Article Text

Abstract
Background Sleep disordered breathing represents a spectrum of upper airway obstruction including snoring, increased respiratory effort and obstructive sleep apnoea. An increasing demand for paediatric preoperative sleep studies and postoperative high dependency unit (HDU) beds was having a significant impact on service delivery at this ear, nose and throat (ENT) unit.
Methods Retrospective and prospective review of all paediatric sleep study requests over a 30-month period in a single tertiary ENT department. Data were collected on indication for and result of sleep study, patient outcome, operative details and HDU bed occupancy. During the study period, a ‘Sleep Study’ proforma was introduced which incorporated the ‘I’m Sleepy Score’ (ISS) and ENT-UK national guidelines.
Results Retrospective review included 198 sleep studies, of which 62% (n=118) showed no evidence of obstructive sleep apnoea (OSA). There was little consistency in patients’ sleep study results and need for monitoring on HDU following adenotonsillectomy. Prospective review following intervention included 60 patients, of which 62% (n=37) showed evidence of OSA. The mean ISS in this cohort was 4.7. Only those with moderate-to-severe OSA or with relevant risk factors underwent overnight HDU observation. The number of sleep study requests fell by >50%; from 11 per month to 5 per month. The total HDU bed occupancy was reduced by 50% following intervention (from n=18 to n=9).
Conclusion The use of the ISS and incorporation of ENTUK’s recommendations has reduced the number of negative sleep studies being requested and has rationalised the number of paediatric HDU bed requests being made. This has helped provide a prudent elective paediatric ENT service in this unit with corresponding cost benefits.
- diagnosis
- paediatrics
- Quality improvement methodologies
Data availability statement
Data are available on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Background
Sleep disordered breathing (SDB) represents a spectrum of upper airway obstruction including snoring, increased respiratory effort and obstructive sleep apnoea (OSA).1 SDB affects 1%–4% of the general paediatric population and may have significant effects on both the child’s short-term daytime behaviour and long-term health.2 As a result, paediatric SDB requires prompt diagnosis, investigation and treatment by ear, nose and throat (ENT) surgeons. Although the causes of paediatric SDB are multiple, the most common cause is adenotonsillar hypertrophy which can be managed with adenotonsillectomy.3
The gold-standard investigation for diagnosis of OSA is overnight in-laboratory polysomnography. Alternatively, parents can be provided with a ‘sleep study’ kit to complete the investigation at home.4 Other researchers have developed a variety of scoring checklists which help identify whether children are at risk of OSA; for example, the I’m Sleepy Score (ISS) is a validated 8-point scoring tool which is completed by parents and is highly sensitive for paediatric OSA.5 It is applied in the same way that the Epworth Sleepiness Scale is used in adults with suspected OSA.6
Paediatric ENT surgery is one of the most common elective services in the National Health Service (NHS). Recent changes in hospital regulations based on the 2009 consensus statement for the delivery of elective paediatric ENT surgery may have resulted in many children being transferred to tertiary centres with paediatric intensive care units in order to undergo postoperative monitoring for elective ENT surgery.7 8 This has been supported by findings in the Getting It Right First Time national programme.9
This led to ENTUK’s National Strategy for the Safe Delivery of Paediatric ENT Surgery in the UK.10 This strategy has outlined recommendations about which paediatric patients can be appropriately managed in both secondary and tertiary units when undergoing elective ENT surgery.
Problem
There were growing concerns for the demand in paediatric pre-operative sleep studies at this tertiary unit, some of which appeared to be requested without rationale. In addition, the number of postoperative high-dependency unit (HDU) beds being booked for patients undergoing elective adenotonsillectomy was having a significant impact on patient waiting times and cancellations due to bed shortages. HDU bed bookings should be made for those patients whose sleep study had shown moderate-to-severe OSA or for other coexistent morbidities; however, HDU beds are occasionally booked at the discretion of the individual ENT clinician. Our elective paediatric surgical unit has a capacity for 16 patients with 4 HDU beds available in addition, however, these require additional nursing staffing to operate.
This study’s aim was to determine if implementation of risk-stratification tool for performing preoperative sleep studies and introduction of a local guideline based on the ENTUK National Strategy guidance could provide a safe, prudent approach to requesting sleep studies and postoperative HDU beds in this paediatric ENT department.
