Article Text

Abstract
Introduction Handover is the system by which the responsibility for immediate and ongoing care is transferred between healthcare professionals and can be an area of risk. The Royal College of Physicians (RCP) has recommended improvement and standardisation of handover. Locally, national training surveys have reported poor feedback regarding handover at Glasgow Royal Infirmary.
Aim To improve and standardise handover from weekday to weekend teams.
Methods The Plan–Do–Study–Act (PDSA) quality improvement framework was used. Interventions were derived from a driver diagram after consultation with relevant stakeholders. Four PDSA cycles were completed over a 4-month period:
PDSA cycle 1—Introduction of standardised paper form on three wards.
PDSA cycle 2—Introduction of electronic handover system on three wards.
PDSA cycle 3—Expansion of electronic handover to seven wards.
PDSA cycle 4—Expansion of electronic handover to all non-receiving medical wards.
The outcome of interest was the percentage of patients with full information handed over based on a six-point scale derived from the RCP. Data were collected weekly throughout the study period.
Results 18 data collection exercises were performed including 525 patients. During the initial phase there was an improvement in handover quality with 0/28 (0%) at baseline having all six points completed compared with 13/48 (27%) with standardised paper form and 21/42 (50%) with the electronic system (p<0.001). When the electronic handover form was expanded to all wards, the increased quality was maintained, however, to a lesser extent compared with the initial wards.
Conclusion A standardised electronic handover system was successfully introduced to downstream medical wards over a short time period. This led to an in improvement in the quality of handover in the initial wards involved. When expanded to a greater number of wards there was still an improvement in quality but to a lesser degree.
- hospital medicine
- quality improvement
- continuity of patient care
Data availability statement
Data are available on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Glasgow Royal Infirmary (GRI) is a large teaching hospital located in central Scotland with approximately 1000 inpatient beds. The medical departments consist of an acute assessment area for direct general practitioner admissions, 5 multispecialty receiving wards (respiratory, general medicine, gastroenterology, cardiology and stroke/department of medicine for the elderly), a medical high-dependency unit and 29 downstream medical wards.
Handovers between junior doctors occur twice daily on receiving wards and the acute assessment area. On downstream wards there are morning, early evening and night-time handovers 7 days a week. At the weekend, downstream wards are covered by an out of hours (OOH) team of junior doctors who are usually unfamiliar with the patients on the wards they are covering. It is therefore the responsibility of ward doctors during the week to leave a handover for the OOH team. The volume of patients in downstream wards is such that the weekend doctors have to select which patients to review based on reports from nursing staff and those patients who have been ‘flagged’ in the handover from the weekday team.
In the 2017 Scottish national training survey, handover was ‘red-flagged’ as an area of concern among junior doctors across multiple medical specialties within GRI.1 Most handovers lacked senior supervision (ie, specialty registrar or above). There was no agreed proforma or structure to help ensure important information about each patient was included in the handover. Furthermore, downstream handovers were typed or handwritten and left on the ward for the OOH team to find. There was no standard location for these to be found meaning they could be lost altogether, and when found, the OOH team would have no opportunity to clarify handover content or ask questions.
Following the national training survey results, it was decided to attempt to improve the quality of medical handover in GRI. A quality improvement (QI) forum was formed and decided to focus on improving handover quality. This forum consisted of core medical trainees (CMTs) and the ‘Chief Resident’ (RC), supervised by the CMT Training Programme Director (JB) and other interested senior clinicians (MD and BC-K). Several subgroups were formed and here we focus on improving the quality of the weekend medical handover on downstream medical wards.
Aim
The aim of this project was to improve the quality of weekend medical handover on downstream medical wards at GRI, as measured by a six-component scale.
Background
Medical handover has been defined as ‘the transfer of professional responsibility and accountability for some or all aspects of care for a patient, or group of patients, to another person or professional group on a temporary or permanent basis’.2 When done well, it enables safe patient care between teams allowing information about unstable patients, problems from the previous shift and outstanding tasks to be prioritised and passed on to those assuming patient responsibility. Handover is one key to efficiency, patient safety and patient experience. However, when handover is inadequate there is significant potential to cause patient harm. Handover is therefore deemed a high-risk clinical activity that requires time, structure and leadership to perform effectively.2
Since the introduction of the European Working Time Directive doctors’ patterns of work in the UK have changed, with an increase in shift work and a reduction in continuity of care.2 This has led to an increase in the number of handovers, creating greater opportunity for harm. It is therefore more vital than ever that handovers are carried out effectively in order to facilitate safe care.
