Article Text

Abstract
A perioperative patient blood management (PBM) educational intervention was implemented for first year postgraduate doctors (interns) at the Royal Brisbane and Women’s Hospital (RBWH) following identification of a perioperative PBM training requirement. This quality improvement activity evaluated the effectiveness of this educational intervention in improving intern knowledge of perioperative PBM principles.
A 15-question perioperative PBM focused multiple choice questionnaire developed from information attained from comprehensive, evidence and consensus-based guidelines regarding PBM practice was distributed to interns immediately before a compulsory perioperative PBM educational intervention and then again 5 weeks later. The perioperative PBM educational intervention was delivered every 10 weeks (five interventions in total) to a different group of interns each time. Statistical analysis determined significance between mean questionnaire score before and after the intervention.
The mean pre-intervention score for correctly answered questions was 7/15 (SD 2.73) and mean post-intervention score was 9/15 (SD 2.99) (p=0.02). Categorisation of questions into core domains of perioperative PBM demonstrated intern scores for correctly answered questions improved in all domains following the educational intervention.
Perioperative PBM education delivered through a dedicated intervention aimed to improve knowledge is associated with objective evidence of educational benefits for interns at RBWH. It is an effective strategy to enact PBM governance and bestow clinical guideline knowledge. This is important given the global health sector’s challenge to improve patient outcomes despite increasingly restricted funding and pressure on doctors to devote more time to service and less to teaching.
- medical education
- anaesthesia
- quality improvement
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Transfusion of blood and blood products affords lifesaving therapy. However, the practice is costly, blood is scarce and accumulating evidence has identified a strong association between blood transfusion and patient morbidity and mortality.1–4 Re-evaluation has prompted a shift in the paradigm of transfusion medicine from conventional product-focused to patient-focused transfusion medicine referred to as patient blood management (PBM).3 5 PBM is the timely application of evidence-based medical and surgical concepts to optimise patient care through management of a patients’ own blood by means of safe and judicious use of blood products and assessment and development of pre-emptive management plans.6 PBM is most effective when implementation encompasses multiple interventions designed to address the three principles, commonly referred to as the three pillars, of PBM.7 These pillars are; (1) optimise patient red blood cell mass and coagulation status, (2) minimise perioperative blood loss and (3) enhance patient tolerance of anaemia.6
In Australia the National Blood Authority (NBA) and National Safety and Quality Health Service (NSQHS) provides comprehensive, evidence and consensus-based guidance regarding PBM practice and governance.6 8 Despite strong evidence and clinical guidelines, a knowledge deficit of basic perioperative PBM principles among first year postgraduate doctors (interns) at the Royal Brisbane and Women’s Hospital (RBWH) was recognised. This finding expedited an urgent need for a perioperative PBM educational intervention. The aim of this quality improvement (QI) activity was to evaluate the effectiveness of the perioperative PBM educational intervention, developed by staff of the Department of Anaesthesia and Perioperative Medicine at RBWH, in improving intern knowledge of perioperative PBM principles.
Background
Blood transfusion medicine is a component of Australian medical schools’ curriculum. However, there is no national, standardised curriculum in transfusion medicine for medical students or interns.7 9 The content and format of transfusion medicine teaching varies greatly between medical schools and hospitals, and so too does transfusion medicine knowledge among interns.7 9 Consequently, interns must learn principles of transfusion medicine as they concurrently care for patients with blood product needs. This can lead to inappropriate utilisation of blood products, increasing the risk of adverse events to patients. This deficit in transfusion medicine education and intern knowledge is not endemic to Australia. Globally, there is a need for healthcare institutions to develop PBM education programmes.9–11
Medical education interventions are common methods to introduce new topics or review difficult topics for interns. A multitude of interventions employed in the postgraduate medical setting, ranging from lectures to simulation sessions, have been successful in improving knowledge retention.12 However, there is paucity of high-level research evaluating the effectiveness of strategies to enhance knowledge of perioperative PBM principles among interns. Furthermore, validated questionnaires evaluating knowledge of transfusion medicine exist, however as far as we know there is no validated tool to assess the broad spectrum of PBM-specific content.13 Provision of knowledge and skills through continuous professional development tutorials is an important strategic instrument to enhance medical competence as well as recruit, motivate and retain high-quality staff.
