Article Text

Abstract
Background and purpose There is conflicting evidence regarding whether physicians’ clinical experience affects healthcare quality. Knowing whether an association exists and which dimensions of quality might be affected can help healthcare services close quality gaps by tailoring improvement initiatives according to physicians’ clinical experience. Here, we present a systematised review that aims to assess the potential association between physicians’ clinical experience and different dimensions of healthcare quality.
Methods We conducted a systematised literature review, including the databases MEDLINE, Embase, PsycINFO and PubMed. The search strategy involved combining predefined terms that describe physicians’ clinical experience with terms that describe different dimensions of healthcare quality (ie, safety, clinical effectiveness, patient-centredness, timeliness, efficiency and equity). We included relevant, original research published from June 2004 to November 2020.
Results Fifty-two studies reporting 63 evaluations of the association between physicians’ clinical experience and healthcare quality were included in the final analysis. Overall, 27 (43%) evaluations found a positive or partially positive association between physicians’ clinical experience and healthcare quality; 22 (35%) found no association; and 14 (22%) evaluations reported a negative or partially negative association. We found a proportional association between physicians’ clinical experience and quality regarding outcome measures that reflect safety, particularly in the surgical fields. For other dimensions of quality, no firm evidence was found.
Conclusion We found no clear evidence of an association between measures of physicians’ clinical experience and overall healthcare quality. For outcome measures related to safety, we found that physicians’ clinical experience was proportional with safer care, particularly in surgical fields. Our findings support efforts to secure adequate training and supervision for early-career physicians regarding safety outcomes. Further research is needed to reveal the potential subgroups in which gaps in quality due to physicians’ clinical experience might exist.
- healthcare quality improvement
- health professions education
- professional competence
Data availability statement
There are no data in this work.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Healthcare quality can be defined as ‘the extent to which healthcare services provided to individuals and patient populations improve desired health outcomes’.1 The Institute of Medicine provides an examination of the divide between good healthcare and provided healthcare.2 To describe, measure and thus improve healthcare quality, the Institute of Medicine proposed six dimensions: safety, effectiveness, timeliness, efficiency, patient-centredness and equity. More recently. WHO added ‘integrated care’ as the seventh dimension in their definition of quality in healthcare.3 Improvement of these dimensions is required to eventually ‘cross the quality chasm’.
Quality gaps exist at all levels of the healthcare system, including at the level of the treating physician. Specifically, physicians’ clinical experience and its effects on variations in healthcare quality remain disputed. A broad range of findings are reported, with reported associations varying between different medical fields.4–8 Empirically, a physician’s clinical experience is typically measured by his or her age or years in clinical practice.9 Knowing whether a physicians’ clinical experience can affect healthcare quality and which dimensions of quality might be affected can help healthcare services close potential quality gaps by tailoring improvement initiatives.
A comprehensive, systematic review within the field was undertaken in 2005 by Choudhry and colleagues; it showed an overall inverse relationship between physicians’ clinical experience and quality.10 This review is now over 15 years old; thus, an updated review could provide valuable knowledge. We, therefore, present a systematised review of recent articles that study the association between physicians’ clinical experience and healthcare quality. Our primary aim was to determine whether there is evidence of an association between physicians’ clinical experience and healthcare quality, and whether an association is attributable to the Institute of Medicine’s specific dimensions of healthcare quality. Outcome measures related to integrated care were not included as these typically measure ‘coproductive partnerships’, and thus relating these to characteristics at the level of the individual treating physician would be difficult.11
Methods
We conducted a systematised review (according to Grant and Booth12) including the databases MEDLINE, Embase, PsycINFO and PubMed. The search strategy involved combining terms that describe physicians’ clinical experience with terms that describe different dimensions of healthcare quality. The terms for the dimensions of healthcare quality were derived from the Institute of Medicine.2 A test search revealed several slightly different concepts that cover both physicians’ clinical experience and the dimensions of healthcare quality. Specifically, by using the term ‘physician experience’, we found several potentially relevant articles. Hand searching the list of references and other related articles, we found that several potentially relevant articles could only be retrieved through using the terms ‘physician age’, ‘physician seniority’ or ‘clinician experience’. We also found that some of the articles describing physician experience used caseload as a proxy. In this review, the term physician experience therefore describes years in practice, age or caseload. Each term that describes physicians’ clinical experience was combined with all the terms that describe dimensions of quality by using the operator ‘AND’. The search terms used in the final search are listed in table 1.
