Article Text

Abstract
A Lean-based improvement approach was used to complete a quality improvement project (QIP) focused on improving speed and quality of discharge of frail patients on two wards at a large teaching hospital in the UK. This was part of a national initiative to embed continuous improvement within the trust. The aim of the QIP was to improve the proportion of prenoon discharges to 33% of total patients discharged from the ward each day. An ‘improvement practice process’ followed, which included seven discrete workshops that took the QIP through four distinct phases—understand, design, deliver and sustain. Several improvement methods and tools were used, including value stream mapping and plan–do–study–act (PDSA) cycles. Ten PDSA cycles were implemented across the clinical areas, including improved planning and data collection of discharge, improved communication between nursing and medical staff, and earlier referrals to community hospitals for discharge. Improved performance was identified through the outcome metric prenoon discharges on both wards, with the average increasing from 8% to 24% on ward X and from 9% to 19% on ward Y, with no other significant change seen in other measures. Pettigrew et al’s context–content–process change model was used to structure the learning from the QIP, which included the impact of varying ward contexts, the format of conducting improvement with staff, the importance of organisational support, the need for qualitative measures, agreeing to an apposite aim and the power of involving service users. The original aim of 33% prenoon discharges was not achieved, yet there was clear learning from completing the QIP which could contribute to ongoing improvement work. This identified that the Lean-based improvement approach used was effective to some degree for improving discharge processes. Further focus is required on collecting qualitative data to identify the impact on staff, especially related to behaviour and culture change.
- patient discharge
- lean management
- hospital medicine
- quality improvement
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
This report was developed using the SQUIRE V.2.0 guidelines.1
Problem
The care of older people is complex in England,2 with many older patients accessing healthcare having frailty.3 Frailty is defined by the British Geriatric Society as ‘a distinctive health state related to the ageing process in which multiple body systems gradually lose their in-built reserves, which has the potential for serious adverse outcomes after seemingly minor stressors or change’.4
As part of a trust-wide approach to embedding continuous improvement over a multiyear period of time known as ‘Vital Signs: an Improvement Practice for the NHS’ (‘Vital Signs’), a defined patient pathway was chosen in which targeted improvement would be completed. The pathway for patients with frailty was picked first, with discharge from hospital being the initial focus area of improvement through this approach. Delay to discharge is a common theme of complaints for hospitals and is often due to overlapping processes involving multiple multidisciplinary team members. A key target which is used to quantify improved discharge from hospital in the ward setting is prenoon discharges,5 but the manner in which increased prenoon discharge is achieved varies between acute trusts. Interventions can include changes to ward rounds, preplanning discharges and workflow discharge checklists.6–8
This quality improvement project (QIP), known as the ‘discharge QIP’, focused on improving discharge within two particular wards to begin with at Queens Hospital Burton (QHB), part of University Hospitals of Derby and Burton NHS Foundation Trust (UHDB). These wards were chosen as they provided care largely for patients who were frail. Ward X was a 28-bed medical ward and Ward Y was a 20-bed, largely surgical ward, with prenoon discharges for both wards being less than 10% of the total discharge before the QIP commenced. The team was taken through a set ‘improvement practice process’, a key part of the ‘Vital Signs’ programme, employing key Lean principles and tools aimed at increasing value for the patients and removing waste.9
The initial aim of this QIP was ‘For frail patients on Ward X and Y at QHB to not be situated in acute beds for any longer than necessary by first December 2019’. This aim was made Specific; Measurable; Achievable; Relevant; Time-bound (SMART)10 by focussing on improving the prenoon discharge to 33% of patients discharged per day.
Background
There has been an increased pressure on acute care services in recent years with the number of emergency admissions of older patients (65 and over) increasing year on year since 2001, with falls being a major reason for attendance.11 12 Older patients now account for 62% of the total bed days in hospitals.13 However, it is estimated that 2.7 million bed days are occupied by older patients who are no longer in need of acute treatment, estimated at around £820 million in cost to the NHS.13
It is well documented that extended lengths of stay in the hospital for older patients can lead to worse health outcomes, such as loss of independence and reliance on others, with community-based management being the preferred option of care for these older patients who do not require acute medical treatment.3 14 15 At the trust, where improvement was taking place, there were historical issues with delays for ‘complex discharges’ accounting for hundreds of lost bed days per month, in which patients with frailty accounted for the majority.
