Article Text

Abstract
Introduction Avoiding low value medical practices is an important focus in current healthcare utilisation. Despite advantages of point-of-care ultrasound (POCUS) over chest X-ray including improved workflow and timeliness of results, POCUS-guided central venous catheter (CVC) position confirmation has slow rate of adoption. This demonstrates a gap that is ripe for the development of an intervention.
Methods The intervention is a deimplementation programme called DRAUP (deimplementation of routine chest radiographs after adoption of ultrasound-guided insertion and confirmation of central venous catheter protocol) that will be created to address one unnecessary imaging modality in the acute care environment. We propose a three-phase approach to changing low-value practices. In phase 1, we will be guided by the Consolidated Framework for Implementation Research framework to explore barriers and facilitators of POCUS for CVC confirmation in a single centre, large tertiary, academic hospital via focus groups. The qualitative methods will inform the development and adaptation of strategies that address identified determinants of change. In phase 2, the multifaceted strategies will be conceptualised using Morgan’s framework for understanding and reducing medical overuse. In phase 3, we will locally implement these strategies and assess them using Proctor’s outcomes (adoption, deadoption, fidelity and penetration) in an observational study to demonstrate proof of concept, gaining valuable insights on the programme. Secondary outcomes will include POCUS-guided CVC confirmation efficacy measured by time and effectiveness measured by sensitivity and specificity of POCUS confirmation after CVC insertion.
With limited data available to inform interventions that use concurrent implementation and deimplementation strategies to substitute chest X-ray for POCUS using the DRAUP programme, we propose that this primary implementation and secondary effectiveness pilot study will provide novel data that will expand the knowledge of implementation approaches to replacing low value or unnecessary care in acute care environments.
Ethics and dissemination Approval of the study by the Human Research Protection Office has been obtained. This work will be disseminated by publication of peer-reviewed manuscripts, presentation in abstract form at scientific meetings and data sharing with other investigators through academically established means.
Trial registration number ClinicalTrials.gov Identifier, NCT04324762, registered on 27 March 2020.
- implementation science
- qualitative research
- quality improvement methodologies
- clinical protocols
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Deimplementing unnecessary health interventions is essential for improving population health and reducing unnecessary waste in healthcare and public health.1 It is estimated that 30% of medical interventions are unnecessary, suggesting that there are areas of medical overuse.2 One example of an overutilised resource is the use of chest radiographs after central venous catheter (CVC) insertions. The placement of CVCs is a common procedure performed, with 5 million placed annually and a cost of nearly US$500 million.3 4 The routine use of chest X-ray for CVC confirmation is an outdated practice that fails to take advantage of the now ubiquitous use of point-of-care ultrasound (POCUS) to guide CVC insertion and position confirmation.5–7 Chest X-ray solely for CVC confirmation is an overused resource because providers already using POCUS for CVC insertion can quickly use it to confirm catheter position confirmation and exclude pneumothorax immediately after the procedure.
Observational data and a randomised controlled trial have shown that POCUS can also provide similar yet faster diagnostic information to chest X-ray after CVC insertion, thus demonstrating superior efficiency.8–11 A POCUS-guided CVC confirmation protocol consists of three ultrasound imaging steps (figure 1). Three recent meta-analyses found that POCUS for CVC position confirmation was feasible (98% adequate visualisation), fast (reducing mean CVC confirmation time compared with chest X-ray), and accurate.8 10 12 In the randomised study, POCUS confirmation reduced the time from insertion to first use of CVC and reduced overall chest X-ray utilisation by 56.7% (p<0.0001).10 Thus, chest X-rays represents avoidable costs and resource utilisation to the healthcare system, results in ionising radiation exposure, and can cause delays in patient care.10 11 13–15

Point-of-care ultrasound-guided catheter confirmation protocol (after right internal jugular vein cannulation). CVC, central venous catheter; IJ, internal jugular; RASS, right atrial swirl sign.