Search strategy
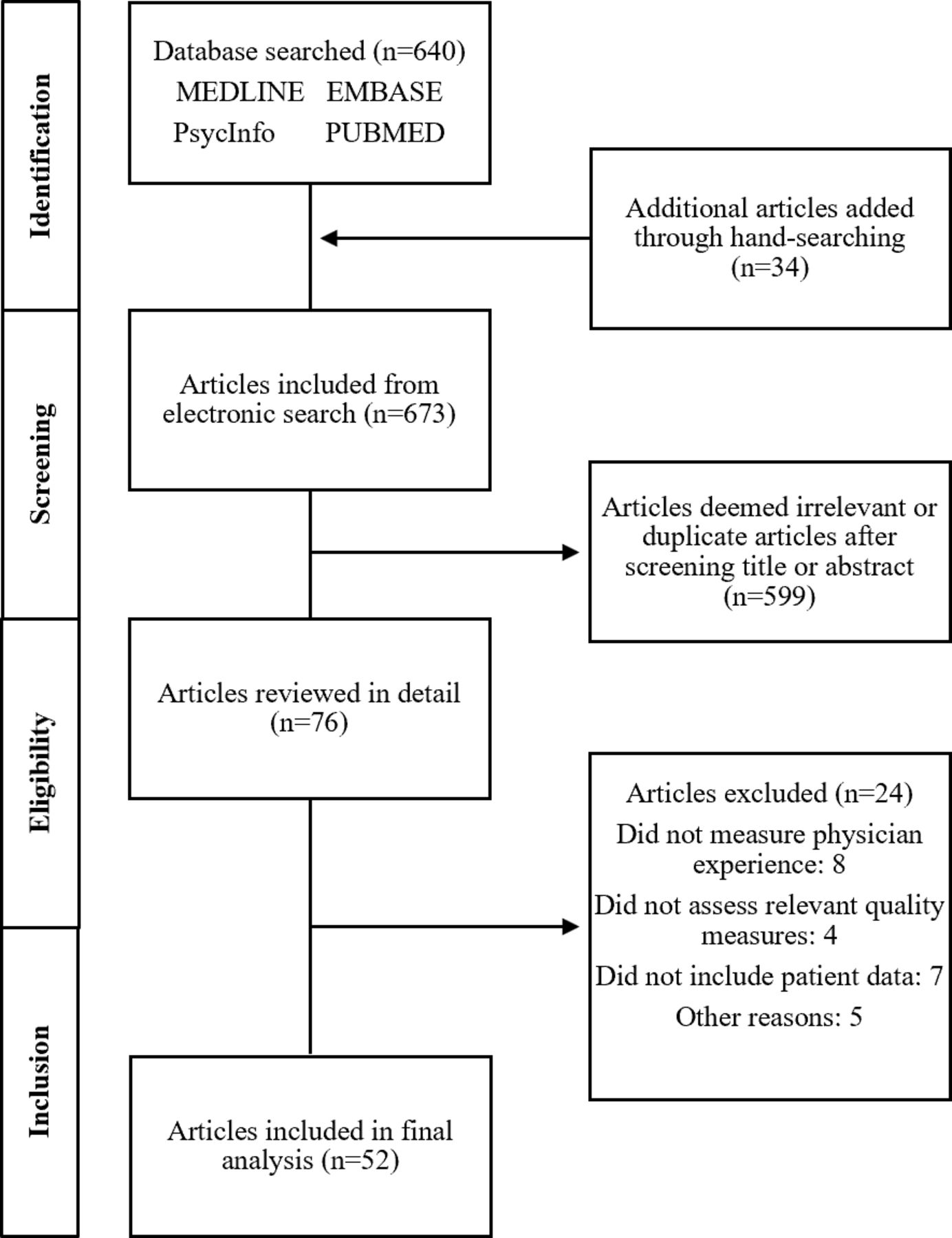
Titles and/or abstracts were screened for inclusion. After retrieving potentially relevant articles, we hand searched a list of articles listed in PubMed as ‘related to’ or ‘citing’ the previously published guiding review by Choudhry and colleagues on the subject.10 The review by Choudhry and colleagues included relevant studies before June 2004; thus, we included articles published from June 2004 to November 2020. Only original studies that assess the association between process or outcome measures that reflect one or several dimensions of healthcare quality and a measure of physicians’ clinical experience were included. For studies that assess several outcome or process measures, we included only relevant measures. The selection process is outlined in figure 1.