As part of a national initiative, UHDB was successful in gaining support from NHS Improvement (NHSI) to implement a continuous improvement programme known as Vital Signs. This initiative drew on Lean principles alongside approaches such as the ‘Engineering Better Care’ report,16 with a view to supporting a culture change across the trust, embedding continuous improvement at the trust’s core rather than focussing on loosely connected improvement ‘projects’ as had been the previous approach.
‘Lean thinking’ originates from academic research investigating the productivity and practices at Toyota Motor Corporation.9 17 Lean thinking - also known as,The Toyota Production System - is founded on two main principles of "respect for people and society" and the "continuous removal of waste to deliver value to the customer".9 Throughout this article, we will refer to these principles as ‘Lean’ and the local adaptation used in this QIP as ‘Lean-based improvement approach’.
Lean has been widely used in many Western healthcare organisations such as Bolton NHS Foundation Trust and Virginia Mason Hospital18 as an organisational-wide approach which has been documented to have made successful improvements to patient care.19 Vital Signs was adapted from the traditional Lean approach as an iteration from the NHS–Virginia Mason Institute partnership approach implemented with five trusts in England, and drew on learning from this partnership.16 The trust implementing this approach had numerous attempts at making improvements in the past which were successful to varying degrees, but Vital Signs was chosen as it was seen as a way to create a standard organisational approach to improvement to drive continuous and sustainable improvement going forward.
A common criticism of case studies using Lean in healthcare is that it is not implemented across the whole patient pathway, but rather used in small and isolated areas, leading to issues with scalability and impact.19–21 For Vital Signs, in order to embed continuous improvement in a stepwise approach, patient pathways were identified for focused improvement activity known as ‘value streams’—using this targeted activity to complete improvement in an ‘inch-wide, mile-deep’ manner. Given the opportunity for improved care and efficiency across the system discussed previously, the first value stream picked was for patients with frailty admitted to the hospital, with the first focused area for improvement being the discharge process.
Timely discharge of patients more widely has been a focus of healthcare providers in England over the last decade. Efforts such as Red2Green, ‘super-stranded’ patient multiagency events and the SAFER Care bundle have made efforts to reduce the time patients spend in the hospital, which does not add value to the patient.22 23 These initiatives have gone someway to implementing Lean principles such as visually managing performance with Red2Green or smoothing flow through the hospital by discharging patients earlier in the day. Nonetheless, these seemed to focus on isolated areas rather than viewing the macrosystem of the hospital or trust systems. Discharge of complex patients such as those with frailty can be especially complicated due to the number of agencies. Bauer et al24 suggests that more timely discharge of frail patients requires the input of all people involved in the process including service users and carers.
Measurement
Through the improvement practice process adopted through Vital Signs, a suite of measures were identified across different areas associated with discharge including process, outcome and balancing measures.25
Outcome measure
The primary outcome measure was prenoon discharges for the wards involved. This was chosen as this is a relatively common national target; 33% of total discharges from acute care ward beds are supposed to be discharged before 12 noon (prenoon discharge).
The length of stay (LoS) of patients for the two acute care wards was also captured as an outcome metric. If a patient only spent time on the ward that was necessary, then the overall discharge would happen in an expedited manner. An additional reason for collecting these data was to act as a balancing measure to ensure that prenoon discharge figures were not ‘gamed’. This is where patients were held back from evening discharge and instead discharged the following morning to inflate figures.26 27
Process measure
The process measure collected was the number of patients who were scheduled to be discharged versus actual patients discharged. Although not the overarching aim, by scheduling patients to be discharged the day before as well as reviewing plans for discharges from the previous day, this would indicate some level of discharge planning was being completed, increasing the likelihood of increasing prenoon discharge. To achieve the 33% target, Ward X was required to discharge one patient prenoon per day and Ward Y was required to discharge two patients on average.
Balancing measure
The 30-day readmission rate was collected for both wards to ensure rapid discharges were not causing an increase in return to the hospital. In addition, the number of discharges completed per day was also captured as a balancing measure to ensure there was no adverse effects on the total number of patients discharged.