Despite advantages of POCUS over chest X-ray, POCUS-guided CVC confirmation has a slow rate of clinical adoption.10 11 13–16 Even among providers with ultrasound experience, self-reported use of POCUS for CVC confirmation and deadoption of chest X-ray is low (1.5%), citing various barriers to this practice.17 18 This demonstrates an important gap, necessitating advance in this space. A deimplementation programme called DRAUP (deimplementation of routine chest radiographs after adoption of ultrasound-guided insertion and confirmation of central venous catheter protocol) is developed to take advantage of an evidenced-based innovation and deimplement low-value chest X-ray in the acute care environment. In this study, we will facilitate the adoption of the DRAUP programme with multifaceted strategies against identified barriers and evaluate implementation as well as effectiveness outcomes.
Methods and analysis
The implementation of the DRAUP programme has a three-phase approach: first, we will use qualitative methods to understand the context and barriers to change; in phase 2, we will identify and refine implementation and deimplementation strategies; and in phase 3, we will measure implementation and deimplementation outcomes. We have initiated the DRAUP programme in the emergency department (ED) and are beginning to use some of the strategies (January 2020) prior to phase 1. This study will be performed at a tertiary academic medical centre. The design and reporting of this study adhere to the Standards for Reporting Implementation Science and can be found in online supplemental file 1).19 Patients or the public were not involved in the design, and will not be involved in the conduct, or reporting, or dissemination plans of our research.
Supplemental material
Stakeholders’ engagement
Relevant stakeholders to implementing the evidence-based innovation include medical providers, the ED administrators who must support the DRAUP programme, and nurses who are taking care of the patient. Intensive care unit physicians and nursing leadership also serve as gatekeepers. Stakeholders and gatekeepers will be involved by participating in a qualitative exploratory analysis as well as empowering the institutional climate of change.
Study population, subjects and recruitment
In phase 1, we will conduct focus groups of practising critical care medicine and emergency medicine physicians to discuss current practices in POCUS-guided CVC confirmation. Participants will be recruited from our local health system, selected by purposive sampling, and carefully identified to reflect variations in practice settings (academic and community) to capture a broad range of beliefs towards CVC position confirmation practice.20 Motivation to participate is based on the voluntary selection of early adopters of POCUS-related innovations.21 Additional focus groups will include physician administrators and nursing leadership as stakeholders because they can foster a positive implementation climate and can ensure organisational readiness for change. Contact will be initiated via email requests for participation.
In phases 2 and 3, study participants will be senior (third & fourth year) emergency medicine residents and faculty members. This subject group will be chosen given previous data demonstrating adequate retention of ultrasound knowledge and skill for ultrasound guided CVC confirmation.22 Recruitment will be via email request for participation in protocol education and training. They will undergo a 60-min didactic training and will demonstrate adequate ultrasound image acquisition and interpretation.
Procedures, instruments and design
Phase 1: exploration by qualitative methods
A common exploratory framework called the Consolidated Framework in Implementation Research (CFIR)23 will be used to understand the contextual environment. Focus groups will be chosen to allow inductive facilitators and barriers to emerge in a group setting. An interview guide informed by the CFIR will be used for each focus group and is included in the online supplemental file 2). CFIR is a determinant framework and best fits our study goals about understanding the organisational and personal contexts that are preventing the deimplementation of chest X-ray after POCUS guided CVC confirmation. Field notes with written observations will be created during each focus group. We estimate approximately 4–8 focus groups made up of 5–7 physicians. This sample size is adaptative to the attainment of theme saturation, meaning focus groups will be continued until thematic saturation of barriers has been achieved.24–26 This qualitative data will inform implementation and deimplementation strategies that will be incorporated into the DRAUP programme.27
Supplemental material
Qualitative analysis
Focus groups and field notes will be recorded and transcribed verbatim by a professional transcription company. Research team members, experienced in qualitative research will independently code the deidentified transcripts for content (NVivo V.12, QSR Industries, Doncaster, Australia). A coding dictionary will be developed that includes specific definitions of each code and criteria for good examples of code applications.28 We will use the deductive codes created using CFIR constructs and inductive codes that are discovered in the coding of transcripts to generate a codebook. The coders will then independently recode all transcripts using the newly created codebook. Coding discrepancies will be reviewed with a qualitative methods expert.