Selection process for the articles included in this study.
We reviewed each dimension of healthcare quality separately. Relevant outcomes from each article were thus categorised according to dimension. Descriptions of each quality dimension included in the Institute of Medicine report were used for classification.2 For example, measures of adverse events were classified as safety adherence to guidelines for treatments were classified as clinical effectiveness and the time required until treatment or diagnosis was classified as timeliness. Some outcome measures were not easily classified into specific quality dimensions. For example, readmission is a complex quality indicator that might reflect several dimensions of quality.13 Complex outcome measures were therefore classified to the best of our abilities and, in the case of readmissions, as a measure of safety.
For each included study, we reported the following parameters: study design, medical field, sample size, key results and the nature of the association. The nature of the association was classified as either positive (proportional relationship between measures of physicians’ clinical experience and healthcare quality), neutral (no association) or negative (inverse relationship between measures of physicians’ clinical experience and healthcare quality). Whenever some but not all outcome measures from a single study were associated with measures of physicians’ clinical experience, the evaluation was classified as either partially positive or partially negative. We did not perform a formal meta-analysis of quantitative results, assess the validity of our search strategy or formally assess the quality of the included studies.
Results
Fifty-two studies were included in the review sample. Thirty-four of the included studies originated from the USA. Fifty were observational; of these, 36 were retrospective cohort studies. With regard to medical fields, 12 studies assessed different surgical fields; 3 assessed psychiatrists; and 6 assessed general practitioners; the remaining 31 studies assessed disciplines within internal medicine or a mixed group of physicians. Details of the study design and medical fields are presented in online supplemental table 1.