Using a structured patient handover communication system in an internal medicine setting may reduce avoidable adverse events and in recent National Institute for Health and Care Excellence (NICE) guidelines deemed to be cost-effective with a cost of £180 per Quality-Adjusted Life Year (QALY) gained.3 In addition to befitting patients, a structured communication system can also help doctors feel more informed on the patients they are caring for as well reducing the time needed to go through admission notes.4 Overall good structured handover communication is beneficial to patients and doctors.
Measurement
Using guidance from the Royal College of Physicians (RCP) handover toolkit5 and BMA,6 as well as the widely used handover mnemonic SBAR (Situation, Background, Assessment and Recommendation),7 we developed a six-component scale which we decided to use as our quality outcome measure. This included patient identification (name and community health index number), current situation/problem, background/medical history, assessment/current state, recommendation/reason for review and resuscitation/escalation plan. We measured the completeness of patient handovers by measuring the proportion of completed components for all patients handed over in downstream wards.
Design
A driver diagram was produced to explore contributing factors to poor handover quality and potential solutions (figure 1). There were multiple aspects of handover recognised as being suboptimal. We decided to focus efforts on improving the quality of handover of individual patients. Standardised handover forms were a potential solution to improve handover quality by providing a structure for junior doctors to use when handing over patients. An electronic handover would have the additional advantage of being in a secure location, remotely accessible and easily auditable.
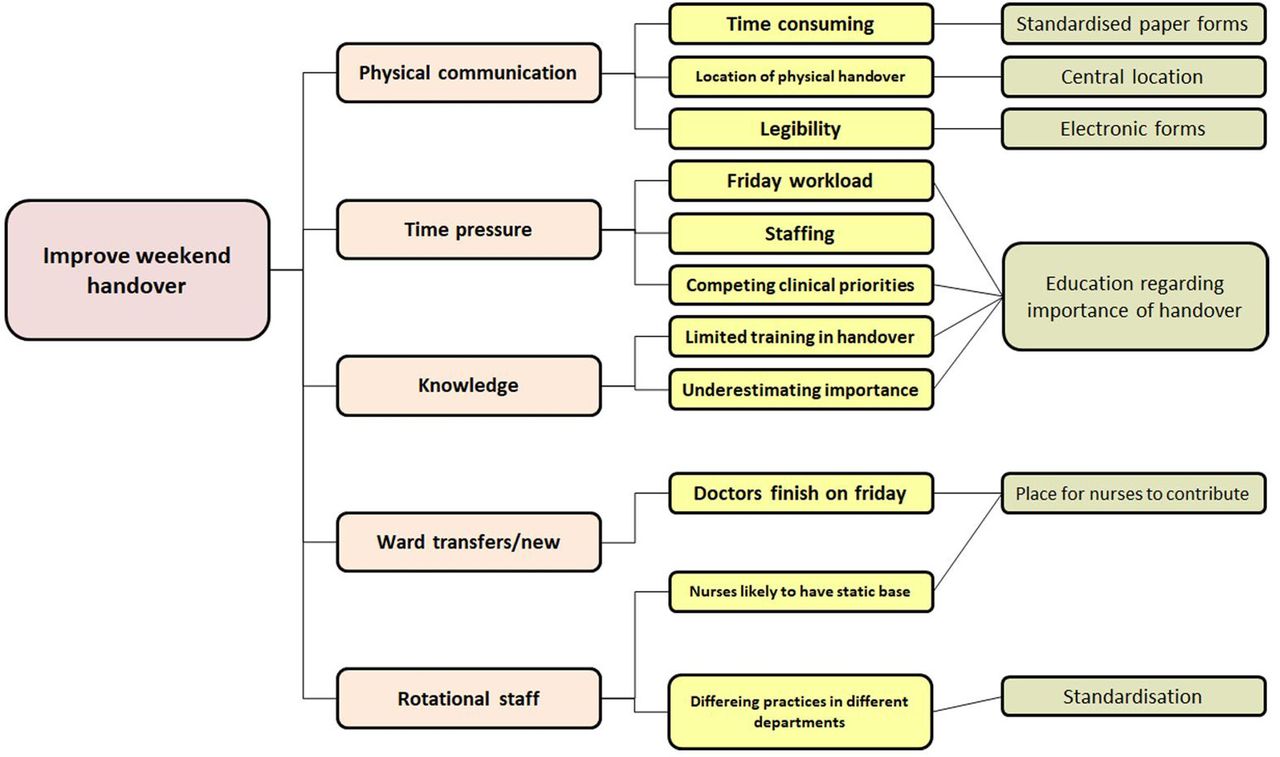
Driver diagram illustrating factors affecting handover.