Phase 2: adapting the implementation strategies within the intervention (DRAUP programme)
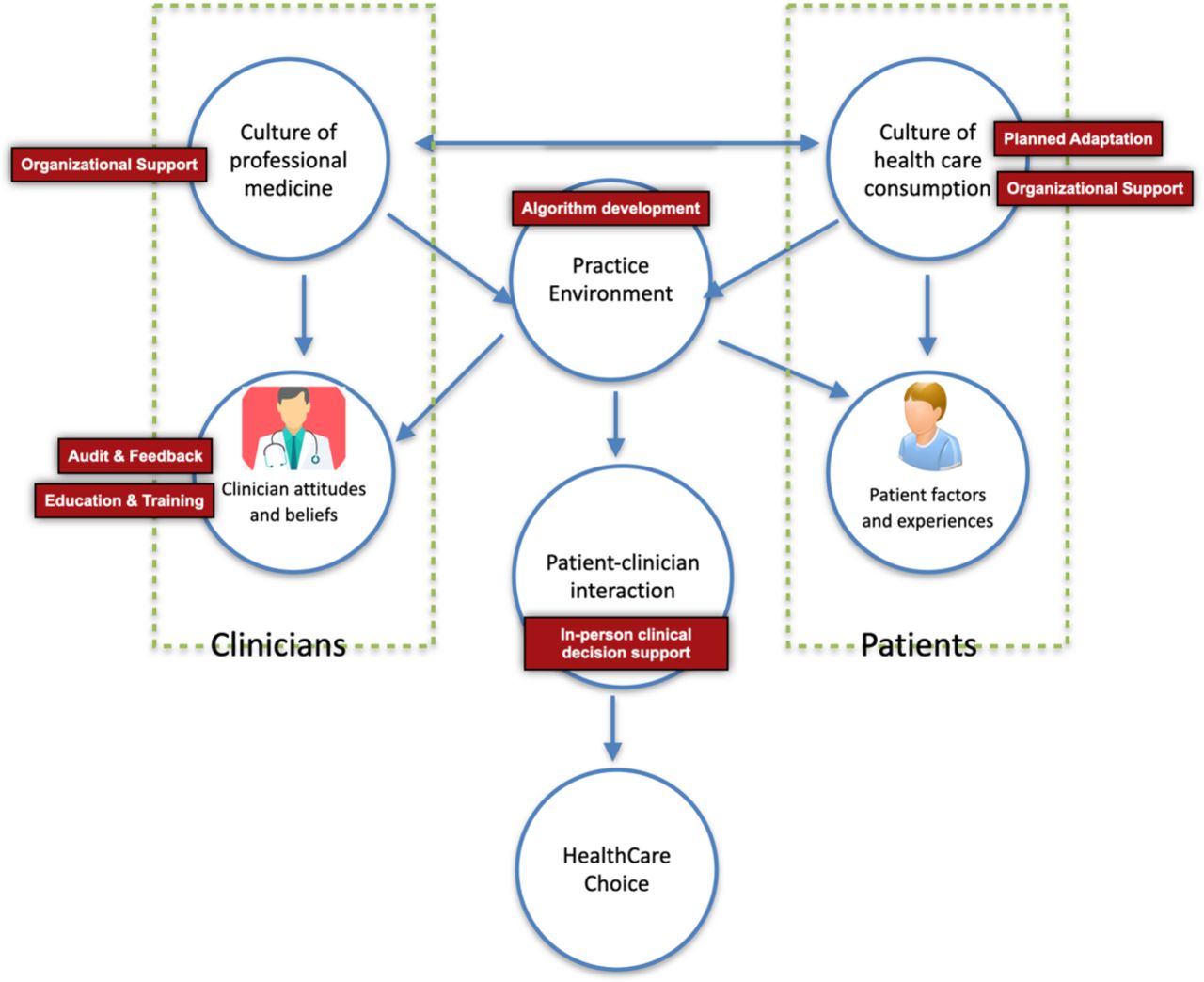
During the implementation phase, the DRAUP programme will include substitution of routine chest X-ray for POCUS after right internal jugular vein CVC insertion. The DRAUP programme will be guided by a second framework that highlights the specific process of deimplementation called Morgan’s framework for medical overuse and will tailor the strategies to any additional determinants identified in phase 1.29 This framework is a process framework allowing prioritisation of specific interventions towards understanding medical overuse and deimplementation (figure 2). The strategies will be evaluated after 1 year of implementation.