Supplemental material
The 52 included studies reported 63 evaluations (groups of, or single, relevant outcomes) of the association between physicians’ clinical experience and healthcare quality. Twenty-seven (43%) of the 63 included evaluations reported a positive or partially positive association between physicians’ clinical experience and healthcare quality; 22 (35%) found no association; and 14 (22%) evaluations reported a negative or partially negative association (figure 2).
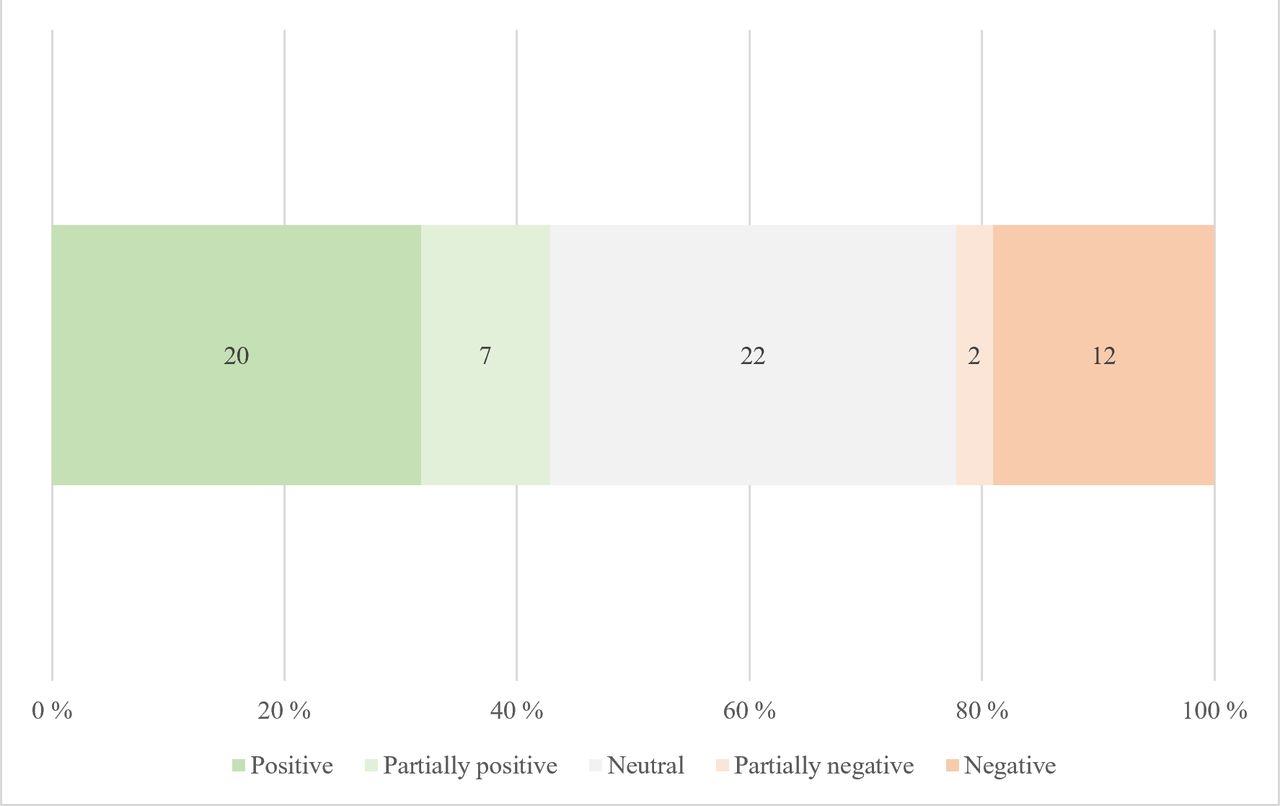
Overall frequency and the nature of associations between physicians’ clinical experience and healthcare quality. A total of 63 associations from 52 articles were included;positive: a proportional relationship between healthcare quality and physicians’ clinical experience; partial: some but not all outcomes within an evaluation pointed in one direction; negative: inverse relationship between healthcare quality and physicians’ clinical experience.
Safety
We included 11 studies that assessed outcome measures related to safety.6 14–23 Of these, six (54%) found a positive or partially positive association with physicians’ clinical experience, and five (46%) were neutral (see online supplemental table 1 and figure 3). Four out of the six (67%) studies that found a positive association included only surgical patients. The study by Epstein and colleagues was the most comprehensive of the included evaluations of safety; they analysed the association between various complications after birth deliveries (vaginal and caesarean) and physicians’ years in practice.18 A 0.21% reduction in complication rates per year in the first decade of training (95% CI −0.23 to −0.19) was found, a 0.11% reduction in the second decade and a 0.05% reduction in the third decade. The association between years of training and reduced complication rates was thus positive and most pronounced during the first decade of training.