Differences between handover completion rates were compared using the χ2, Student’s t-test and analysis of variance (ANOVA) tests. Statistical analyses were performed using SPSS V.21.0 (SPSS) and were considered significant if p<0.05.
Strategy
We completed a total of four Plan–Do–Study–Act (PDSA) cycles. Initially we identified three medical wards on which we would pilot the project. We collected baseline data for these then introduced a paper document which standardised the domains covered in the handover, again on the same three wards. These domains were mapped to the extended SBAR model covered above. On week 8 of the project, we migrated handover to an electronic format. The form itself covered the same data points as its paper version, although in a different format, and was based on a software platform called TrakCare. This application is used across the Health Board as its Patient Management System. This allows doctors to select patients from real-time ward plans without having to manually re-enter patient demographics. This was achieved with the hospital’s Clinical eHealth Lead (BC-K). Weekday doctors handing over on a given weekend were approached by QI team members during the week before for one-on-one training. Likewise, weekend doctors receiving the e-Handovers were also identified and trained. A total of 125 doctors across all grades were trained.
Once e-Handover was successfully established on the three pilot wards the expansion phase of the project commenced. The e-Handover was expanded to seven wards and then to all other downstream medical wards. The total duration of the project was 18 weeks. E-Handover is now well established in all studied wards. This is the summary of the completed PDSA cycles:
Introduction of standardised paper form on three wards.
Introduction of electronic handover system on three wards.
Expansion of electronic handover to seven wards.
Expansion of electronic handover to all 17 non-receiving medical wards.
Results
A total of 18 weekly data collection exercises were completed. The number of weeks for each PDSA cycle ranged from 1 to 5. A total of 525 patient handovers were included for study. The number of patients per PDSA cycle ranged between 28 and 218. Table 1 shows the number of patients per PDSA cycle. Electronic handover is now established in 17 wards. For analysis, two groups were considered: the initial cohort (PDSA 1 and 2) and expansion cohort (PDSA 3 and 4).
Table showing the number of patient handovers and weeks for each phase of the project
A range of wards and specialties were included in the study. All wards have a mix of general medicine and specialty patients. The initial cohort consisted of endocrinology wards (3 wards). The first expansion was then into the respiratory department (4 wards) and then on to cardiology, acute medical, gastroenterology and rheumatology (total of 17 wards). The department of medicine for the elderly was not included at time of the project but has subsequently adopted the same process.
Initial cohort: three pilot wards
A total of 118 patient handovers were completed in the pilot 3 wards over PDSA cycles 1 and 2. There was a steady increase in completion rate of the six component scale within the pilot 3 wards (figure 2). At baseline 0/28 (0%) had all six points completed, with standardised paper form 13/48 (27%) and with the electronic system 21/42 (50%) had all six points completed (χ2 p<0.001).
