Demographics
A total of 175 emergency general surgical patients were referred to the AEC pathway during the 3-month study period. Of these referrals, 79 (45%) were male and 96 (55%) were female. The mean age of male and female patients was 41.82 (SD 16.03) and 41.83 (SD 18.57) years, respectively (table 1). The majority of patients referred were of working age: 70 (88.6%) males, 83 (86.5%) females.
Patient demographics
Clinical indications for AEC referral
Overall, there were: 61 (34.9%) RIF pains, 33 (18.9%) RUQ pains, 18 (10.3%) non-perianal abscesses, 13 (7.4%) perianal abscesses, 16 (9.1%) wound reviews, 10 (5.7%) EFD, 6 (3.4%) LIF pains and 5 (2.9%) hernias. There were additionally 13 (7.4%) ‘other’ reasons for referral, which included abdominal collection (n=2), colorectal cancer (n=1), fistula (n=3), foreign body in rectum (n=1), lymph node needing biopsy (n=1), haemodynamically stable rectal bleeding (n=3), sarcoma (n=1) and dysphagia (n=1). Nine referrals (5.1%) were inappropriate and did not meet AEC criteria, however, of these only one required admission for observation.
Clinical outcomes and patient safety
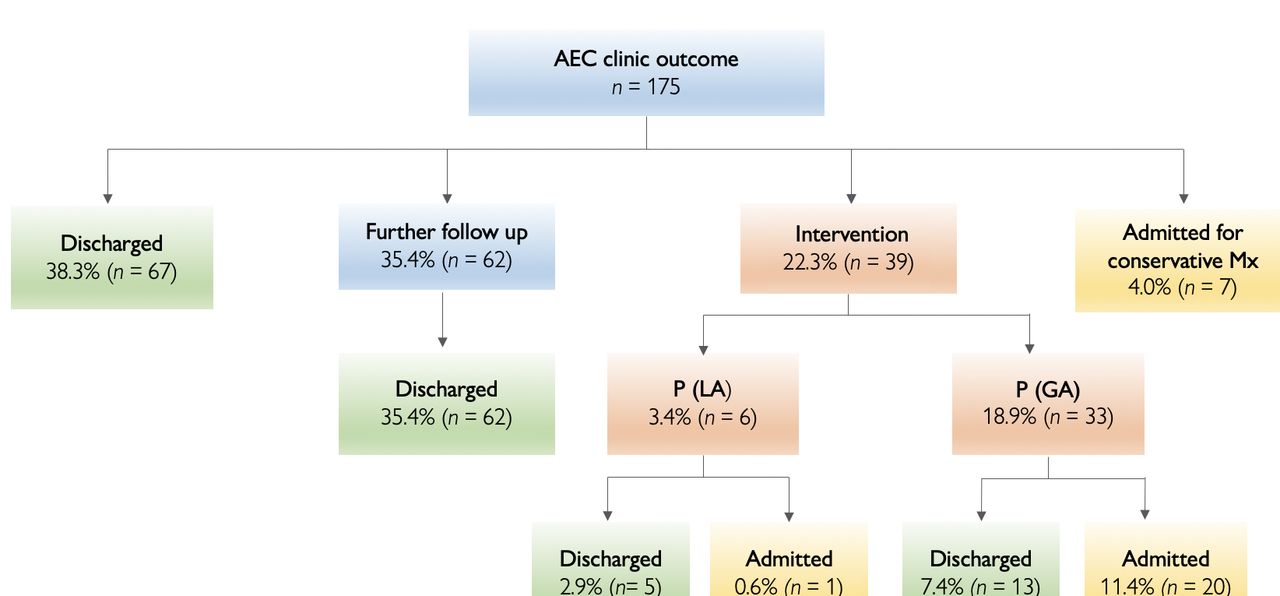
The median time from request for senior review to senior treatment decision was 26 min (IQR 9–62 min). The primary discharge rate was 38.3% (n=67, including 6 DNAs). A further 62 (35.4%) patients were able to be discharged after a follow-up AEC appointment (figure 2), obviating the need for an admission overnight. Of these, 10 patients were booked for a future elective procedure, all of which were laparoscopic cholecystectomies.
{kind=link}
{kind=link}
Clinical outcomes from AEC. AEC, ambulatory emergency care; P(GA), procedure under general anaesthetic ; P(LA), procedure under local anaesthetic.