{kind=link}
{kind=link}
{kind=link}
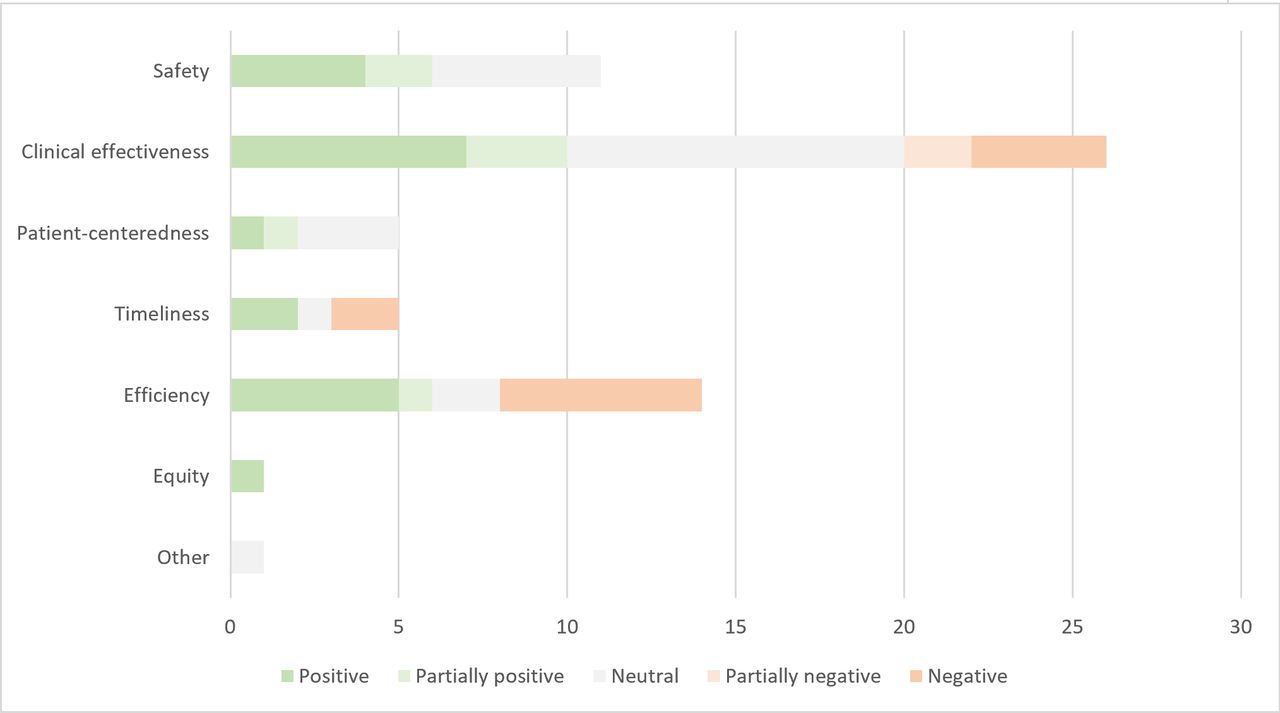
Frequency of associations grouped into six healthcare quality dimensions. A total of 63 associations from 52 articles were included; positive: proportional relationship between quality and physicians’ clinical experience; partial: some but not all outcomes within an evaluation pointed in one direction; negative: inverse relationship between quality and physicians’ clinical experience.
Another study by Berk and colleagues evaluated 829 emergency room cases that involved an adverse outcome (eg, death, concerns from staff or family, readmission, etc).16 By peer review, cases where low healthcare quality could be attributed to a cognitive error by the treating physician were identified. The authors found that emergency physicians with 1.5 years of experience or more were significantly less likely to make an error (Relative Risk=0.66, 95% CI 0.48 to 0.91). This is the only included study that performed a comprehensive review of potential low-quality healthcare cases before attributing them to physician errors.
Five other studies did not find an association.14 19 21–23 This included the only interventional study with a quasi-experimental design by Southern and colleagues.21 In this study, 30-day readmission rates and years in practice (in 5-year increments) were studied; no significant association was found across different age groups. None of the included studies showed a negative association.
Clinical effectiveness
We included 26 studies that assessed outcome measures related to clinical effectiveness.6–8 14 21 24–44 Of these, 10 (38%) found a positive or partially positive association with physicians’ clinical experience; 10 (38%) found no association; and 6 (24%) were negative or partially negative (see online supplemental table 1 and figure 3). The study by Satkunasivam and colleagues was one of the largest studies, including 1 159 676 patients who had been treated by 3314 surgeons.6 They found a reduced risk of 30-day mortality for each 10-year increase in surgeon age and for the surgeons with the highest case volumes.
Several other studies assessed both case volume, age, or years of training as a measure of physicians’ clinical experience, with conflicting results. Chai and colleagues analysed the association between thoracic surgeons’ age and mortality for 3766 patients and found lower mortality rates for surgeons>45 years old regardless of caseloads.28 Khatana and colleagues studied 356 interventional cardiologists and 1 45 247 cases with regard to deaths per 100 cases.7 They found a higher caseload, but not the number of years since medical school training, to be associated with reduced mortality.