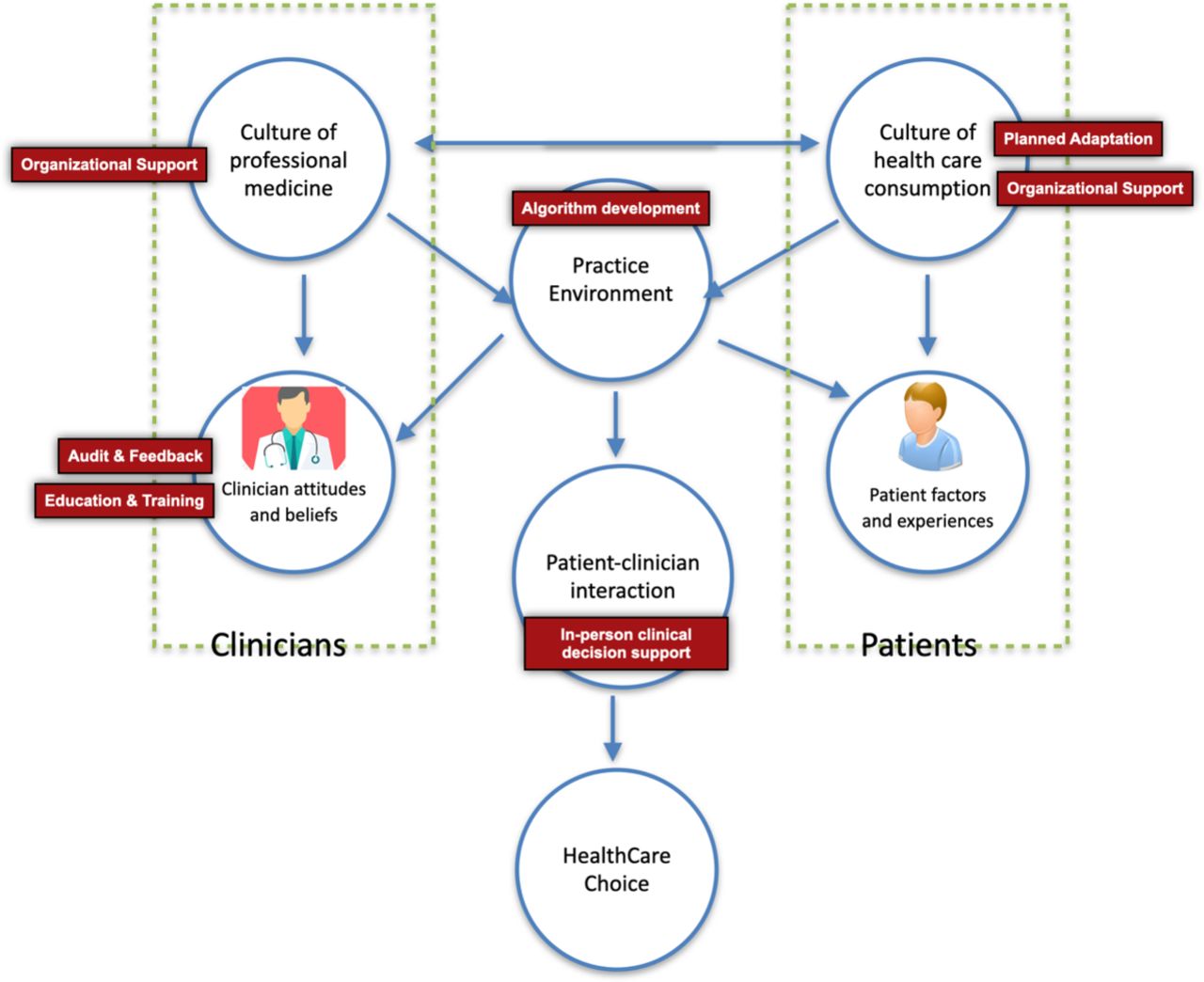
Morgan’s framework for conceptualising interventions to reduce medical overuse with embedded strategies from DRAUP (red) and their primary level of influence. (Source: Morgan et al29, 2017.)