A total of 39 (22.3%) patients required surgical intervention; 6 (3.4%) patients required a procedure under local anaesthetic (P(LA)) and 33 (18.9%) required a procedure under general anaesthetic (P(GA)). Of the P(LA) patients, five (2.9%) were discharged the same day and one (0.6%) required admission. Of the P(GA) patients, 13 (7.4%) were discharged the same day and 20 (11.4%) required admission. A further seven (4.0%) patients were admitted from AEC for conservative management. Of the total 28 (16.0%) patients requiring admission, 18 (10.3%) were clinically appropriate. For 10 (5.7%) patients, admission could have been avoided: 4 were admitted due to the referring clinician being unaware of the AEC pathway, one due to a COVID-19 test delay and five due to no availability on the SDEC list that day.
In total, there were nine representations to A&E within 30 days following discharge from AEC. According to the Clavien-Dindo Classification, there were 5 grade I complications and were discharged after review with no imaging required. There were 2 grade II complications (1.1%); one patient had a UTI and was discharged with oral antibiotics, and the other worsened cholecystitis who was admitted for intravenous antibiotics. There were 2 grade IIIb complications (1.1%). Both were patients with acute appendicitis who had been counselled and opted for conservative management and discharged from AEC, who then subsequently represented and underwent a laparoscopic appendicectomy in a timely fashion with no complications. No patient complaints were received during this period.
Discussion
A well-designed AEC may alleviate the demand for inpatient beds by reducing admissions through A&E streaming to the AEC pathway or supporting early discharges by offering early follow-up. There are increasing pressures on senior staff to meet NHS targets and service demands and two major challenges present itself to any surgical department; growing workforce gaps and an NHS budget that is not in keeping with the healthcare needs of a growing population. A physician associate AEC clinic with senior-decision maker support may be one way to address these challenges.
Patient outcomes
A carefully thought out AEC can reduce the time-to-treatment-decision for patients, reduce inpatient admissions and support early discharges to facilitate patient flow.4 Our senior-led ambulatory emergency surgical clinic found the primary discharge rate was 38.3% and an overall discharge rate (never requiring admission) of 84% (n=147). Our AEC also found a median senior decision-making time of just 26 min (IQR 53 min) meaning minimal delay to patient’s treatments.
This is higher than previously reported discharge rates; Kazem et al10 report a primary discharge rate for all emergency surgical referrals of 29% (SD 3.44%) when a dedicated senior surgeon was attached to their surgical ambulatory care unit. This was a statistically significant increase from their previous discharge rate of 17% when no SACU service existed, and 20% with an SACU present but no senior decision maker input.10 The time-to-senior-review was also considerably higher at mean 131 min (SD = 12.32). In another 50 patient audit, the second-limb of which happened to coincide with the first COVID-19 lockdown, it was reported that in-patient admission following AEC review was reduced to 14 (28%) from 20 (40%).11 However, while this is encouraging, the small sample size and observational nature limit further conclusions that can be drawn from this.
Our findings are also consistent with that reported abroad; in an Australian fast-tracked abscess service total length of stay was significantly reduced from 1.7 to 0.34 days.12 In the USA, Frazee et al have suggested that outpatient laparoscopic appendectomy should indeed be the standard of care for simple appendicitis, with 305 of their 345 patients (88%) able to be managed as a same day surgery.13
Our AEC pathway was deemed safe with no patient complaints and only four patients representing to the emergency department with Clavien-Dindo grade II complications and above within a minimum 30-day follow-up period. Overall, these patient outcome findings are encouraging, and particularly pertinent given the COVID-19 pandemic. This AEC was implemented just prior to the second wave of COVID-19 infections in London and thus its utilisation may mitigate indirect, but potentially fatal, patient harm through the risk of COVD-19 transmission as an inpatient during this time, as well as the morbidity and mortality from pandemic-related delays to treatment.14 15
Role of physician’s associates
Crucially, our AEC clinic PA role addresses the most well described problems when PAs are attached to surgical teams; lack of job role clarity, lack of prescribing and lack of ability to request ionising radiation.6–8 16 17
The PA role in our AEC was predominately clerking based, however, if medications were required (for example analgesia) our surgical team was able to prescribe remotely due to our EPR system, which has a remote prescribing ability. However, in hospitals without this ability, medical AEC doctors and prescribing nurses present in the clinic could be utilised. Any ionising radiation required was requested by the doctor contemporaneously when referring to AEC, and, if requested out of hours or requiring radiologist discussion, this was carried out by the next day surgical team in a timely manner.