A large study by Conway and colleagues included 36 271 patients with 66 933 emergency room admissions and analysed the association between the emergency physician’s years of experience and mortality.29 The study found a reduced risk of 30-day mortality for physicians with more than 20 years of experience, only for high-risk patients. This is the only included study that stratified outcomes by a patient’s risk profile.
Patient-centredness
We included five studies that assessed outcome measures related to patient-centredness.5 33 45–47 Of these, two (40%) found a positive or partially positive association with physicians’ clinical experience, and three (60%) found no association (see online supplemental table 1 and figure 3). The study by Fathy and colleagues evaluated the effect of physicians’ age on patient satisfaction; this was one of the largest studies, including 1342 ophthalmologists.45 They found that the time to the first unsolicited complaint was the highest (ie, better quality) with ophthalmologists older than 70 years. The association with age assumed an almost linear pattern for 10-year increments from the age of 30. The nature of the complaints (eg, communication, care, treatment, etc) was similar across all age groups.
With regard to technical procedures, Seely and colleagues included physicians performing stereotactic biopsies and studied the association between patient-satisfaction scores (with regard to pain and bruising from the procedure) and the treating physicians’ years in practice.47 For stereotactic vacuum-assisted biopsies, they found that patients of more experienced physicians reported significantly less pain and bruising (p=0.0013).
Timeliness
We included five studies that assessed outcome measures related to timeliness.4 14 32 40 41 Of these, two (40%) found a positive association with physicians’ clinical experience; one (20%) was neutral; and two (40%) were negative (see online supplemental table 1 and figure 3). The studies that found a positive association had a prospective design, but the advantages in the design might have been offset by the larger number of patients included in the two retrospective studies that found a negative association.4 14 32 40 Both the study by Harvey and colleagues and the study by Li and colleagues included emergency physicians and analysed the association between waiting times in the emergency room and physicians’ clinical experience.32 40 Harvey and colleagues concluded with shorter waiting times for the patients of more experienced physicians, while Li et al had the opposite conclusion.
The only study that assessed timeliness according to differences in diagnostic accuracy in a technical procedure was performed by Mehrotra and colleagues.4 They included 104 618 patients and assessed adenoma detection rates in gastroscopy. They found a mean detection rate that was 6% higher in physicians who had less than 9 years since their residency completion (p=0.004) compared with physicians who had 27–51 years of practice.
Efficiency
We included 14 studies that assessed outcome measures related to efficiency.21 24 29 40 48–57 Of these, six (43%) found a positive or partially positive association with physicians’ clinical experience; two (14%) found no association; and six (43%) were negative (see online supplemental table 1 and figure 3). None of the included studies assessed surgical patients; otherwise, the included studies represented a broad range of settings.
Schwartz and colleagues performed one of the largest studies, including 3 159 834 patients and 41 773 generalist physicians.55 They defined 17 primary care-associated, low-value services (minimum clinical benefit) and counted the annual rates of these services per 100 patients per year. After including age as one of several physician characteristics, they found a significant increase in low-value services per 10-year increase in age, thus concluding with a negative association between age and healthcare quality. This is the only included study that adjusted for within-region and within-organisation variations.
Two of the included studies assessed costs per case as a measure of efficiency, and both showed a positive association. Cournane and colleagues included 19 295 emergency department patients and analysed the association between years of experience and costs per case.48 Five-year increments of increased experience above 15 years had a significantly reduced OR for costs below the median. Mehrotra and colleagues included 2 861 093 claims attributed to 12 724 physicians and compared the expected costs for the condition in question with the cost apparent from the claim.52 Compared with physicians with more than 40 years of experience, physicians with fewer years of experience had higher cost profile scores. Both studies, therefore, concluded that more experienced physicians had beneficial cost profiles.
Equity
Only one study with outcomes related to equity was included. The study by Essien and colleagues included 143 274 patients of both resident and staff primary care physicians.58 They collected details regarding patient’s ethnicity, insurance status, poverty and education, in addition to quality outcomes such as guideline-concordant disease management, screening, resource use and patient-reported health experience. They found that resident physicians had a higher proportion of typically underserved populations than staff physicians and that when controlling for patient factors, residents had lower scores for all quality-outcome measures, except for patient experience. The authors found that residents and staff physicians serve significantly different patient groups. The lower healthcare quality provided by residents compared with staff physicians thus represented an equity problem with typically underserved populations receiving lower-quality care.