Analysis
Automated weekly reports were set up and shared with all the QIP team throughout the study period to support dissemination of information and identification of improvement as well as sustainability of change. The use of statistical process control charts would support the identification of when there was a change in the measures especially in relation to the interventions which were being implemented.
Design
As a central part of setting up the QIP, a core team was developed which consisted of several members of trust staff: ‘executive sponsor’, who was identified as the chief operating officer; a ‘clinical lead’ was the associate medical director at the time; ‘process lead’ was the deputy director of operations; ‘improvement coordinator’ was a member of the trust transformation team; and an external NHSI Lean transformation consultant oversaw the process. The Lean transformation consultant provided several training modules to the other members of the core trust staff, which introduced Lean principles, tools and behaviours as well as explained the improvement practice process prior to the commencement of the QIP. Other members of staff involved in the QIP through the appropriate clinical areas underwent appropriate training during, rather than prior to the workshops.
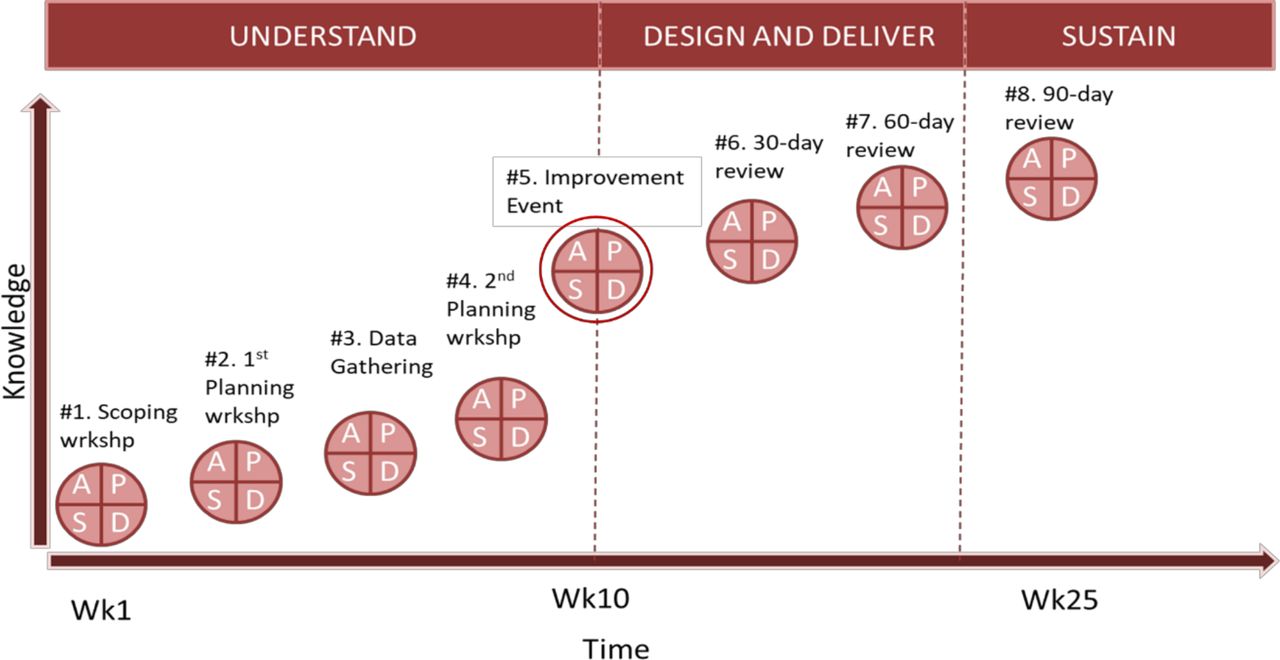
The improvement practice process used for the QIP included seven structured workshops over a 25-week period, which included a period of data gathering and staff engagement to support improvement. This process was broken down into several sequential improvement phases: ‘understand’, ‘design’, ‘deliver’ and ‘sustain’ and is visualised in figure 1.16 These workshops were also developed and tested using plan–do–study–act (PDSA) methodology due to the first time being completed in the trust in question, but they will not be discussed in this article.28

Schematic of the improvement practice process followed to complete the discharge QIP. QIP, quality improvement project; Wk, Week; wrkshp, workshop.