Clinical leaders and senior managers at RBWH, determined to promote best practice in relation to prescription, management and administration of blood and blood products in accordance with current evidence-based standards, developed a perioperative PBM educational intervention designed to enhance intern knowledge of perioperative PBM principles. To our knowledge, this study is the first in Australia to evaluate change in intern perioperative PBM knowledge using pre-intervention and post-intervention questionnaire scores.
Measurement
We determined change in intern perioperative PBM knowledge by comparing pre-intervention and post-intervention questionnaire scores. The questionnaire was composed of 15 multiple choice questions (see online supplemental materials 1 and 2) formulated by members of the perioperative PBM group at RBWH using information attained from NBA’s PBM guidelines and NSQHS Chapter 7: Blood and blood products. The questionnaire was reviewed by staff of the RBWH Anaesthesia and Perioperative Medicine Department who were not involved in development of the questionnaire to identify ambiguous or misleading questions and eliminate unnecessary questions as well as ensure the questionnaire was of reasonable length. The questionnaire was modified based on this feedback before being administered to the study population.
Supplemental material
Supplemental material
Design
This QI activity was undertaken at the RBWH in Brisbane, Australia between February 2018 and December 2018. RBWH is a tertiary level hospital and part of the Metro North Hospital and Health Service in Queensland, Australia. It is the largest teaching and research hospital in Queensland. RBWH recruits the largest number of interns in the state from a number of different universities, making it an ideal cohort to attain a study population.
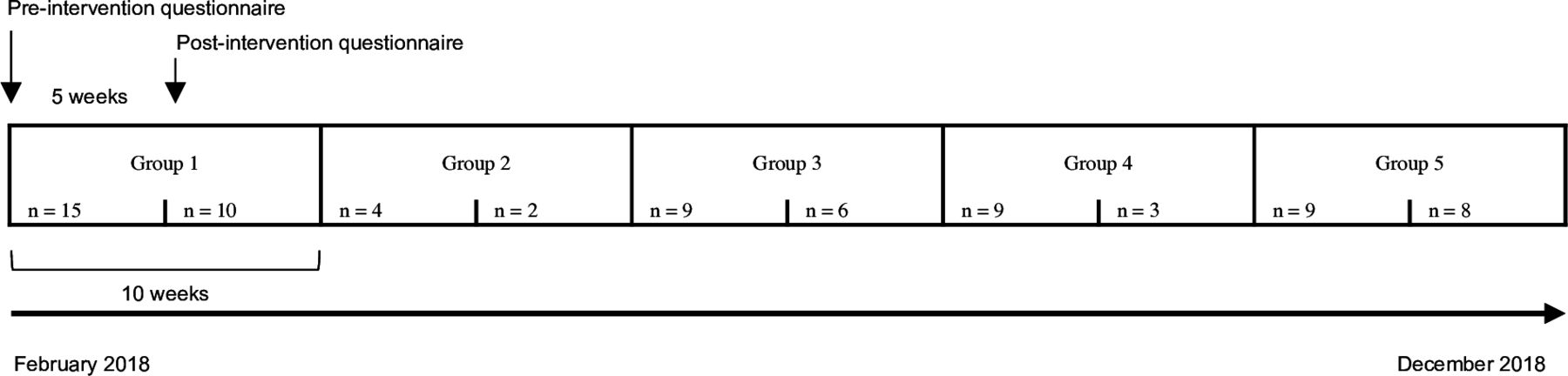
The educational intervention was collaboratively delivered, in 50 min, by a preoperative anaemia Clinical Nurse Consultant, blood transfusion Clinical Nurse Consultant, Haematology Physician and Anaesthetist. The intervention was delivered every 10 weeks (five interventions in total) to a different group of interns within a dedicated education room at the hospital (figure 1). The same staff members facilitated each educational intervention. The intervention included education on the following topics; PBM definition and the importance of PBM to patient care, NBA perioperative module, the three pillars of PBM management and how the pillars can be applied to a surgical patient, perioperative anaemia identification and management, the morbidity and mortality associated with preoperative anaemia and red blood cell (RBC) transfusion, interpretation of blood pathology results, prescription and management of iron infusions, safe blood transfusion practice including correct prescribing and local hospital policies relating to blood management. Multiple iron deficiency and anaemia case studies and a single case study detailing a surgical patients’ perioperative journey was also discussed within the educational intervention. Time was allowed for questions and open discussion. PowerPoint presentations and hard-copy handouts facilitated content delivery during these tutorials. Interns who attended the tutorial were also emailed soft copies of the presented material for their own review. RBWH staff from the Department of Medical Education used a QR code scanner with export to Excel to track intern attendance at each tutorial.