Multifaceted strategies
We will identify and adapt multifaceted strategies (that targets both implementation and deimplementation) that we believe to be feasible, adaptable, generalisable and informed by our qualitative methods and Morgan’s framework for medical overuse29 in table 1. These strategies are initially selected to address the possible domains/drivers of influence for understanding medical overuse. Pragmatic details of our programme strategies are described in table 2 and strategy specifying and reporting30 table is available in online supplemental file 3). These strategies, while hypothesised to address known barriers, will be adapted based on new themes derived from the qualitative results from phase 1. These strategies are informed by Morgan’s framework and target interventions at the clinician, clinic environment, culture of healthcare and practice environment levels.29
Supplemental material
Implementation strategies informed by Morgan’s Practical framework for conceptualising interventions to reduce medical overuse (source: Morgan et al, 2017)
Description of specific applications of the multifaceted strategies to promote adoption of DRAUP
At the clinician level, strategies include (1) education and training (academic detailing) with interactive didactics, skill building workshops with follow-up,31 (2) clinical decision support with supervision,32 and (3) audit and feedback, we believe these three strategies to be the most effective strategies at the individual level to promote replacing an intervention with a new evidence-based intervention.33–35 Emergency medicine ultrasound expert faculty group will provide real time, in-person decision support (education, supervision) for the use of the DRAUP algorithm. Programme utilisation will include weekly electronic audit and feedback process in the ED (already part of the ED ultrasound imaging workflow) and monthly summary and assessment to see if there is cumulative change in practice.34 This frequency of audit and feedback will allow us to perform sensitivity analyses that will be used to identify the optimal timeframe to perform audit and feedback for future larger scale projects.35
To address the culture of change, we will focus on strategies that effect clinic/organisational level such as (4) leadership support/endorsement.36 37 For strategies at the practice environment level, (5) an algorithm38 demonstrating a specific POCUS-guided CVC confirmation was created. After adequate planning and organisational support of the protocol (compliant with hospital process and procedures), we will disseminate the DRAUP algorithm to ED stakeholders including department administration, nursing leadership and intensive care unit leadership (figure 3). We will review the implementation strategies quarterly and revise the intervention based on poor interest or fidelity.39 Any implementation strategy modifications made to fit clinician or clinic characteristics that occur will be reported as a (6) planned adaptation.40 41

DRAUP (deimplementation of routine chest radiographs after adoption of ultrasound -guided insertion and confirmation of central venous catheter protocol) algorithm for deimplementation of chest radiography after central line insertion. POCUS, point-of-care ultrasound; IJ, internal jugular vein; CVC, central venous catheter; PACS, picture archiving and communications system; DRAUPOUT/.DRAUPIN, electronic record documentation template of findings; CXR, chest X-ray
Outcomes
Phase 3: evaluation using implementation and deimplementation outcomes
During the evaluation phase, implementation and deimplementation outcomes from Proctor’s conceptual model for implementation research framework will be used to evaluate the success of the strategies described in phase 2.42 This is an evaluation framework and will focus on adoption, deadoption, fidelity and penetration as the most optimal outcomes of deimplementation. Operationalisation of the constructs measured using Proctor’s framework is demonstrated in figure 4.43 The selected outcomes and their measures are reported on table 3. Unintended negative consequences to consider include premature use of the DRAUP programme outside of the acute care environment without adequate training (short-term) or decreased confidence interpreting a chest X-ray for CVC confirmation (long term).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Operationalisation of implementation plan using Proctor’s conceptual model for implementation research (source: Proctor et al, 2009) with embedded DRAUP (deimplementation of routine chest radiographs after adoption of ultrasound-guided insertion and confirmation of central venous catheter protocol) strategies and outcomes. ED, emergency department; POCUS, point-of-care ultrasound.
DRAUP implementation and effectiveness outcomes and measures
Successful deimplementation outcomes will be defined as outcomes that persist after 1 year of strategy integration. This timeframe was chosen given the following characteristics: strength of evidence, magnitude of the problem and characteristics of the intervention. The ED selected for this proposal has an average of 260 supradiaphragmatic CVCs placed per year. With the selected strategies, we define an increased adoption of the DRAUP programme (accompanied by a deadoption of chest X-rays) of at least 50% at 1 year as a marker of successful implementation. We hypothesise that there will be interval increases in fidelity and overall penetration of the DRAUP protocol within the ED over the 1-year timespan.