Workshop 5 of the improvement practice process was the main catalyst for improvement (usually referred to as a rapid improvement event (RIE))29 (figure 1). As part of this workshop, Ward X involved two medical consultants, three ward nurses, a discharge coordinator, occupational and physical therapists and a pharmacist with varying levels of involvement in follow-up workshops. Ward Y did not involve medical staff as part of the QIP, however involved two ward nurses, a pharmacist, a physiotherapist and an occupational therapist. Additional staff outside the dedicated ward staff were also involved in the improvement practice process, including operational managers, dedicated discharge team and community hospital nurses. This engagement and involvement was vital to define value for our staff and service users.
This workshop (RIE) used value stream mapping and fishbone diagram technique, and other common improvement tools supported the identification of several problem areas requiring improvement split between the clinical areas.30 31
These included
Data collection of planned versus actual discharges.
Communication with patients and relatives.
Ward communication.
Discharge documentation.
Community hospital referral process.
Table 1 outlines the PDSA cycles which were used to test and develop the interventions through the RIE and during the subsequent follow-up workshops. Each of the problem areas identified during this workshop were addressed to varying degrees on the respective ward areas.
Ward X and Y PDSA cycles completed over discharge QIP
Patient and public involvement (PPI)
Service users were involved in workshops 5–8 and were central to developing and critiquing ideas, ensuring the patient’s voice was always heard and defining value for the customer. As the service users were partners on several trust boards, they supported feedback outside of the workshops to a wider audience in addition to presenting their findings during their work to executive staff.
Strategy
PDSAs were used to implement interventions on the wards (table 1). These varied from capturing data in a more effective way on the wards through to improving communication between medical and nursing staff regarding discharge readiness. Five PDSAs were completed on the two wards over a 4-month period. Follow-up workshops were held at 30, 60 and 90 days post the RIE. This was to maintain momentum and readdress problem areas which had not been reviewed yet. Selected staff discussed earlier from each of the ward areas were identified to attend these workshops and implement changes in between workshops.