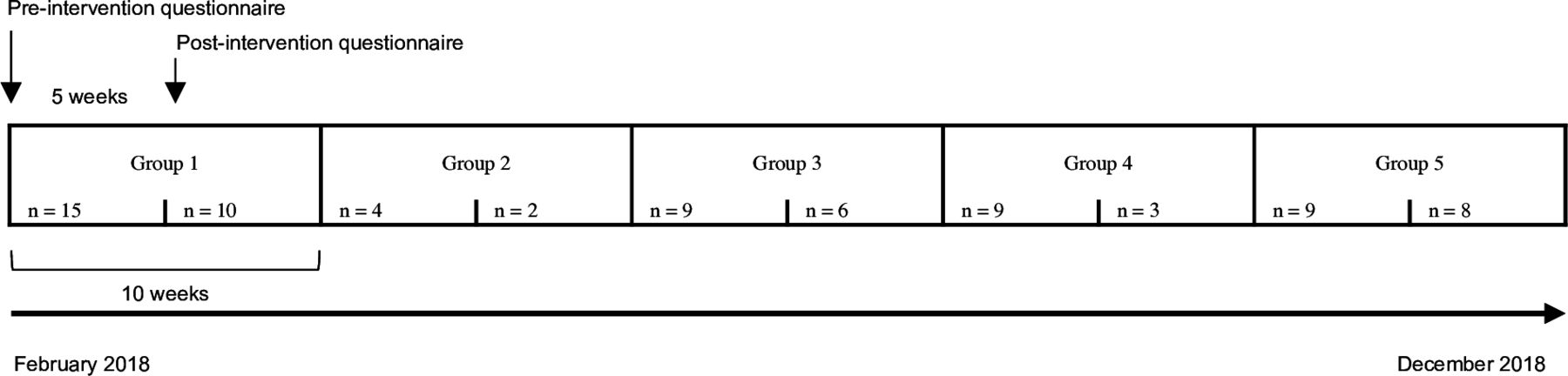
Timeline of quality improvement intervention depicting timing of pre-PBM educational intervention questionnaire and post-PBM educational intervention questionnaire as well as the number of participants who completed each questionnaire according to group and pre-intervention and post-intervention status.
Strategy
The questionnaire was distributed face-to-face in paper format to interns pre-intervention. The questionnaire was subsequently redistributed face-to-face 5 weeks later in paper format among the same interns for completion (figure 1). The data collected was anonymised after each test period which meant an individual’s score could not be tracked from pre-intervention to post-intervention. The data was entered into an Excel spread sheet and then analysed once all questionnaire responses recorded. Questionnaires were completed under supervision of PBM facilitators to ensure sharing of information or answers did not occur during completion of the questionnaire.
