Article Text

Abstract
Aim To improve communication on the medical ward round with patients with limited English through implementation of a medical communication chart.
Local problem King’s College Hospital (KCH), London, is situated in Southwark in which 11% of households have no members that speak English as a first language, 4.1% of London’s population report they do not speak English well. Language barriers impair healthcare delivery including during daily ward rounds. This has been exacerbated by the need for PPE during the SARS-CoV2 pandemic. Effective communication between healthcare teams and patients is essential for high quality, patient-centred care. Communication tools commonly used include online, telephone and face-to-face translation services but these have limitations.
Methods Face-to-face patient questionnaires were conducted in the pre-QIP (baseline) group to assess communication on medical ward rounds. Medical communication charts were designed by adapting pre-existing aids commonly used by speech and language therapy. Charts were translated into commonly spoken languages among KCH inpatients. Patients with limited English were selected from both COVID-19 and non-Covid wards. Preintervention and postintervention questionnaires were completed in three Plan–Do–Study–Act (PDSA) cycles.
Results At baseline, patients agreed or strongly agreed that the ward round addressed physical symptoms (8/8), concerns or anxieties (7/8), ongoing needs (7/8). Only two of eight doctors felt they could communicate effectively with patients. In PDSA 1, four of five patients reported high satisfaction in communicating physical symptoms, anxieties or concerns preintervention with five of five postchart implementation. Five of five patients reported high satisfaction in communicating ongoing needs preintervention but only three of five postintervention. In PDSA 2, two of five patients reported increased satisfaction in communicating physical symptoms, concerns or anxieties with four of four doctors reporting improved satisfaction in communication in PDSA 2 and two of three doctors reporting higher satisfaction in communication in PDSA 3.
Conclusion Using communication charts in patients with limited English can improve bidirectional communication on medical ward rounds.
- quality improvement
- communication
- hospital medicine
- COVID-19
- patient-centred care
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
According to the Office for National Statistics for England and Wales,1 nearly 4.1% of the London population report they are unable to speak English well (up to 8.7% in the Borough of Newham) compared with a national average of 1.3%; with 0.3% of the population of England and Wales reporting that they cannot speak English at all.
King’s College Hospital (KCH), London, is a tertiary centre and Central London teaching hospital located in Camberwell (situated in the Borough of Southwark). Southwark is a multicultural, multinational and multilingual borough in London. Over 120 languages are spoken in Southwark and 11% of households have no members who speak English as a first language.2 For this reason, there is a risk of inequitable healthcare delivery due to language barriers in the healthcare setting. Communication on daily ward rounds is challenging within a diverse patient demographic. KCH itself is one of London’s largest and busiest teaching hospitals and is a Major Emergency Centre for the South East, a major trauma centre, hyperacute stroke unit and cardiac arrest centre.3 KCH National Health Service (NHS) Foundation Trust has approximately 1638 inpatient beds with approximately 176 545 inpatient admissions; 1 869 207 outpatient appointments and 229, 730 Emergency Department attendances between July 2017 and July 2018.4
Previous research5 has found clinicians’ use of technical language was over 60% on medical ward rounds observed and was associated with patients feeling excluded with reduced patient participation on inpatient ward rounds, while the lack of ability to communicate in critical care settings puts patients at greater risk of poor treatment and delayed rehabilitation.6 Visual aids with updated daily care plans have been found to improve inpatient satisfaction by 24.5% and nurse satisfaction by 20.3%7 even without the added complexity of language barrier in patient–provider communication.
A number of existing communication aids and technologies are in use, but have limitations for daily medical ward rounds which require efficient and timely communication. Telephone translators require access to cordless phones, online translation apps may not be accurate and arranging face-to-face translators is not practical for daily ward rounds. Common problems identified in using telephone translators are that cordless phones were not available on wards, not charged adequately and the telephone translation service did not have the language required. Face-to-face translators were almost entirely absent during the peak of the COVID-19 pandemic due to concerns about risk and transmission; and family members were not permitted to visit patients in line with strict visiting criteria. Using family members as translators can be extremely helpful especially for contributing to better patient understanding of their disease,8 however, can reduce patient confidentiality and may limit honest communication about patient concerns and preferences due to non-third-party translation.9 Additionally, the use of N95 masks and face shields for Personal Protective Equipment during the COVID-19 pandemic has been found to impair speech perception10 among healthcare professionals requiring alternative communication strategies adapted for medical care in the pandemic and postpandemic setting.