Results
Ward X
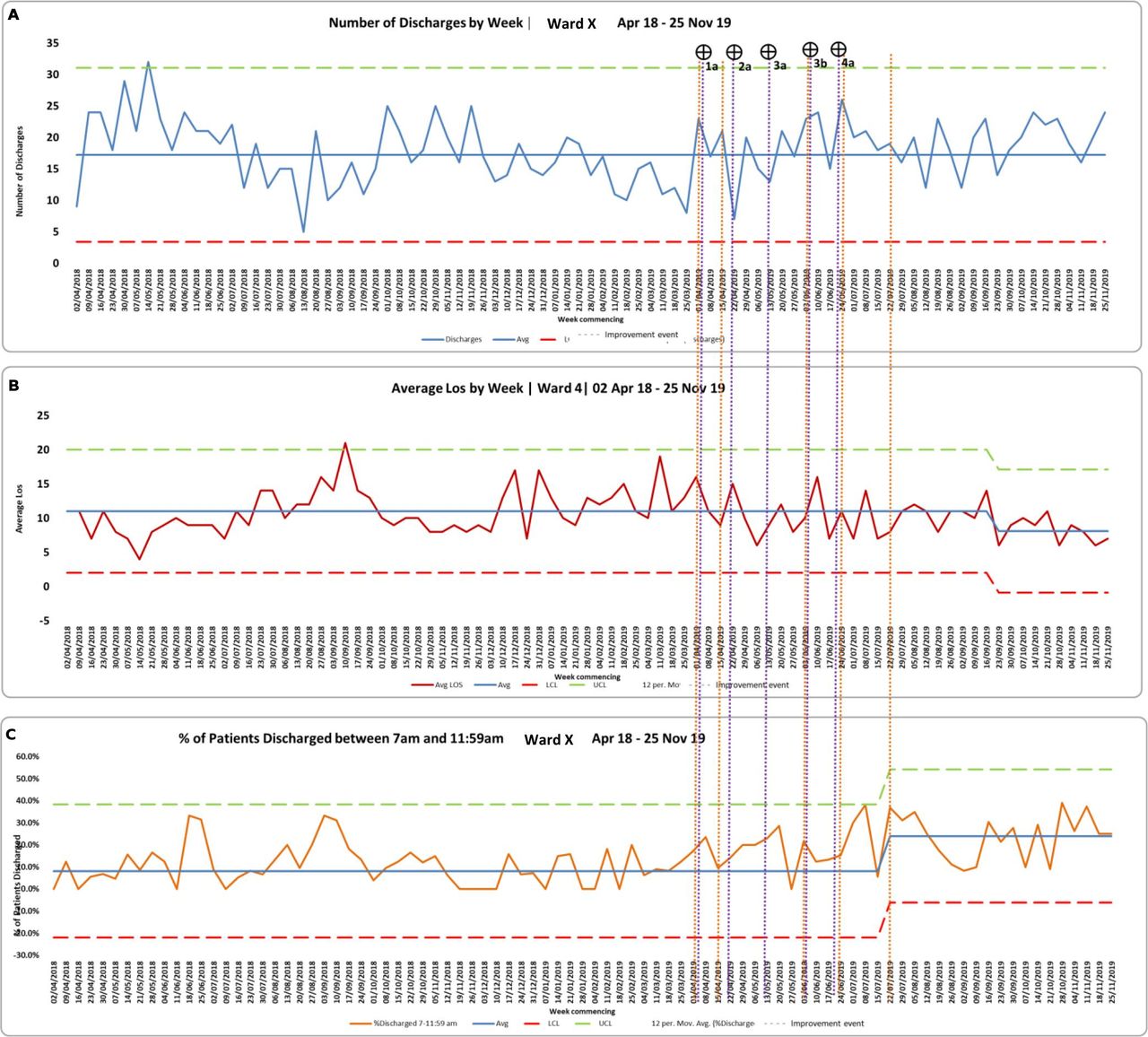
It was possible to see a significant change in the percentage prenoon discharges (figure 2C), but this was not seen until several months after the RIE, following the implementation of a number of PDSAs on Ward X (see table 1). It was initially agreed by the ward that collection of data around planned versus actual discharges would be helpful to monitor performance around discharge planning (PDSA 1a, ward X). Yet, following the RIE, the ward team did not find this data collection useful in practice and opted to abandon these interventions. Therefore, this process measure was not collected. The subsequent PDSA focused on a regular ward meeting to discuss patients and general improvements to improve team communication and cohesion once a week (figure 2)

Ward X statistical process control outlining. (A) Number of discharges. (B) Average LoS. (C) Percentage prenoon discharge of total discharges from 18 April to November 2019. Orange line indicates improvement workshops; purple line indicates plan–do–study–act cycles. LOS, length of stay. LCL, Lower Control Limit; UCL, Upper Control Limit
A key intervention implemented focused on ensuring appropriate discharge documentation was completed by the medical team, which began with setting an estimated date of discharge and then progressed to clearly documenting when the patient was ‘medically stable to be discharged or transferred’. Finally, a case patient was reviewed who had a long length of stay (114 days) in which a full root cause analysis was completed, including identifying the days in which the hospital was the only place care could have been provided for this patient. This analysis highlighted various areas for improvement and led to the instatement of weekly long length of stay reviews on the ward. From the data, it is not possible to see which intervention had the greatest impact, but it is likely there was a cumulative effect. Nonetheless, following PDSA 4a, we saw an improvement in the prenoon discharge measure from baseline of 8% to 24%.
Average LoS on Ward X did not change during the QIP from its baseline average of 11 days (figure 2B). However, several months after the final improvement workshop (90-day review) there was a gradual decrease of the LoS, which showed a significant change from baseline figures to 8.10 days. There was no change in 30-day readmission rates based on the data available.