Results
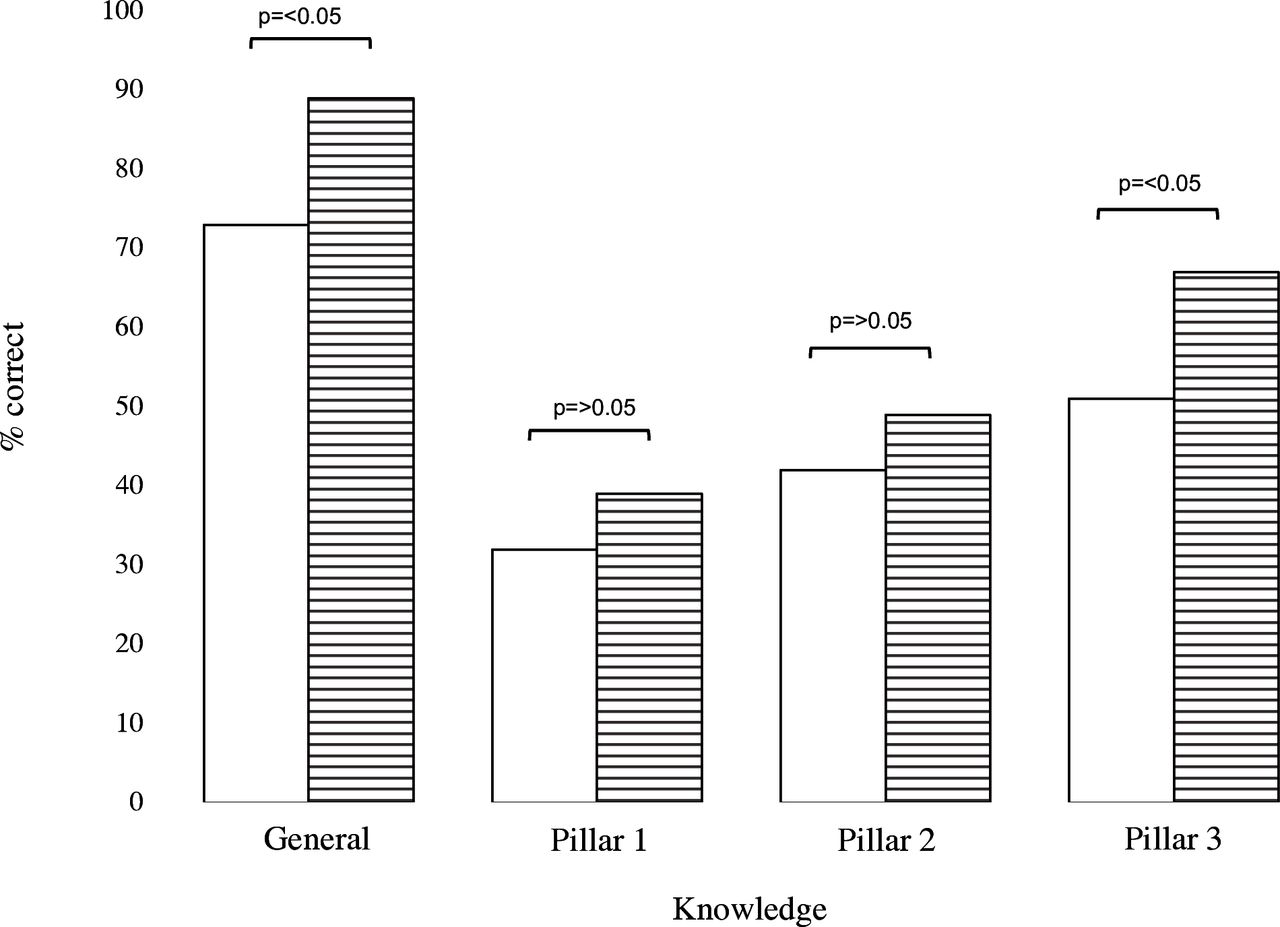
The results presented have been pooled across the five groups of interns as variance was assumed to be similar in each group. The number of questions answered correctly increased from 46.6% pre-intervention to 60% post-intervention (p=0.02). Paired t-test determined statistical significance which was set at a value of p<0.05. Figure 2 illustrates the percentage of correct answers to the 15 questions asked in the pre-intervention and post-intervention questionnaires categorised into general knowledge and the three pillars of PBM. Table 1 also demonstrates the percentage of correct answers within each domain, also with tests of significance comparing scores pre-intervention and post-intervention calculated as χ2. Statistical significance was set at a value of p<0.05. The intention of this type of statistical analysis was to identify domains where interns were stronger or had better knowledge retention. The domain with the highest score for correctly answered questions pre-intervention and post-intervention was general knowledge. We saw an increase in correctly answered questions in all domains; general knowledge (59%–71%, p=0.02), pillar 1 (32%–39%, p>0.05), pillar 2 (42%–49%, p>0.05) and pillar 3 (51%–67%, p=0.02).

{kind=link}
{kind=link}
Graphical representation of correctly answered pre-intervention (clear boxes, n=46) and post- intervention (lined boxes, n=29) questions (%) according to the following knowledge areas; general knowledge and the three pillars of patient blood management; (1) optimise patient red blood cell mass and coagulation status, (2) minimise perioperative blood loss and (3) enhance patient tolerance of anaemia. P values indicate significance between pre-intervention and post-intervention scores.