Using non-verbal communication, for example, physical gesturing cannot be relied on for accurate assessment of patients’ daily symptoms on medical ward rounds; it is a one-way form of communication between the medical team and the patient and does not address current or ongoing patient needs or concerns.
Communication charts with pictures are regularly used by speech and language therapy (SALT) for patients who have problems in secondary language acquisition for example, poststroke or with primary language difficulty. These communication charts are adapted to the SALT setting and cover basic nursing procedures such as medication rounds, suctioning and oxygen use.
Measurement
We designed patient questionnaires to capture satisfaction with communication on daily medical ward rounds between the medical team and patients with limited English on COVID and non-COVID medical wards. We gathered baseline data on how effective they found communication in identifying and addressing their ongoing needs as well as free text answers for suggestions on improvement. We then designed and implemented communication charts and conducted preintervention and postintervention questionnaires gathering the same data to see if communication was improved by the use of the communication charts. We aimed to repeat postchart questionnaires at day 1, day 3 and day 5 postchart implementation over a 2-month period.
Pre-Quality Improvement Project (QIP) and post-QIP questionnaires assessed patient and doctor satisfaction in communication on the medical ward round using 5-point Likert scales (strongly disagree=1 point, disagree=2 points, neither agree nor disagree=3 points, agree=4 points and strongly agree=5 points), yes/no questions (yes=1, no=0) and free-text answers.
Design
We reviewed four recommended communication charts used by SALT at KCH. These communication charts included three charts which were used in medical settings11–13 and one chart14 which was tailored to the COVID-19 pandemic.
We designed a communication chart which was adapted from the four communication charts to specifically target the medical ward round on both COVID and non-COVID wards.
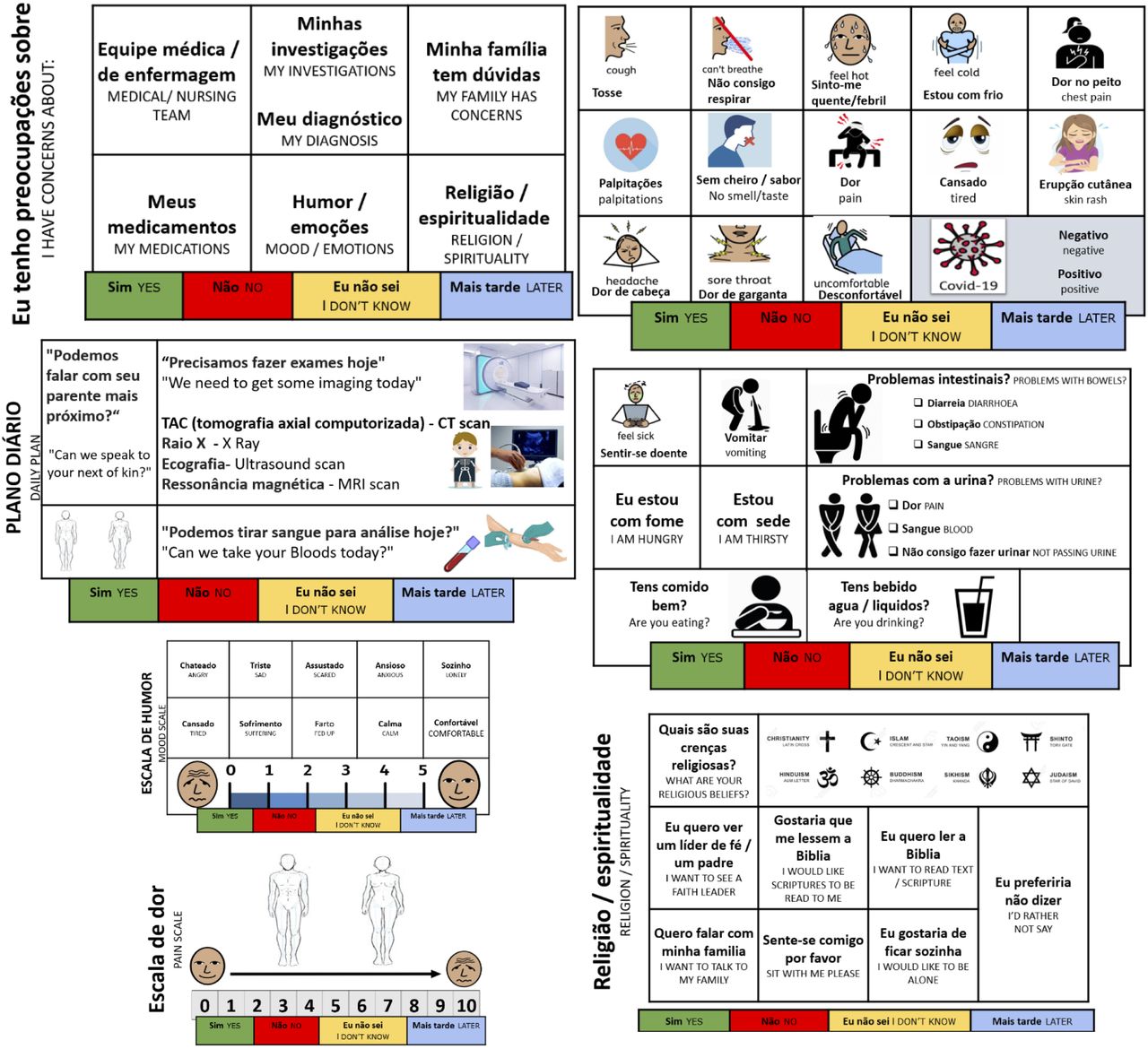
Our communication chart was divided into five sections: patient concerns, current symptoms and systems review, pain scale, mood scale and religion/ spirituality. We translated the charts into ten commonly spoken languages using a free online translation service, and had the translations checked by staff at the hospital. We trialled it on both COVID and non-COVID wards over a 2-month period.