Ward Y
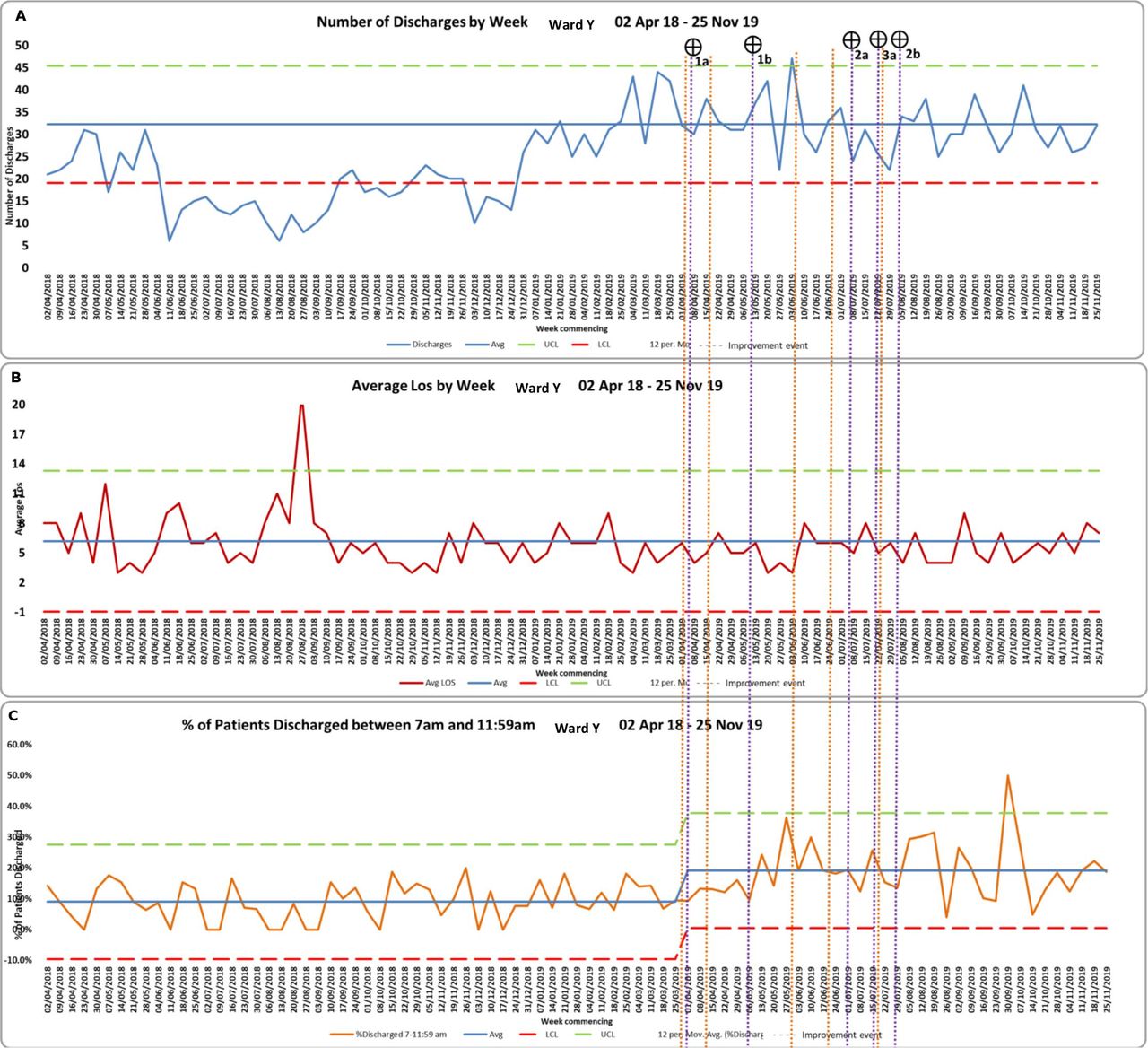
Ward Y saw an almost immediate change in percentage prenoon discharge figures from baseline average of 9%–19% (figure 3B), following the RIE and first PDSA implemented (see table 1). PDSA 1a focused on collecting data around planned versus actual discharges on Ward Y. Contrary to Ward X, this intervention continued following the RIE. Unfortunately, initial data collection was not captured electronically, but subsequent data were collected electronically through PDSA 1b; however, it was difficult to determine if there had been a significant change due to the lack of complete data set. There were several months between the first and second PDSA chains. PDSA 2a focused on reducing the referral time to community hospitals for orthopaedic patients. As follow-up to this PDSA, a patient leaflet was developed to update patients on their expected journey from acute care hospital into community hospital. Finally, PDSA 3a focused on improving the communication with staff, with the redevelopment of a clear ward communication board codesigned with staff expected to use the information. Despite these additional interventions, there were no further significant changes for the outcome measure. No changes were identified for 30-day readmissions (figure 3).