Adoption and deadoption
Adoption is defined as the intention, initial decision or action to try or employ an innovation or evidence-based practice.42 Deadoption is the discontinuation of a clinical practice after it was previously adopted.44 Adoption of the DRAUP programme will be measured by the number of occurrences where POCUS is used for CVC confirmation. Deadoption will be measured by the number of chest X-rays deemed unnecessary after POCUS-guided CVC confirmation. After 1 year, we will also measure uptake by conducting a postimplementation survey of attitudes and perception to expand and more deeply understand the providers’ decision, as it is influenced by core elements of appropriateness and feasibility.45 46 A physicians risk tolerance profile may impact their adoption of a new innovation like the DRAUP programme.47 Thus, we will also evaluate participating physicians risk profiles using three validated survey instruments (malpractice fear scale,48 risk-taking scale49 and stress from uncertainty scale47). Assessing the physician’s risk profile will extend the understanding in this area by testing the risk association and their intent to adopt the DRAUP programme.
Fidelity
Fidelity, the degree to which an intervention was implemented as it was prescribed, will be measured to assess the internal validity of the clinical outcomes.42 In this context, fidelity will be assessed by measuring the adherence to the programme when attempted.42 Adherence, defined as the utilisation of the procedures of a protocols within the DRAUP programme, will be measured by documentation in the electronic medical record. Fidelity will be assessed by measuring adherence to the DRAUP protocol (assessed monthly by audit & feedback) and the adequacy of the stored POCUS images in the medical record (evaluated by the ultrasound expert faculty).
Penetration
Penetration is the integration of a practice within a service setting and its subsystems specifically, the number of eligible persons who use a service, divided by the total number of persons eligible for the service.50 Penetration also can be calculated in terms of the number of providers who deliver a given service or treatment, divided by the total number of providers trained in or expected to deliver the service. The electronic medical record will measure this outcome by calculating the number of actual CVC insertions where POCUS was used divided by the number of possible CVC insertions where POCUS could have been used. After 1 year, a 50% reduction in post CVC insertion chest X-ray will be a marker of successful internal penetrance of substitution of routine chest X-ray for POCUS after DRAUP. Penetration outside the ED will be assessed by measuring the proportion of cases where the receiving clinician does not immediately obtain a chest X-ray after the patient arrives to the ICU.
Distal outcomes
In addition to the proximal implementation outcomes, distal outcomes such as service outcomes will be evaluated. Efficiency and effectiveness are service outcomes that are important to long-term sustainability of DRAUP and can be measured using data from the electronic medical record.42 Clinical efficiency has always been a benefit of POCUS.8 Efficiency in this context is measured by the time needed to perform the POCUS-guided CVC position confirmation compared with ordering and performing a chest X-ray. Clinical effectiveness is measured by the diagnostic accuracy of POCUS-guided CVC confirmation compared with in-hospital chest X-rays (which will be obtained at some point during the patient hospital stay). Descriptive analysis with accuracy, sensitivity and specificity will be calculated for POCUS-guided CVC confirmation using chest X-ray as the reference standard.
Sample size
Patients will be enrolled for approximately 12 months to: (1) decrease the chance that any seasonal/temporal trends could skew the data and (2) achieve an adequate sample size. As this is an observational study, the primary implementation and effectiveness outcome of the DRAUP programme is more descriptive than inferential on a hypothesis test between two treatment groups. The sample size should, therefore, be large enough to observe an event with a high degree of probability and with sufficient precision. Over the course of a year, we expect 5 patients per week to fulfil inclusion criteria and be eligible. With an inclusion of just under one patient every 2 days, on average, we expect to have 150 patients eligible for enrollment in the study during the year.
Innovation
This study contains several important innovations. First, the use of POCUS as a substitute for chest X-ray for CVC confirmation is a relatively new implementation phenomenon although the evidence has been present for over a decade. Although data support the use of POCUS as the first approach for CVC confirmation, current practice patterns demonstrate that its use is non-existent.17 18 Radiography has been the standard method for confirming CVC placement for over 50 years. The DRAUP programme would be a substantial change in the standard of care thus creating a critical translational gap for innovation implementation. With limited data currently available to inform interventions, we believe that our results will fill a knowledge gap.