Methods
Study design
There were three cycles in this quality improvement project. Retrospective review, intervention design and prospective review of all paediatric patients undergoing preoperative sleep study at a single tertiary ENT unit over a 30-month period was performed. The Standards for QUality Improvement Reporting Excellence (SQUIRE) 2.0 guidelines have been adhered to in the planning and reporting of this quality improvement project.11
Definitions
For the purposes of analyses, sleep study results were classified and analysed according to the Apnoea Hypopnea Index (AHI) as follows12 :
AHI<1: no OSA.
AHI≥1 to<5: mild OSA.
AHI≥5 to<10: moderate OSA
AHI≥10: severe OSA.
Exclusion criteria
Paediatric patients who had sleep studies requested by other specialties, patients who did not complete their care within the NHS and patients who did not complete sleep study.
Analysis
Data were anonymised and input into Microsoft Excel. Data are presented as number (n) or percentage (%) unless otherwise stated, to allow comparison between preintervention and postintervention data, as well as with international literature.
Patient and public involvement
Patients were not involved in the formation or reporting of this project.
Strategy
Baseline retrospective review
Retrospective review of all paediatric patients who had a sleep study requested by an ENT clinician in a single ENT department between June 2016 and December 2017 (18-month period). Data were collected on: patient demographics, indication and result of sleep study ((AHI, number of apnoeic events, minimum and mean oxygen saturations, pulse rise index and number of events, mean pulse±SD), patient outcome and subsequent operative details (indication for surgery, operation note, length of stay and place of recovery). These data were then compared with the standards set by the ENT-UK national strategy to determine the compliance with current best practice guidelines and allow areas for improvement to be identified to streamline the elective paediatric ENT service delivery; considering both the patient and system-centred benefits.10
Intervention design process
Following this baseline review, intervention in the form of a ‘Sleep Study Request Proforma’ was designed in conjunction with both ENT, paediatric and anaesthetic staff. The aim was to create an evidence-based pathway in order to assist the clinician’s decision to request a sleep study and if applicable, postoperative paediatric HDU bed. This was initially created by a working party of a consultant paediatric ENT surgeon with a special interest in sleep disorders, a consultant paediatric anaesthetist, a paediatric ENT nurse specialist who coordinates elective paediatric ENT surgery, junior ENT trainees with an interest in paediatric ENT and paediatric ward nursing staff. The latest relevant published evidence was considered and placed in the context of the local problem to create a thorough proforma; intending to capture the child’s likelihood of OSA, need for further investigation via sleep study and subsequent need for HDU bed postoperatively. Multidisciplinary input from the wider ENT consultant body was then sought in this process and the proforma was modified until a consensus was achieved. This was performed by presenting iterations of the proposed proforma until the most user-friendly, efficient and evidence-based version was agreed by all staff.
The final version of the request proforma utilised the evidence-based ISS (where a score of ≥3 out of 8 indicates a high likelihood that child is at risk of OSA, as determine by the original authors of the ISS).5 The domains include frequent snoring, daytime somnolence, apnoeic episodes, enlarged tonsils and raised body mass index.5 A patient with a score of ≥3 or one relevant risk factor (box 1) was subsequently referred to the paediatric nurse specialist for completion of the sleep study. The criteria for booking a postoperative paediatric HDU bed were based on the Safe Delivery of Paediatric ENT Surgery in The UK National Strategy 2019, where a postoperative HDU bed was indicated if AHI was ≥5 (moderate-to-severe OSA), oxygen saturations nadir ≤85% during sleep study or relevant comorbidity.10
Relevant risk factors for elective paediatric ENT surgery10
Age <3 years.
Weight <15 kg.
Body mass index >99th centile for age/gender
Down’s syndrome.
Cerebral palsy.
Neuromuscular disorders (eg, hypotonia, muscular dystrophy).
Craniofacial anomalies or difficult airway.
Polysaccharidosis.
Significant comorbidity (eg, complex or uncorrected congenital heart disease, home oxygen requirement, severe cystic fibrosis).
ENT, ear, nose and throat.
Prospective review
Once agreed, the proforma was implemented from January 2019. All relevant ENT clinicians were made aware of the new proforma process at a monthly departmental meeting. To support compliance, the proforma was readily available for clinicians when seeing paediatric patients in clinic. In addition, the lead paediatric ENT nurse specialist enhanced compliance by ensuring that the proforma was completed for all children requiring a sleep study or being considered for elective ENT surgery where a HDU bed may be required, prior to review in the pre-operative assessment clinic.