Demonstrates mean questionnaire score, from a total score of 15, both pre-intervention (n=46) and post-intervention (n=29) (SD) as well as the per cent of correctly answered questions pre-intervention and post-intervention categorised into knowledge domains. P values indicate significance between pre-intervention and post-intervention questionnaire scores
Lessons and limitations
A limitation of this study design was related to the sample size, which was largely dictated by the attendance rates to the educational intervention sessions which in turn represented varied questionnaire response rates per phase of the study. The interns were asked to complete the post-intervention questionnaire only if they answered affirmatively to have attended the initial educational intervention. However, we cannot confirm the same as we anonymised the interns after receiving pre-intervention questionnaire scores. Although a limitation, this is representative of the expected reality of the delivery of this type of intervention as not all individuals will necessarily be able to attend the sessions.
Knowledge changes in a control group who did not receive PBM education was not assessed. Differences in knowledge between interns who did and did not receive the educational intervention would provide insight into the knowledge of senior doctors’ transfusion practices who bestow knowledge on interns through cascade learning. Conversely, this knowledge attained though clinical experience and teaching is a confounding factor in the outcome of this QI activity.
Generalisability of findings is limited as intervention was undertaken at a single site. Although PBM has been implemented nationally in Australia, delivery of PBM education across the eight different state-based or territory-based healthcare systems in Australia not only varies between the states and territories but also hospital to hospital.9 14–16 It is important that an effective educational intervention and validated questionnaire is developed to ensure doctors receive adequate education and training to support safe and appropriate PBM regardless of their hospital location or role within the hospital. Future studies should focus on validation of one unique multiple-choice questionnaire based on expert opinion applying questionnaire design methodology.
Conclusion
In recognition of transfusion-associated patient morbidity and mortality and decreasing availability of donor blood many hospitals have developed and promulgated blood transfusion programmes and guidelines to support clinicians to provide optimal PBM therapies.9 14–16 Recognition of the effectiveness of a perioperative PBM educational intervention delivered through expert-led, relevant and timely teaching to interns to enact PBM governance and bestow clinical guideline knowledge is important. The impact of a successful intervention improves the quality and safety of patient care and attributes social, economic and environmental value to the healthcare system.
In a single-hospital-wide intervention to implement more restrictive RBC transfusion practices, hospital mortality and length of stay reduced, with millions of dollars in cost savings.17 These findings correlate with a systematic review and meta‐analysis of randomised control trials which demonstrated that trials with more restrictive transfusion thresholds significantly reduced cardiac events, infection, rebleeding and mortality compared with trials that used less restrictive transfusion thresholds.18 Improved PBM knowledge reduces blood transfusions.19 Reduction in blood transfusions will have an advantageous environmental impact by reducing energy consumption required for product development.
The impact of transfusion medicine and PBM strategies to enhance doctor knowledge has previously been investigated. Kotzé and colleagues demonstrated PBM educational intervention improved anaemia management of surgical patients through reductions in preoperative anaemia, blood loss and blood transfusion.19 Medical students confidence and transfusion medicine test scores were significantly greater following an educational intervention which used an engaging and visually stimulating presentation to display high-impact transfusion medicine material, than other students who did not receive the presentation.20 Similarly, medical students’ transfusion medicine test scores improved significantly following a simulation-based education activity designed to teach transfusion medicine.21 The results of this QI activity indicate a dedicated perioperative PBM educational intervention is an important strategic instrument to enhance medical competence among interns and the questionnaire applied is appropriate to assess change in level of knowledge. This is significant considering the global health sectors challenge to improve patient outcomes with increasingly restricted funding and pressure on doctors to devote more time to service and less to dedicated teaching. Healthcare providers should support and strengthen further activities in PBM. We will recommend to hospital administration the ongoing delivery of our education programme to interns and yearly evaluation thereof. Future direction will focus on ensuring this attained knowledge is applied to practice.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical exemption was granted from the Royal Brisbane and Women’s Hospital ethics committee (HREC/18/QRB3/114). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank Eva Malacova for her help in providing statistical analysis of the data.
References
Supplementary materials
Footnotes
Contributors KW designed the study. KW, KT and SC-B contributed equally to the formation of questionnaires. KT and SC-B undertook distribution and follow-up of the multiple choice questionnaire. KT performed statistical analysis with the help of statistician. KT, KW and SC-B drafted and reviewed the paper. KW is the guarantor of this QI project.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.