Inclusion criteria: included patients who spoke limited or no English who were not confused nor delirious and who verbally consented to patient questionnaires before±after implementation of the communication chart. The 10 languages were Arabic, Chinese, French, Hindi, Polish, Portuguese, Romanian, Spanish, Turkish and Urdu. Characteristics of participants in each Plan–Do–Study–Act (PDSA) cycle are shown in online supplemental table 1.
Supplemental material
We initially designed and conducted a questionnaire assessing how patients who did not speak English as a first language found communication on the ward round. These included 5-point Likert scales from very ineffective to very effective as well as free text boxes. These questionnaires were conducted using family as translators, telephone translation services and online translation apps.
Figure 1 shows an example of the Portuguese communication chart after PDSA cycle 3.

Example communication aid intervention.
Strategy
We conducted baseline questionnaires (n=8) on patients who did not speak English as their first language assessing how they found communication on medical ward rounds. This included communicating current physical symptoms, expressing concerns or anxieties, having spiritual or faith needs addressed, being told their diagnosis, understanding their diagnosis and how patients felt we could improve communication on the medical ward round. We also asked doctors to rate how effectively they found communication on the medical ward round with patients who don’t speak English as their first language.
Figure 2 shows an example of prechart and postchart questionnaires.

Example questionnaires pre and post Quality Improvement Project (QIP) intervention.
We conducted three cycles using the Plan Do Study Act (PDSA) template. In our first PDSA cycle, we designed and conducted patient questionnaires on five patients prechart and postchart implementation assessing how patients found communication on the medical ward round including feedback on the readability and content of our communication chart itself. These questionnaires included 5-point Likert scales rating different aspects of communication on the medical ward round from very ineffective to very effective as well as free text answers. During this cycle, we found that we were missing crucial feedback from the medical team on the impact of the communication chart on the medical ward round as well as their feedback on its readability and content.
In our second PDSA cycle, we reflected on missing feedback from the medical team in PDSA 1 and therefore included questions for the medical team about communication on the ward round as well as feedback on the Chart design itself in our prechart and postchart questionnaires.
In our third PDSA cycle, we adjusted our communication charts to include daily investigations and highlight family concerns responding to feedback from PDSA 2.