The aims of this stage were to determine the compliance with the sleep study proforma and thus compliance with ENTUK national guidelines.9 As a result, the aim of this were to assess the positive implications on the elective paediatric ENT service. Data were collected prospectively for 12 months from January 2019 to December 2019 (12 months). Each proforma was collected by the paediatric ENT nurse specialist after completion. After each child had undergone surgery, the authors undertook prospective review of the sleep study requests, collecting identical data points to the retrospective review as above, as well as the child’s ISS. This also allowed an assessment of the number of HDU beds required on weekly basis, comparing the preintervention and postintervention periods.
The intervention has maintained longevity and the changes have been preserved to date. It now forms a core aspect of the ENT nurse-led preassessment clinic workload, where sleep study result and subsequent need for post-operative HDU bed can be considered and booked if necessary.
Results
Retrospective review
A total of 198 sleep studies were requested during the 18-month study period and 191 sleep studies were completed. This represents 11 sleep study requests per month. Mean age of patients was 5.02 years (range: 2–17 years).
The indications for the sleep study request were: 60.7% (n=116) for SDB, 23.0% (n=44) for SDB with recurrent tonsillitis, 3.7% (n=7) SDB post-tonsillectomy, 3.7% (n=7) for recurrent tonsillitis alone, 2.1% (n=4) for large tonsils and 6.8% (n=13) for other indications including laryngomalacia, otitis media with effusion, nasal obstruction and asymmetrical tonsils.
Of the 191 sleep studies completed, 61.8% (n=118) showed no evidence OSA and 38.2% (n=73) showed evidence of OSA. Based on classification of sleep study by AHI, as explained above:
61.8% (n=118) showed no evidence of OSA. Of these, 1 patient had adenotonsillectomy with overnight stay on HDU with monitoring (with an unclear indication), 38 had tonsillectomy with postoperative recovery on ward. Eighty-three patients were discharged from clinic with no intervention or ‘watchful waiting’. Watchful waiting may include observation without intervention or keeping patients on a ‘see-on-symptom’ list for a specified period of time prior to discharge form clinic.
29.8% (n=57) had mild OSA. Five patients had adenotonsillectomy with overnight stay on HDU with monitoring, 20 had tonsillectomy with postoperative recovery on ward and 32 were discharged from clinic with no surgical intervention.
3.1% (n=6) had moderate OSA. Two patients had adenotonsillectomy with overnight stay on HDU with monitoring, one had tonsillectomy with postoperative recovery on ward and three were discharged from clinic (all with watchful waiting at request of parents).
5.3% (n=10) had severe OSA. Eight patients had adenotonsillectomy with overnight stay on HDU with monitoring, 1 was discharged from clinic and one was lost to follow-up.
In total, 18 children used HDU beds postoperatively in this study period, of which 37.5% (n=6) were unnecessary based on AHI. This equates to approximately one child per month requiring HDU following adenotonsillectomy.
Prospective review
Following implementation of the ISS proforma, data were collected prospectively for 12 months. Sixty sleep studies were requested in this period and 60 were completed. This represents five sleep study request per month. Average age was 5.45 years (range 2–16 years).
The clinical characteristics of the patients in the prospective cohort are compared with the retrospective cohort in table 1.
Clinical characteristics of patients in the two study groups
The indication for sleep study requests were 66.7% (n=40) SDB, 10.0% (n=6) SDB and recurrent tonsilitis, 8.3% (n=5) recurrent tonsilitis, 6.7% (n=4) SDB and otitis media with effusion, 6.7% (n=4) otitis media with effusion and 1.7% (n=1) combined SDB, recurrent tonsilitis and otitis media with effusion.