Second, a combined approach towards implementation and deimplementation strategies is innovative. The strategies that affect deimplementation may overlap with those that affect implementation.44 Many innovations in healthcare require a simultaneous adoption of one practice and deadoption of another previously valued practice to impact the patient.51 Implementation strategies that support POCUS-guided CVC confirmation do not guarantee deimplementation of the chest X-ray at the provider or organisational level given the asymmetry in human behaviour.52 53 The activities required to deimplement a practice, through substitution, might not be the simple inverse of those needed for implementation and diffusion.53
Finally, the utilisation of three different frameworks adds comprehensive approach to implementation science efforts to change one clinical practice. The multifaceted approach using use a determinant framework, a process framework, and an evaluation framework are relatively novel in this context.
Impact
Current CVC confirmation by chest X-ray is an outdated and frequently overused resource. Clinicians already using POCUS for CVC insertion can quickly use POCUS immediately after the procedure with no further confirmatory steps or resources needed. The DRAUP programme would be best suited for academic medical environments where ultrasound equipment and ultrasound knowledge is standardised demonstrating adequate social validity and acceptance of POCUS among early adopters.54 This study has the potential to impact public health by increasing our understanding of simultaneous implementation and deimplementation of physician behaviour based on their risk profiles. Findings from this study will have the potential to inform future policy mandates around implementation and substitution. Findings will also add to the implementation science literature by providing information on the impact of policy on implementation of evidence-based innovations and the potential moderating effect of organization-level and leader-level variables on implementation. Finally, the study has the potential to improve the quality of care to patients and healthcare systems by improvements in resource utilisation and diagnostic efficiency.
Limitations
This is an observational study at a single-centre location evaluating a clinical practice that has been historically difficult to change. Our study will not describe any causal relationships between proposed implementation strategy and measured outcomes, only associations. Our implementation and deimplementation strategies will be cumulative; thus, this study is not designed to identify which strategy(ies) are driving the implementation outcome. Finally, this study does not evaluate if adoption of the DRAUP programme will be sustained after initial implementation plan with the multifaceted strategies. Future studies assessing the implementation plans also should include this as outcome.
Data storage and management
All data will be entered by the study team and data accuracy will be verified by the study principle investigator. Data quality control measures will include queries to identify missing data, outliers and discrepancies. Only study team members will have access to protected health information. The data will be uploaded and stored using Research Electronic Data Capture (RedCap), a web-based data management application. All computers will be password protected and encrypted per university policy.
Dissemination and data sharing
To enhance reporting transparency, this study will be reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology Statement: Guidelines for Reporting Observational Studies. Data and resources will be shared with other eligible investigators through academically established means. The datasets used and/or analysed during the study will be available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Study procedures have been approved by the Washington University Institutional Review Board (#202004042). Study enrolment began in January 2020 until March 2020 (paused because of COVID-19), resumed in July 2020.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors EAA is the PI on the study, led the protocol development, conception and study design, acquisition of data, analysis and interpretation of data, drafting and revising the manuscript. BP, VM and RG have been integral to the development of the study protocol, planned analysis and interpretation of data, drafting and revising the manuscript. AJ, CC and MK are involved in analysis design and interpretation of data, drafting and revising the manuscript. SK is a qualitative moderator, involved in data collection and revising the manuscript. All authors read and approved the final manuscript.
Funding EA is funded by the Washington University School of Medicine K12 Mentored Training in Implementation Science grant, Grant Number: K12HL137942. BP is supported by the National Institute of Mental Health K01MH113806; VM is supported by the Institute of Clinical and Translational Sciences grant UL1TR002345 from the National Centre for Advancing Translational Sciences of the National Institutes of Health. AJ is supported by the Siteman Cancer Centre and the Barnes Jewish Foundation. CC is supported by grants from the John A. Hartford Foundation and West Health Institute. RG is supported by grant 1 R18 R18 HS025052-01 from the Agency for Healthcare Research and Quality, grant P30DK092950 from the NIH/National Institute of Diabetes and Digestive and Kidney Disorders, Washington University Centre for Diabetes Translation Research.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.