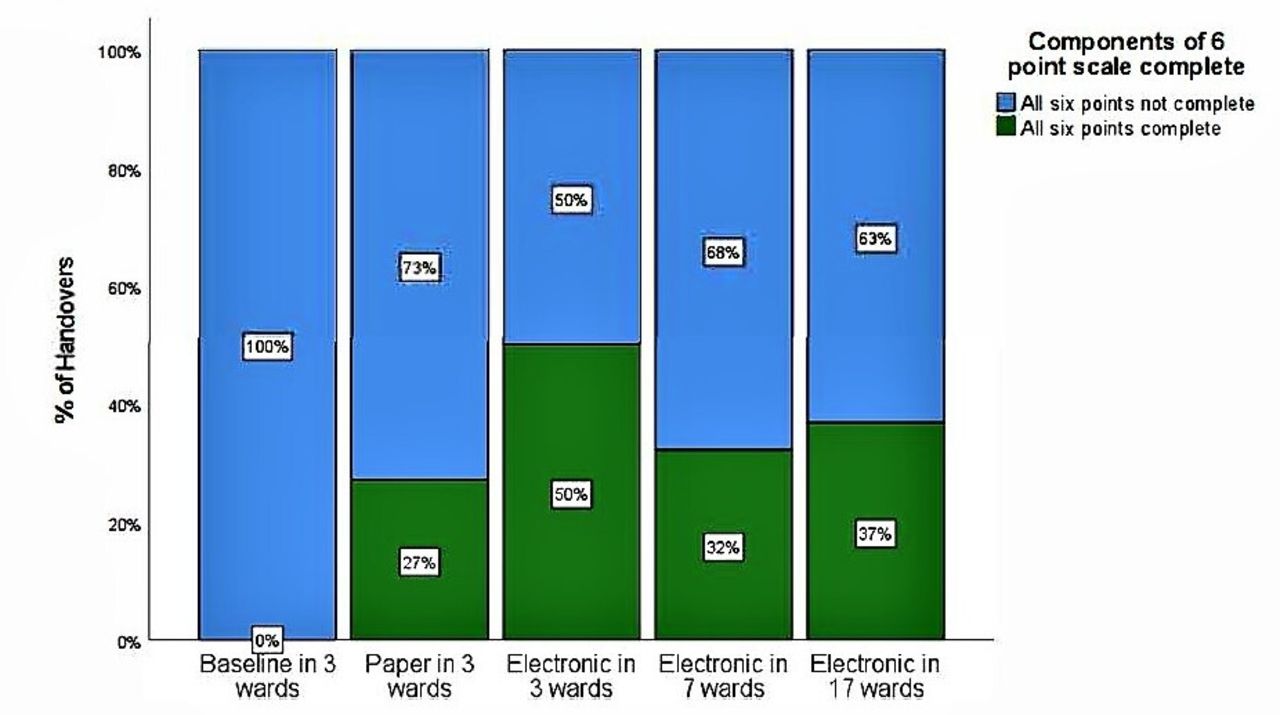
Bar chart showing the proportion of handovers fully compliant with the six-component scale for each phase of the project.
The mean number of points completed of the six point scale was 4.54 at baseline, 4.85 with paper forms and 5.31 with the electronic system (ANOVA p=0.001). The most frequently omitted piece of information across all groups was escalation/resuscitation plan with only 43% of patients having this documented. Overall the introduction of a standardised electronic handover system improved the information handed over in our pilot cohort.
Expansion cohort: 7 wards then 17 wards
PDSA cycles 3 and 4 represent the expansion phase in the project where the electronic format was rolled out into 7 then 17 wards. In the final PDSA cycle with all 17 wards involved, 80/218 (37%) of patients had all points of the six-component scale completed which was significantly higher than baseline measurements (χ2 p<0.001). The highest completion rate was when the electronic system was introduced to the three pilot wards.
The mean number of points completed for each PDSA cycle was 4.54 (baseline), 4.85 (PDSA1), 5.31 (PDSA2), 4.92 (PDSA3) and 4.96 (PDSA4).
Figure 3 shows the run chart of the mean number of points of the six component scale completed for each week. There was continued improvement compared with baseline throughout the study period with the maximal improvement being when the electronic format was enrolled in the pilot wards. The mean number of points completed for each PDSA cycle was 4.54 (Baseline), 4.85 (PDSA1), 5.31 (PDSA2), 4.92 (PDSA3) and 4.96 (PDSA4).The mean number of points completed was marginally higher in the final PDSA group compared with baseline (4.96 vs 4.54, t-test p=0.049).

{kind=link}
{kind=link}
{kind=link}
Run chart showing mean number of points complete for each week of the study period. PDSA, Plan–Do–Study–Act.