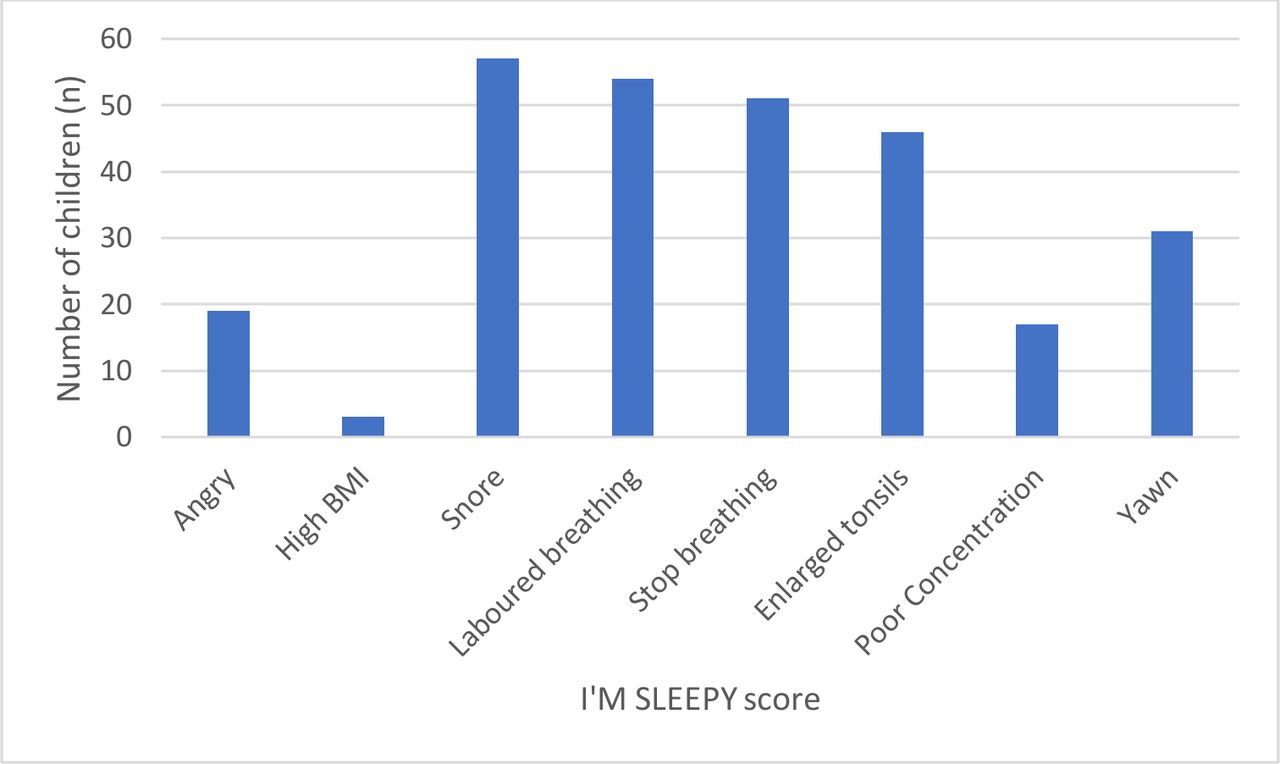
The mean ISS for this cohort was 4.6 (range 3–7 out of 8). Figure 1 shows the overall breakdown of the ISS for this cohort of paediatric patients preoperatively, with SD and range.

Breakdown of I’m Sleepy Score matrix for children undergoing sleep study preoperatively. BMI, body mass index.
Fourteen patients had a relevant risk factor: five children were aged less than 3 years, five weighed less than 15 kg and four had a relevant comorbidity as listed in box 1.
Of the 60 sleep studies completed, 38.3% (n=23) showed no evidence of OSA and 61.7% (n=37) showed evidence of OSA. Based on classification of the AHI:
38.3% (n=23) showed no evidence of OSA. Five were treated with adenotonsillectomy with recovery on ward, 13 were discharged from ENT follow-up and 5 were managed with watchful waiting. The mean ISS score for the non-OSA group was 4.2 (range 3–7).
30.0% (n=20) had mild OSA. Six were managed with adenotonsillectomy on the ward and 14 were discharged from ENT care.
16.7% (n=10) had moderate OSA. Five patients were treated with adenotonsillectomy with overnight observation on paediatric HDU and five were managed with watchful waiting at parental request.
8.3% (n=5) patients had severe OSA. Four were managed with adenotonsillectomy with overnight observation on HDU and one child was treated with watchful waiting at parental request.
The full sleep study trace was not available for two patients, however, the AHI and relevant results were summarised in ENT consultant clinical letters.
In total, nine children utilised HDU beds postoperatively in this study period, all which were necessary and evidence based. This equates to approximately one child every 2 months requiring HDU following adenotonsillectomy.