{kind=link}
{kind=link}
{kind=link}
Ward Y statistical process control outlining outlining. (A) Number of discharges; (B) Average LoS. (C) Percentage prenoon discharge of total discharges from 18 April to November 2019. Orange line indicates improvement workshops; purple line indicates plan–do–study–act cycles. LoS, length of stay. LCL, Lower Control Limit; UCL, Upper Control Limit
Lessons and limitations
The findings from the discharge QIP suggest strengths and challenges with the interventions implemented, as well as the engagement and application of the Lean-based improvement approach used in context. From the data it was possible to see differing levels of improvement at different times. This learning will be explored and guided using Pettigrew and Whipp’s context–content–process change model32:
Context
Organisational support
At the macro level, the discharge QIP was the first of a series of QIPs which would be taking place across the trust to improve the value stream for frail patients admitted to the hospital. With this, there was significant pressure especially on this QIP to deliver improvements, with it being the first time this improvement practice process was used. This facilitated significant buy-in from trust executives and senior management with attendance both in and outside of workshops. Commitment of executive staff has been found to be pivotal to success not just with Lean but other similar improvement approaches.33
Content
Development of apposite aim
In hindsight, using prenoon discharge as a proxy aim for ‘discharge’ more widely was too narrow in scope. This SMART aim was developed iteratively over the improvement practice process. Yet, despite this acting as a useful barometer of improvement, this outcome measure only loosely reflects the complexity of discharge. This highlights the importance of confirming the scope and SMART aim early in the QIP, ensuring that staff involved have an understanding of what it is trying to achieve.
Limited qualitative measures
There were little qualitative data collected as part of the improvement practice process for the discharge QIP. Tangible benefits such as better team cohesion, communication and knowledge of processes were reported during feedback, but this impact is not possible to capture using quantitative measures. Poor qualitative data collection is a common shortcoming among projects using lean and is an opportunity for improvement for future projects to gain a deeper understanding of the key stakeholders experience of the approach, resulting qualitative changes as well as patient experience.20 34
Engaging service users
A real strength of this QIP was the involvement of patients in the workshops and testing of interventions. None of the patients involved were deemed frail, but this PPI was fundamental, bringing a different perspective on what is ‘valuable’ for patients, challenging conventional staff views and supporting identification of waste.35–38
Process
Varying ward contexts
At the micro level, the two wards implemented differing interventions at different times. This was encouraged due to the different contexts of the wards and the differing levels of engagement of ward staff. From the data, ward Y clearly benefitted from implementing data collection related to planned versus actual discharges, which Ward X chose not to embed initially but chose later to develop a similar approach through implementing an ‘estimated discharge date’.
Both wards had varying degrees of staff engagement for the discharge QIP, with Ward X having two medical consultants engaged in the workshops and Ward Y not having the same level of medical staff buy-in. This may have been due to the differences between the wards in terms of specialty and type of patients that would be cared for, with Ward X being a medical ward for complex, often frail patients and Ward Y being a surgical ward providing care for frail patients but largely those who had fallen and sustained fractured. These varying levels of medical buy-in contributed to more expedited changes for Ward Y, where nursing staff in attendance had more control of the discharge process and were able to make the changes during the RIE. Ward X took longer to get consensus on appropriate intervention, but once agreed, this led to a greater level of improvement on prenoon discharges.