The frequency of which individual components of the six point scale were completed differed (table 1). Of the total 526 handovers, the majority included patient identification 519 (99%), current situation/problem 510 (97%), background/past medical history 416 (79%), assessment/current state 470 (89%) and recommendation/reason for review 480 (91%). However, escalation status was consistently poorly completed with only 204 (39%) of handovers having a resuscitation/escalation plan handed over to the weekend team.
Lessons and limitations
We have successfully established a new standardised electronic weekend handover communication system in GRI which has been adopted and now established in all non-receiving medical wards. We have evidenced a sustained improvement in the completion of handovers during the study period. The biggest improvement in the completion of handovers was achieved when the electronic handover system was rolled out across the original pilot wards. As the project was scaled further this effect was diluted but the rate of full handover completion remained higher than our baseline measurements. Overall we have shown that a large scale endeavour to standardise practice over many departments is achievable over a modest timescale.
In providing a fixed framework for handover, we guided practitioners handing over to their weekend colleagues. However, there are some limitations to this study. Elements of the electronic handover were not mandatory and could be submitted in such a way that missed data fields or failed to cover the question being asked. The training we carried out focused on the technical side of using the new system and did not necessarily highlight the importance of handover in a way that motivated practitioners to use it to its full potential. There were also no interventions to combat the ‘Friday afternoon workload’ effect. This meant practitioners still had to produce a handover in the context of the pressure of wrapping up multiple loose ends before the weekend. Finally, this project focused purely on the completion and inclusion of key variables and accuracy for each case was not assessed. Likewise we only recorded those patients that had a handover created and not those who perhaps should have been handed over but were not. Targeting those elements could constitute a future step in QI in this area. We also do not have data on patient outcomes following the changes in handover practice. However it is recognised by the RCP, BMA, NICE and patient safety groups that handover is key for good clinical care.
Escalation status was poorly documented throughout all phases of the project. Potential escalation decisions are often difficult for more junior medical staff to make. Our 39% completion is in keeping with previous studies (9.1%–41.1%).8 Treatment escalation plans (TEPs) are one way senior clinicians can make escalation decisions in advance so as removing ambiguity for junior medical staff. Often TEPs include making decisions regarding resuscitation and ‘higher’ levels of care such as high dependency and intensive care. Adoption of TEPs are becoming more common in clinical settings.
This project highlights the QI Forum as a catalyst for change. It enabled 125 doctors to be trained on a new system easily though peer to peer learning. It brought together keen trainees and senior colleagues who were able to bring about the changes in electronic systems needed for improving handover. The migration to an electronic handover process in itself represents a success. All the doctors were already very familiar with the platform that was used as they already use it daily for their ward work including requesting all tests and imaging. This meant that there was no need to provide any new user accounts and training requirements were minimal as the process was very similar to requesting a test. As healthcare providers move towards using digital platforms for multiple purposes, from prescribing to requesting imaging and laboratory tests, the medicolegal advantages of having a system that automatically logs handovers in a permanent audit trail are clear.
Conclusion
The introduction of a standardised electronic weekend handover communication system is feasible and achievable in a large hospital. We demonstrated a significant improvement in the completion of handovers when this standardised handover was introduced particularly in the wards piloting the system. When this was enrolled throughout the medical unit there was still an improvement in handover completion however to a smaller degree. With a standardised platform now established, other interventions can be tested to further improve quality of weekend handover. The GRI QI Forum was the key driver for this change.
Data availability statement
Data are available on request.
Ethics statements
Patient consent for publication
Acknowledgments
The Glasgow Royal Infirmary Quality Improvement Forum. NHS Greater Glasgow and Clyde eHealth Directorate.
Footnotes
RN, MW and LLH contributed equally.
Contributors RN, MW and LLH are considered joint first authors. MW and RN were contributed to study concept, planning, data collection, analysis, drafting and approving manuscript. LLH contributed to data collection, analysis, drafting and approving manuscript. RC contributed to study concept, planning and manuscript approval. MD contributed to study concept and manuscript approval. BC-K contributed to study concept, planning, development and delivery of electronic handover system and approving manuscript. JB contributed to study concept, planning, data collection, analysis, drafting and approving manuscript as well as overall supervision and guarantor of study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.