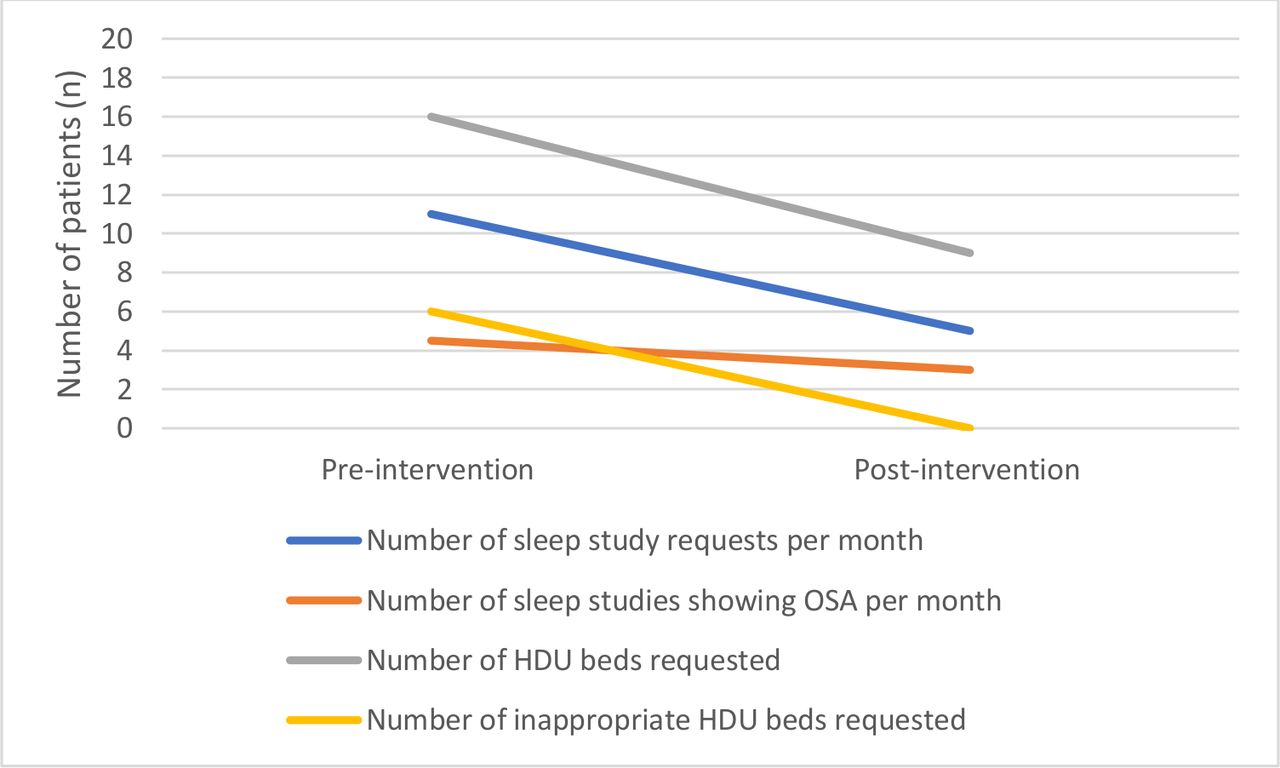
Figure 2 shows a line chart of the key measurements relating to number of sleep study requests and subsequent HDU bed requests when comparing preintervention and postintervention phases.

{kind=link}
{kind=link}
Line chart of key measures comparing preintervention and postintervention. HDU, high-dependency unit; OSA, obstructive sleep apnoe.
In this quality improvement project, the use of a paediatric OSA risk stratification score was associated with a reduction in preoperative sleep study requests. In addition, postoperative HDU bed requests were reduced by implementing ENTUK’s national recommendations for the safe delivery of paediatric ENT surgery.
Initial review identified that there was a high volume of sleep studies completed with normal results and a disparity between postoperative HDU bed requests. In addition, the demand for sleep studies and postoperative paediatric HDU beds was having an overwhelming effect on the ENT department. Completion of sleep studies was being significantly delayed for patients and a number of elective operations had to be cancelled due to scarcity of postoperative HDU beds and appropriate paediatric nursing staff to operate the elective surgical HDU.