Other
The study by Reid and colleagues could not be categorised within a specific quality dimension, as their outcome measure was a composite performance score of 124 different quality measures assessing several dimensions of quality.59 The study was comprehensive, including 1.13 million patients and 10 408 physicians from a broad range of settings. They included several physician characteristics, including age, but did not find an association between age and healthcare quality.
Discussion
In this systematised literature review of 52 studies, we found that the most frequently reported association was a proportional association between physicians’ clinical experience and overall quality of care (43%). However, a relatively large proportion of evaluations found no association (35%) or even an inverse relationship between a physician’s clinical experience and quality (22%). Regarding specific dimensions of healthcare quality, in our sample, 26 studies that assessed the associations between a physicians’ clinical experience and measures of clinical effectiveness were included. There was a substantial dispersion regarding the nature of the associations in these studies, with similar proportions of studies reporting a proportional, neutral and inverse association. A similar pattern emerged for the 14 studies that assessed measures of efficiency. For the 11 studies that assessed measures of safety, most reported a proportional association between physicians’ clinical experience and measures of safety (54%), with no inverse associations found. This was primarily driven by studies that assessed surgeons. For patient-centredness, two of the included studies were positive (40%), with no negative association, but only five studies were included overall, and most of these (60%) found no association. Only one included study assessed equity and found a positive association. Due to the heterogeneity of the included studies and the relatively small differences in proportions, we cannot conclude with evidence of an association between physicians’ clinical experience and overall healthcare quality. For different dimensions of quality, our results indicate that, for outcome measures that reflect safety, there is a proportional association between physicians’ clinical experience and quality. For the other dimensions of quality, no firm evidence of association was found.
Theoretically, there are plausible explanations for both a proportional and an inverse relationship between physicians’ clinical experience and healthcare quality. More experienced physicians, through the accumulation of tacit knowledge and skills, might provide higher-quality care than their less experienced peers. However, an experienced physician might also provide poorer quality due to a lower willingness to adopt new therapies, the ineffectiveness of continuing medical education programmes or even neurocognitive changes associated with advancing age.60 An additional explanation for studies that report neutral or inverse associations is related to the definition of physicians’ clinical experience. In most of the included studies, this was narrowly defined as either their years in practice or age, and, in a few studies, as case volume. Elstad and colleagues argue that what physicians gain over time is complex social, behavioural and intuitive wisdom, as well as the ability to compare present-day patients against similar past patients.9 This acquired understanding of patient types might lead to better care that is not captured by common quality indicators. In some instances, deliberately disregarding guidelines due to an understanding of patient types can be warranted and lead to better quality. In most studies, this potential quality contribution is overlooked, and the lack of adherence to guidelines is prematurely reported as deficient care. This highlights some of the challenges with the narrow definitions or proxies for physician experience such as age or years in practice used in most included articles. Berk and colleagues’ study was the only article in which potential low-quality cases underwent peer review before being classified as a physician’s cognitive error.16 Through peer review, the risk of overlooking increases in quality that are not captured by common quality indicators is reduced. They found a positive association between quality and a physician’s experience, and thus might support the theory stated by Elstad and colleagues.
Our findings contrast those reported by Choudhry and colleagues in 2005, indicating an inverse relationship between physicians’ clinical experience and healthcare quality.10 There are possible explanations for this. First, Choudhry and colleagues argued that their results could be due to a ‘cohort’ effect. The cohort effect in this context means that an inverse relationship between physicians’ clinical experience and quality could be due to the substantial changes that have occurred in medicine over the past decades (eg, adaptation of evidence-based medicine and quality assurance techniques). Reduced familiarity with this among the older physicians included in their review might have led to lower quality. The cohort of older physicians included in the studies that formed the basis of the review by Choudhry and colleagues (from 1966 to 2004) is probably not included in our review; thus, this disparity in quality due to a potential cohort effect is expected to be absent or less pronounced in the current review. Second, the review by Choudhry and colleagues typically included articles that assessed knowledge and adherence to diagnosis or therapy through self-reported data, while only seven of the articles reported health outcomes. Most articles included in this current review reported health outcomes. Comparing the included studies that reported only health outcomes, we found that the difference between the two reviews is less pronounced.