Results
In our baseline questionnaire (n=8 patients), all eight patients agreed or strongly agreed that the medical team understood their current physical symptoms, seven of eight agreed or strongly agreed the ward round addressed their concerns or anxieties as well as ongoing needs. Seven of eight patients reported they had been told their diagnosis of which six understood their diagnosis. Patient suggestions for improving communication on the medical ward round included using a formal interpreter, using family members as interpreters or communication aids. Only two of eight doctors felt they were able to communicate effectively with patients who did not speak English as their first language.
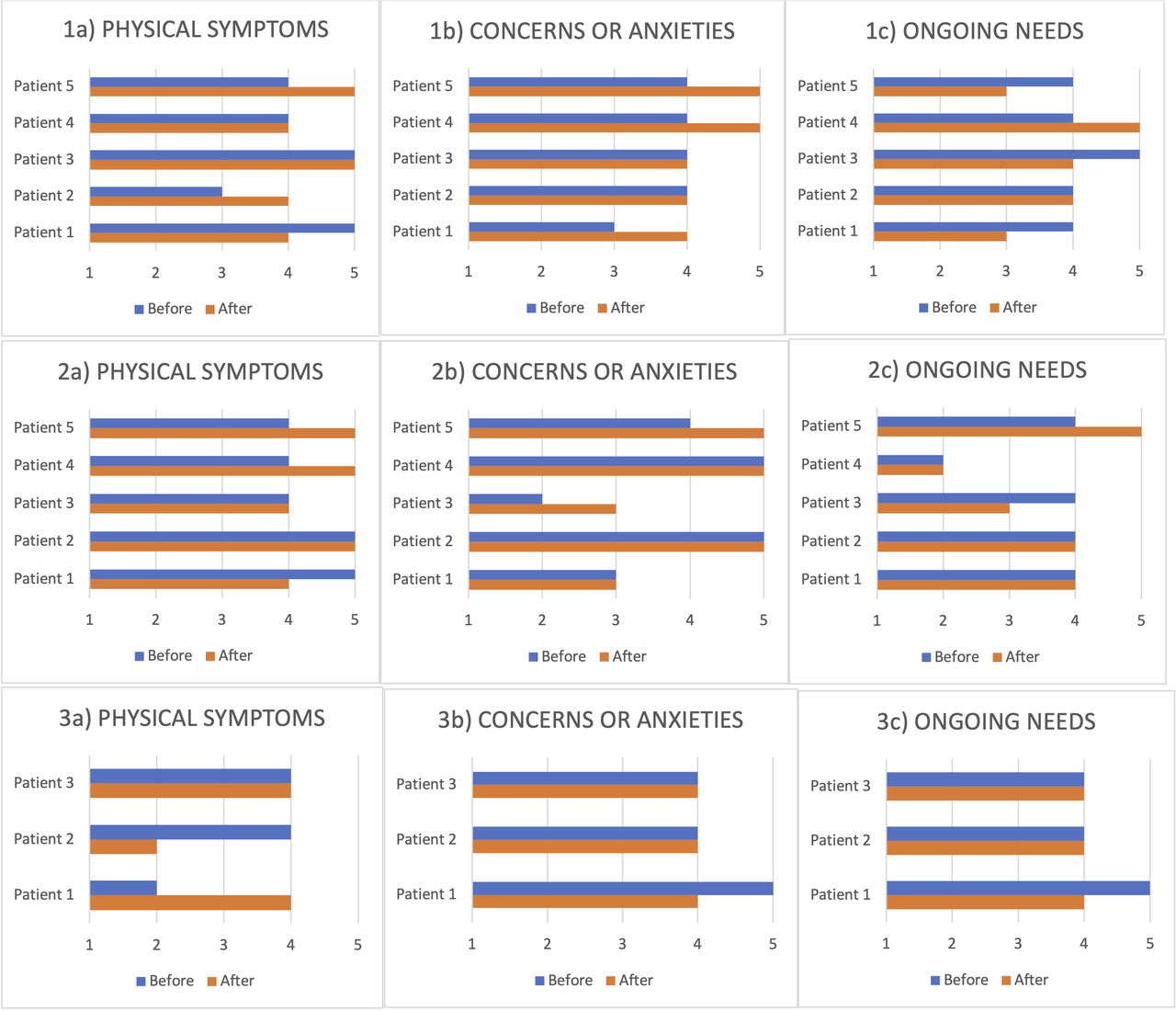
During PDSA 1 (n=5 patients), four of five patients agreed or strongly agreed that the ward round addressed their physical symptoms, concerns or anxieties pre chart implementation with five of five postchart implementation. However, five of five agreed or strongly agreed that the ward round identified and addressed their ongoing needs prechart implementation with three of five postchart implementation showing a worsened outcome (figure 3 shows results for all PDSA cycles). No patients had spiritual or faith needs they felt were relevant to be addressed. Three of five patients reported they had been told their diagnosis of which all understood their diagnosis. Patient suggestions for further improving communication on the medical ward round included easy access to the communication chart and a face-to-face interpreter.