PAs can also provide an educational role, directly teaching and also by easing time-pressures on junior doctors so they can attend formal teaching sessions.6 7 In the case of surgical departments, this time-relief can be spent in the operation room helping to reach required procedural competencies. The PAs role was clearly defined and communicated, with no team discord. Thus, the role of our PA in AEC has been deemed initially successful but requires ongoing evaluation with qualitative analysis. This AEC PA role has the potential for multiple applications pan-specialty and may provide a new long-term capacity for PA placement in departments where previously their integration has been unsuccessful.
Potential cost-efficiencies
A total of 147 patients avoided admission over this 3-month period. The 2020–2021 NHS national tariff workbook sets a cost of a non-elective admission for abdominal pain without intervention is £610, while the cost of a non-elective admission for abdominal pain with intervention is £2366.18 Of those admitted (n=28), 18 were clinically necessary, only for 10 patients could admission have been avoided. This could be lowered with further clinician education, as four were admitted due to the referring clinician being unaware of the AEC pathway in the first weeks of AEC commencing.
A well-run AEC pathway potentially has huge cost-savings for surgical departments and could be a way to ensure their sustainability. Unfortunately, we were not able to carry out a formal cost-analysis comparison for the AEC pathway; one of the challenges faced was that it was launched in November 2020. Thus, it was felt that there was likely to be changes in A&E practice due to the second wave of the COVID-19 pandemic rendering a ‘before and after’ analysis of how many patients would have avoided admission if they were seen in the A&E without AEC versus with inaccurate.
Furthermore, in the UK the NHS sets A&E an operational standard whereby patients attending A&E should have a decision made about their treatment (admission, transfer or discharge) within 4 hours. A ‘breach’ is said to have occurred when this decision is made after the patient has spent longer than 4 hours in A&E and can incur fines. Thus, a surgical “breach” is when A&E refers a patient with suspected surgical pathology to the emergency surgical team outside of the 4-hour target. If the patient meets the criteria laid out in figure 1, the patient can be triaged directly to AEC, and for the purposes of A&E’s patient tracking counts as having made a decision about patient care, helping them to meet this 4-hour operational standard. Our referral to AEC pathway had a surgical A&E breach rate of 4.6% (n=8).Thus, the ability for emergency departments to refer straight to the AEC pathway may reduce costs for trusts if there is a consequential reduction in breach rate, but this requires further exploration.
This report shows encouraging initial results that an emergency surgical AEC clinic may help offset service demands. This study has several limitations however the results indicate that further studies may be worthwhile.
It was carried out in a single centre with a dedicated emergency general surgery service, which may limit generalisability. Regarding safety-profiles we acknowledge there may be a limited number of patients who re-presented to alternative A&Es if complications occurred. There were no patient complaints during the study period, however in future a qualitative analysis of patients’ AEC experiences would be beneficial to improving services.
Future reports could also look to identifying which factors predispose patients to risk of AEC pathway ‘failure’, for example, unnecessary admission or operational wait time on an NCEPOD rather than SDEC list.
There was good team rapport with the AEC PA, however, there was no formal analysis of their experience. In future this would be done ideally at multiple time points, to ensure role satisfaction is continuing over time and with new junior doctors rotating onto the team.
A cost analysis and comparison of A&E breach rates before and after AEC pathway implementation was not able to be performed, as it was felt results would be inaccurate due to pandemic-related changes to A&E practices. However, as things return to some semblance of normality, this could be evaluated in future projects. This may be best done during the addition of another surgical specialty to the pathway, for example, an equivalent pathway for urology.
Conclusion
During the COVID-19 pandemic, an emergency surgery AEC pathway was implemented by combining a PA with a senior decision-maker, enabling fewer emergency admissions and significantly reduced time-to-reach-treatment decisions. This in turn facilitates bed-flow and minimises delays in patient treatment. The use of a well-defined PA role in this setting shows initial success and should be considered as a long-term role.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study was reviewed and prospectively approved by our local audit and service evaluation department (Chelsea and Westminster NHS Foundation Trust, London, UK. Project registration number PCD937. Patient-specific consent was not deemed necessary for this study by the reviewing body.
Footnotes
Twitter @edison_marie
Contributors MAE was primary author. MAE and BW performed statistical analysis. BW and DA performed data collection. NB was involved in concept and initiation of the AEC pathway. All authors were involved in providing critical revision of the manuscript prior to submission. MAE and NB are joint guarantors of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.