When reviewing other QIPs in the literature which focus on improving discharge of patients, lots of similar interventions are seen. However, a key output of such improvement activity is it facilitates shared decision making and distributed leadership between the staff, supporting improved team cohesion and overall team working, which likely supported the sustainability of changes rather than ‘dragging and dropping’ known solutions from different contexts.39 40
Format of improvement
Although staff were released to attend improvement workshops, little time was prioritised by staff when returning to operational duties to complete implementation work which led to slow progress with implementing interventions. It has been identified that quality improvement ‘will not realise its full potential unless change making becomes an intrinsic part of everyone’s job, every day, in all parts of the system’.41 The reliance on periodic externally organised workshops creates a risk in that improvement is seen as attending the ‘workshops’ rather than translation of changes into day-to-day practice. This is a common barrier to implementing Lean and embedding of continuous improvement more widely.33 42 43
Limitations
The original aim of achieving 33% was not achieved for either ward despite there being improvement seen in prenoon discharge measures. In addition, despite focussing on ‘discharge of patients’, this QIP centred only on what improvements can be made internally in the trust. There are lots of reasons for delay which exist between organisations rather than just internal inefficiency and therefore is a shortcoming on the QIP due to its limited scope.
The Lean-based improvement approach used a number of improvement approaches including Lean and, for this reason, did not have high fidelity to any one approach. There are few robust guidelines on how to apply Lean in healthcare, and because of this, there is variability in how such continuous improvement is implemented.20 31 44 Yet, the Lean-based improvement approach used during this QIP was adapted to suit the specific context to ensure that improvement was achievable, which is likely to be the case for whatever setting such an approach is used in. Therefore, this poses the challenge of how to balance both fidelity of implementation and local context and adaptation.
It is difficult to comment on the sustainability of the improvements made as well as the ability to use the improvement practice process more broadly in other contexts due to the limited scope of this evaluation and the relatively short nature of improvement so far. As discussed, the sustainability of the improvements will depend on the factors discussed previously, especially the engagement and ownership by frontline staff and managers, in addition to organisational support. What was encouraging was that improvements in prenoon discharge made had sustained several months after the initial step change.
The purpose of the approach was to create a continuous improvement culture not just one off ‘projects’. Although the improvements seen during this QIP were sustained, there was little focus developing the systems and routines which would continuously identify problems and drive improvement on a day-to-day basis on the wards. This therefore limited a cultural shift around continuous improvement, but this proof-of-concept was a step in the right direction for the organisation. An early positive indicator was that the trust embedded the use of the Lean-based improvement approach within their strategic goals for achieving its overall vision and values. Despite the relative infancy, such indications signal the strong sustainability of such an approach.45 46
Conclusion
This marked the first use of the Lean-based improvement approach at the trust. With this, some improvements in discharge metrics were identified in the clinical areas involved. It was also possible to see that the improvements seen during the QIP were sustained to varying degrees after the final workshop, with additional improvement in key metrics being seen after this. The limited scope of the QIP makes it difficult to confirm whether the improvement practice process used and the discharge interventions developed could be applied to other contexts and would therefore need further evaluation to confirm effectiveness. Nonetheless, at the time, this Lean-based improvement approach was being used in multiple other trusts in England to varying degrees, suggesting some repeatability and confirmation of approach.47
Little attention was focused on the qualitative evaluation of the staff as part of the Lean-based improvement approach. The literature suggests that use of Lean tools is an unsustainable way to make improvements and that culture change should be the focus of implementation, which is not something which can be accurately measured using quantitative measures.20 31 44 Further work should be completed to understand the impact the discharge QIP had on the participants as well as what the key principles are that facilitate a successful improvement project. In addition, further work should be focused on identifying how improvement can be translated into day-to-day practice rather than relying on timely and costly improvement workshops.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was sought locally from the host organisation, but this work was deemed a service evaluation and as such did not require full ethics approval.
Acknowledgments
This article was developed as a result of the author’s master of science dissertation at University of Nottingham, which was funded by the West Midlands Patient Safety Collaborative. Dedicated time was given by the authors' employer to conduct this evaluation; however, no funding was directly given to support this evaluation.
References
Footnotes
Twitter @TomJRollinson, @AklakC
Contributors TJR was the guarantor and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. He led the planning of the project, data collection, analysis, as well as development of the report, which is being used for the publication. JF supported with concept development and report writing, as well as proofreading and academic insight for the final publication submitted. SG was an academic supervisor supporting with planning, data collection, analysis and report development, as well as proofreading and academic insight for the final publication submitted. AC provided support through coaching on completion of the initial project, report writing, overall structure for the report and proofreading for the final publication submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Design section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.