{kind=link}
{kind=link}
{kind=link}
Results of pre and post intervention questionnaires.
During PDSA 2 (n=5 patients), five of five patients agreed or strongly agreed that the ward round addressed their physical symptoms prechart implementation with two of five patients reporting increased satisfaction postchart implementation. Three of five patients strongly agreed or agreed that the ward round addressed their concerns and anxieties with two of five patients reporting increased satisfaction postchart implementation. There was no change in patient experience of the ward round identifying and addressing ongoing needs with chart implementation. Patient suggestions for improving communication on the medical ward round included nursing/medical staff members as interpreters, more in-depth English phrases to be provided on the communication chart especially with explaining mood and emotions.
In PDSA 3, two of three doctors reported improved satisfaction in communication on the medical ward round postchart implementation.
Doctors feedback
In PDSA Cycle 2, four of four doctors interviewed felt the charts were easy to use, readable with a clear lay out. Three of four doctors felt the chart covered all relevant ward round topics with one doctor suggesting covering daily investigations such as bloods and imaging. Feedback included that the charts were particularly useful in the early stages of treatment or when the hospital’s telephone translation service or patient relative was not available; and in identifying areas the patient would like to talk about, for example, the chest pain symbol prompted a conversation about cardiology follow-up. Doctors’ suggestions for further improvement of communication on the ward round included using telephone translators, access to a Wi-Fi phone and being open to the patient’s input. Doctors’ suggestions for improving our communication chart included promoting usage within the medical and nursing teams and adding sections for family concerns and daily investigations required, for example, bloods and imaging.
Free-text feedback was extremely positive with all four doctors feeling the communication chart helped communication on the medical ward round.
Based on PDSA 2 feedback, we added a ‘Daily Plan’ section to the communication chart including bloods and investigations as well as family concerns.
In PDSA 3 (n=3), there was no improvement in patient satisfaction of communication on the ward round between prechart and postchart implementation, however, two of three doctors reported higher satisfaction in communication using the adjusted communication charts on the medical ward round.
Doctors’ suggestions for improving the communication chart including adding a section to introduce your job role and grade and including body parts on the investigations section. All three doctors felt the charts were readable, easily useable with the correct content, layout and order. One doctor in PDSA three wrote ‘it is rarely possible to get someone who is able to translate [on the ward round]. I often use [an online translation app], but this is not ideal for a number of reasons (dependent on Wi-fi, patients may not find it very accessible, may not be correct translation)’.
Discussion
Our results showed that patient satisfaction and their assessment of communication on the medical ward round improved postchart implementation particularly in the domains of physical symptoms, concerns and anxieties. There was little change in patient satisfaction in identifying ongoing needs precommunication chart and postcommunication chart in PDSA 1, 2 and 3. One possible reason could be that our communication chart is better at initial assessment with targeted phrases and images rather than more complex communication. One patient in PDSA 1 wrote ‘The Communication Chart uses limited language. For me as a competent man with strong communication, this is insufficient. E.g. Mood Scale - if you were to ask now how I feel and I point out ‘angry’, I am still unable to explain why. I can speak basic English and the phrases on the Communication Chart are not new to me’.
This suggests that the medical communication chart might be most useful in those with the lowest English language skills, and highlights the importance of facilitating all types and levels of communication on medical ward rounds using multiple tools.