Other more recent literature reviews within specific clinical specialties report findings similar to this review. Melfa and colleagues conducted a review of surgical fields and found that higher volume was associated with better quality. For the individual surgeon, the results were particularly evident regarding complications.61 This result echoes our findings regarding the safety dimension. Another literature review by van der Leeuw and colleagues studied the effect of residency training and experience on patient outcomes and concluded that overall patient care appears safe and of equal quality when delivered by resident physicians compared with more experienced staff.62 This supports our conclusion that there is no significant overall association between physicians’ clinical experience and healthcare quality.
Our systematised review has several limitations. First, we included a heterogeneous group of studies that included assessments of technical and non-technical skills, early-career, and late-career, acute and elective treatments, each within a broad range of medical fields. Thus, there is a possibility that opposite effects in subgroups might have cancelled each other, masking potential associations. Second, regarding the dimensions of quality, some of the dimensions had too few studies to draw firm conclusions about associations. This is particularly the case for the equity dimension. A better search strategy might have helped include more studies. Third, our study focused on potential effects of individual physician characteristics on healthcare quality. Healthcare quality is dependant of a complex set of factors including individual factors, team factors and system factors to achieve successful outcomes. Considering the multitude of factors that might influence healthcare quality, variation attributable to characteristics of the treating physician constitutes only part of the overall variation. Fourth, the narrow definition of physician experience used in this review might have excluded articles using more sophisticated proxies for experience than age or years in practice. One could argue that including other proxies of experience, such as breadth (eg, working in a variety of different healthcare settings), would have resulted in the inclusion of articles reflecting a broader range of physician experience. Fifth, we might have introduced bias by including a large proportion of articles that cite the review by Choudhry and colleagues.10 If, for instance, studies that reported a negative association were more likely to cite this review as a confirmation of their findings, we would have overlooked the possibility of a larger effect towards positive associations. Given the large number of included studies, however, a significant bias is less likely, and it is difficult to predict its potential direction. Sixth, most of the included studies were retrospective cohort studies and thus had inherent weaknesses related to study design. Finally, regarding generalisability, almost all the included studies were from Organisation for Economic Co-operation and Development countries (the majority of these were from the USA). Thus, our findings might not be directly applicable to other settings.
Despite these limitations, our findings do suggest that an overall healthcare quality gap related to physicians’ clinical experience is either non-existent, ambiguous or no longer relevant. This has implications for future research, as more specific studies are needed to determine the potential effects in subgroups, particularly regarding equity. Furthermore, our findings suggest that there is a possible quality gap regarding the safety dimension, as physicians’ clinical experience is positively associated with safer care. This is particularly true for surgeons, and efforts to secure adequate training and supervision of novice surgeons are warranted. Finally, several of the included studies reported large variations at the physician level that could not be attributable to observable measures, such as age or years of experience.26 30 37 42 55 56 59 Physician-level individual variation is thus an important cause of disparities in healthcare quality, and explaining this variation through measures other than age or years of experience will be important in eventually addressing quality gaps.
Conclusion
We found no clear evidence of an association between measures of physicians’ clinical experience and overall healthcare quality. For outcome measures related to safety, we found that physicians’ clinical experience was proportional with safer care, particularly in surgical fields. For other quality dimensions, we found no firm evidence of an association. Further research is needed to reveal potential subgroups in which disparities in healthcare quality might exist.
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @SoffienA
Contributors SCA and KA conceived the research questions and search strategy and approved the final version. SCA performed the literature review, drafted the work and was responsible for the overall content as guarantor. KA did several critical revisions for important intellectual content.
Funding SCA is a research fellow funded by a Safer Healthcare Grant (University Research Fund). Otherwise, the authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.