The intervention, through the use of the ISS and incorporating the ENTUK’s recommendations, has reduced the number of sleep studies being requested by 50% and has rationalised the use of paediatric HDU beds for postoperative monitoring. In the retrospective review, there were on average 11 sleep study requests per month compared with 5 per month following intervention. This demonstrates the value that applying risk stratification scores, such as the ISS, and following national recommendations can have on all departments. Through a relatively simple intervention and adoption of an evidence-based approach, the burdens on our elective paediatric ENT service have been lessened, with positive implications for both staff and patients alike. In particular, the longevity of this intervention ensures adequate availability of beds for elective paediatric ENT surgery even during the pressures of the COVID-19 pandemic.
At initial review, 61.8% of the sleep studies completed showed no evidence of OSA. However, following the introduction of the ISS to risk stratify the requests, only 38.3% showed no evidence of OSA. Likewise, fewer unnecessary post-operative HDU beds were requested following intervention since only those were moderate-to severe OSA as identified on the sleep study were listed for postoperative HDU monitoring. This has improved the work-flow of the paediatric ENT elective service. The COVID-19 pandemic has highlighted the importance of HDU bed availability, and thus the value of risk stratification scores as demonstrated in this study may be wide-reaching to other units and specialties.13 This can be applied to both HDU bed occupancy for critically ill patients but also in the planning of elective surgical services.14
Interestingly in the prospective review, a higher ISS did not necessarily correspond with a higher AHI on sleep study (table 1). However, the authors believe that this is because the children in this cohort with severe OSA were more likely to be younger (<3 years) and have more relevant risk factors. The mean ISS score was higher in the patients with OSA when compared with those without OSA, however, the ISS score was less reliable at predicting mild, moderate and severe OSA based on the subsequent AHI.
The NHS National Cost Collection Guidance 2019 states that a paediatric HDU bed costs approximately £1339.00 per night (code: XB07Z).15 This study demonstrated a reduction of 18 paediatric HDU beds to 9 HDU beds following intervention, which is likely to represent a significant cost benefit.
Identification of paediatric OSA is key to preoperative assessment; particularly due to the high risks of the postoperative period and adverse effect of anaesthetic agents.16 This has led to numerous OSA screening tools being published in the literature including: ISS, Paediatric Sleep Questionnaire, Sleep Clinical Record, OSA-18 score (OSA-18), Brouilette score and ‘Sleeping Sleepless Sleepy Disturbed Rest’ questionnaire.17 18
The ISS is a validated, dichotomous 8-point scoring tool which is completed by clinician and parent in order to assess both the nocturnal and diurnal symptoms of SDB.5 In a comparative analysis, the ISS was found to be one of the more useful tools due to its simplicity, short time to complete, high sensitivity for paediatric OSA (>82%) and implications for further investigation.15 Anecdotally, the ISS was felt to be an appropriate, quick screening tool for OSA in our paediatric ENT clinic and hence this tool’s selection in our study.
Limitations
The data generated are reliant on patients’ electronic records which are presumed to be complete and correct. This quality improvement project has been beneficial for this single ENT department due to the local problems faced in service delivery; and thus, further multicentre research is needed to determine the generalisability of this work.
Conclusion
Management of OSA is a large part of the paediatric ENT surgeon’s workload. This study reports the beneficial intervention of a sleep study proforma which incorporates the ISS and ENTUK recommendations for elective paediatric ENT surgery. The tool has aided clinical decisions regarding the need for preoperative sleep study in paediatric patients with suspected OSA undergoing elective surgery and rationalised the use of paediatric HDU beds for postoperative monitoring in our institution. These changes have contributed to the provision of a prudent and safe paediatric ENT elective service which have been maintained to date.
Data availability statement
Data are available on request.
Ethics statements
Patient consent for publication
Ethics approval
The project was registered and approved by the health board’s audit and research department. Formal ethics committee approval was not considered necessary.
Acknowledgments
Gemma Hebben, staff in the anaesthetic, paediatric and ENT departments of Morriston Hospital Swansea.
References
Footnotes
Presented at Results were presented at British Academic Conference in Otolaryngology (BACO) International Virtual conference January 2021.
Contributors SM is lead data collector, lead author and guarantor. RJ and PMP were involved in data collection, drafting and coauthors. ME and HW were coauthors and project supervisors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.