Overall, free-text feedback from doctors was extremely positive on the helpfulness of translated communication charts in improving communication on medical ward rounds and identifying patient concerns. Verbal feedback from the MDT further confirmed the need for written communication charts due to limitations in accessing telephone, face-to-face and online translation services.
Anecdotally, two patients took their communication chart home on discharge in case of future hospital admissions requiring a communication aid.
Limitations and lessons learnt
The main limitation in this QIP is the small sample size. Due to this QIP method using face-to-face patient and doctor questionnaires, data collection was relatively time-intensive as it was conducted by full-time clinical staff during the pandemic.
We were limited in gathering further data postchart implementation as average patient stays were shorter than 3 days for acute medical patients without delirium and did not allow for follow-up questionnaires at day 3 or day 5 as initially planned. COVID-19 ward visiting restrictions also meant follow-up questionnaires were difficult to conduct. Therefore, all patients who completed PDSA 1, 2 and 3 had only one postchart questionnaire completed.
This QIP did not show overall improvement in patient satisfaction but mixed results for different communication domains particularly with worsened/no change in outcome in the medical ward round addressing ongoing needs. Addressing ongoing needs is a more complex domain than simple information exchange, and further research looking at ways to ensure that all patients are able to express their needs would be useful.
A limitation in the use of such a satisfaction survey is that it aims to measure multiple patient satisfaction measures and it is difficult to practicably summarise these multiple domains under one overall heading of ‘satisfaction’.
Our communication chart is recommended for ward round use only. It is not a replacement for telephone translation services or face-to-face translators which are essential for more detailed history-taking or explaining investigations, managements or diagnoses to patients. Due to the prohibitively high cost of vetting our Communication chart by a translation service, charts available are limited to seven commonly used languages and are currently not proof-read for other languages. Another limitation was that a few patients could not read the translated communication chart due to reduced eyesight limiting readability of the chart or low literacy in their spoken language. In these circumstances, they used the communication charts more as visual aids as pictures were included.
Conclusion
Communication charts tailored to the medical ward round are a low resource, effective and useful communication tool which can be used for daily ward round reviews and in quickly identifying patient symptoms and concerns.
There was improvement in doctors’ satisfaction of communication on the medical ward round postchart implementation. Possible reasons could be that it is a prompt for considering a patient update during busy ward rounds and provides an easy-to-use and accessible resource which does not require prior planning or expert knowledge. Further qualitative work is required to identify the reasons behind this improvement.
Medical communication charts can help in delivering high quality, patient-centred care in multicultural and multilingual healthcare settings within the NHS; in keeping with the GMC’s Good Medical Practice values,15 and are useful as an adjunct to telephone and face-to-face translation services.
Sustainability and spreading our intervention
After completion of our third PDSA cycle, we are undergoing quality assurance of the communication charts in the most commonly used languages at KCH with KCH Trust Staff acting as volunteer proof-readers and seeking funding for professional translation. We plan to laminate the vetted translated communication charts, promote their availability using ward posters and audit the frequency of their use on medical inpatients on the Acute Medical Unit to monitor engagement with the intervention. After this, we plan to promote our communication charts for use across all medical and surgical wards at KCH by publicising them through the All-Staff Bulletin, the Trust homepage and ward managers.
We are seeking funding to expand the languages available, and following quality assurance and governance processes to make the communication chart widely available on the Trust Intranet, available at multiple sites. These communication charts will be free to use and available 24/7 via the Trust Intranet.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Acknowledgments
With thanks to SALT at KCH for providing reference communication charts to develop our own medical communication chart. We would also like to thank the following KCH Trust Staff members for volunteering to proof-read our charts and generously giving their time: Alvaro Canovas, Ali Dogan, Megha Macwan, Ida Meye de Souza, Adriana Recto, Adarsh Sharma and Adina Tomuta.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors ANS, AC and L-JS conceived the QIP design. ANS was QIP lead and was involved in design and implementation of communication charts, selection of patients, design and conduction of prechart questionnaires and postchart questionnaires for three PDSA cycles, performed data collection and analysis; and wrote the primary and subsequent drafts of the manuscript. AC was involved in design of communication charts, design of prechart questionnaires and postchart questionnaires and performed data analysis. L-JS was involved in supervision of QIP and review of manuscript including editing final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.